
Abstract
Objectives: This study evaluated how often patients who reported social risk factors requested assistance with these risks in an integrated health system.
Methods: We examined how self-reports of risk related to stated desire for help with that risk reported during social risk screenings at Kaiser Permanente Northwest (KPNW). We examined how patient characteristics were associated with desire for help with each social risk domain using logistic regression.
Results: Approximately 24% (n = 7,807) of the 32,865 KPNW members aged ≥ 18 years who were screened between June 1, 2017, and December 31, 2019, reported at least 1 social risk. More than half of patients who reported a risk were risk/help concordant (i.e., they also wanted help with that risk). The highest concordance (81.7%) was observed among patients reporting medical financial hardship. Several demographic, health, and other factors were associated with concordance across domains.
Conclusions: Patients do not request assistance for all reported social needs. Our findings could help shape future work examining patients' reasons for not accepting assistance and developing interventions to help patients with high social risk more effectively.
- Financial Stress
- Integrated Health Care Systems
- Logistic Models
- Population Health
- Referral and Consultation
- Risk Factors
- Self-Report
- Social Determinants of Health
Introduction
Socioeconomic status plays a critical role in health1⇓–3 as it underlies adverse social determinants of health (SDoH), also called social risks, such as food insecurity and housing instability. To address the impact of social risks on health, medical and public health organizations recommend systematically collecting and documenting social risks in electronic health records (EHRs),4⇓⇓–7 and many health systems have begun to do so.8
Some health systems that conduct social risk screening are also attempting to respond to patient-reported risks by referring patients with such risks to community-based social service organizations.9⇓–11 While patients are generally accepting of social risk screening,12⇓⇓–15 research shows that uptake of referrals targeting social needs varies widely across contexts, making it difficult for health systems to address these risks.16⇓⇓⇓⇓–21 Explorations of reasons why patients may be reluctant to accept assistance have indicated that low screening validity of tools meant to detect social risks, general lack of interest among patients in receiving assistance from health care organizations, and negative perceptions of social service agencies may play important roles.22 A recent study found that offering assistance before assessing social risks led to higher rates of acceptance of assistance.23 However, more data are needed about factors related to patients' willingness to be connected to resources related to self-reported social risks to identify more effective ways to help these patients.
Better understanding of who accepts help and for which social risk domains is needed for health system-level social risk interventions to be successful. This information can be used to design interventions that connect patients with needed resources and ensure that health system social risk programs can effectively reach those patients who most need assistance. This study examined patients' social risk screening responses, the relationship between self-reported social risks and patients' interest in receiving assistance, and sociodemographic and health factors associated with accepting assistance among patients reporting social risks in a large integrated health care system.
Methods
Study Setting
Kaiser Permanente Northwest (KPNW) is an integrated health care delivery system that provides health care to more than 620,000 members in Oregon and Southwest Washington. In 2017, KPNW introduced an SDoH screening tool called Your Current Life Situation (YCLS).24 The YCLS is a 9-item screening tool that assesses 5 social risk domains: housing instability, food insecurity, transportation hardship, medical financial hardship, and non-medical financial needs (including debt and childcare expenses). There is also a question about activities of daily living, which are not addressed in this manuscript. For each domain, patients are asked both whether they are experiencing hardships in this domain and whether they would like help addressing those hardships (Appendix 1). Answers to the 2 questions are independent: patients can request or decline to request assistance with any domain, regardless of whether they indicated experiencing risk in that domain.
As of July 2018, hospital admission staff have been instructed to administer the YCLS to all patients admitted to the 2 major KPNW hospitals for inpatient care. In the outpatient setting, it is administered mostly by patient navigators to patients who are frequently readmitted to the emergency department, uninsured patients, patients with public insurance, patients referred by their primary care physician to a patient navigator, and patients are seen in the gender health clinic (see Friedman & Banegas 2018 for more details about YCLS administration).25 The YCLS is administered through in-person or telephone interviews by a variety of health care professionals (patient navigators, social workers, nurses, care managers), or self-administered on paper or online.
Study Population
Data came from all KPNW members aged 18 years or older who completed the YCLS between June 1, 2017, and December 31, 2019 (n = 32,865). If a patient completed multiple YCLS screenings, the most recent responses were used. This study was approved by the KPNW Institutional Review Board.
Social Risk Variables
The YCLS assessed the following risk domains: housing instability, food insecurity, transportation needs, and medical financial hardship. The following criteria were used to define each risk:
Housing instability – the patient reported (1) temporarily staying in a shelter or with a friend or relative or being homeless; (2) having concerns about their current living situation, such as housing condition, cost of housing, or lack of permanent housing; or (3) having trouble paying for housing or housing utilities in the past 3 months.
Food insecurity – the patient reported having worried that their food would run out before they could buy more or have had trouble paying for food in the past 3 months.
Transportation hardship – the patient reported that lack of transportation had kept them from attending medical appointments or doing other things they needed for daily living or having trouble paying for transportation in the past 3 months.
Medical financial hardship – the patient reported having had trouble paying for their medical needs in the past 3 months.
The YCLS also included a non-medical financial hardship domain that included childcare costs and debt, but these were rarely identified as hardships by patients; we did not include this domain in our analysis.
Interest in Receiving Assistance/Perceived Social Needs
We created binary variables indicating whether a patient indicated wanting help with a specific social risk domain based on their responses to the YCLS item “Which of the following would you like to receive help with at this time?” Patients could choose from response categories (e.g., food, housing, transportation) or indicate no interest in receiving assistance.
Sociodemographic, Clinical, and Other Variables
We extracted sociodemographic, clinical, and other variables that might impact the decision of a patient to request assistance with social risk domains from the KPNW EHR for each patient who completed a YCLS. These included race/ethnicity collected at patient registration through patient self-report (categorized as Asian, Black, Hawaiian/Pacific Islander, Hispanic, American Indian/Alaskan Native, Mixed Race/Other, Unknown, or White), sex, age (categorized by decade), and insurance status (commercial, Medicare, Medicaid, or uninsured) at the time of the YCLS completion. The Neighborhood Deprivation Index (NDI), constructed based on census tract-level socioeconomic variables,26,27 was also calculated, based on patient addresses documented at the time of filling in the YCLS (a high value indicates higher levels of deprivation). The unweighted Elixhauser comorbidity score, which measures patient comorbidity based on the International Classification of Diseases, Ninth Version, Clinical Manifestation (ICD-9-CM) and Tenth Version (ICD-10) diagnoses, was calculated as described by Elixhauser and colleagues28 and used as a summary measure of health status. We also determined whether another person was present when responding to YCLS questions using information about who filled out the YCLS (patient, family member/friend/caregiver, patient with help) and whether an interpreter was used.
Statistical Analysis
Descriptive statistics were used to report sociodemographic characteristics. Frequencies of reporting a risk and of indicating a desire for help were calculated for each risk domain. We assessed the alignment between patients' reported social risks and their requests for assistance by defining respondents who reported social risks within a domain and requested assistance with that domain as “risk/help concordant,” and those who did not request assistance with a domain where they reported a risk as “risk/help discordant.” Among those discordant in each domain, we further examined whether they requested help in other domains.
Logistic regression was used to examine the association between sociodemographic characteristics and concordance (1 = risk identified and wanted help, 0 = risk identified and did not want help) within each risk domain. All models included age, sex, race/ethnicity, whether or not someone needed an interpreter, insurance type, Elixhauser score (categorical variable), NDI, the person who filled out the YCLS, and reported needs in other domains.
All analyses were done using SAS v9.4.
Results
Population Characteristics
Baseline characteristics of the study population are presented in Table 1. The majority of patients were female (54.3%) and white (82.4%). Approximately two-thirds were older than 60 (60.4%), half had Medicare coverage (51.1%), and half had Elixhauser comorbidity scores higher than 3 (50.9%). Most (76.6%) completed the YCLS themselves; 3.4% had needed an interpreter.
Baseline Population Characteristics (N = 32,861)
Patterns of Help-Seeking
The most commonly reported social risk was housing instability (13.3%), followed by food insecurity (11.1%), medical financial hardship (8.5%), and transportation hardship (7.6%) (Table 1). Respondents were most likely to request help with medical financial hardship (13.6%), followed by housing (8.8%), food (6.4%), and transportation (5.7%). Notably, more patients requested help with medical financial hardship than reported a social risk for this domain.
Overall, more than half of patients who reported having a social risk within each domain were risk/help concordant, also reporting wanting help with that risk (Table 2). The highest concordance was observed for medical financial hardship: 81.7% who reported this social risk also requested help with it. Concordance rates were 59.8% for housing instability, 59.4% for transportation hardship, and 51.7% for food insecurity.
Request for Help Among Patients Who Reported Having Social Risks by Social Risk Domain
Factors Associated with Social Risk/Help Concordance
Several demographic, health, and other factors were associated with risk/help concordance across domains. One common pattern was that variables associated with lower socioeconomic status (SES) (ie, uninsured or on public insurance, high neighborhood deprivation index) were often positively correlated with risk/help concordance across all domains. Patients insured by Medicaid were more likely than those who were commercially insured to be concordant for housing instability (OR, 1.65; 95% CI, 1.34-2.03), food insecurity (OR, 1.37; 95% CI, 1.13-1.67), and transportation hardship (OR, 2.03; 1.57-2.61); Medicaid provides coverage of medical expenses and requires low copays). In some domains, rates of concordance were also higher for uninsured patients (housing instability: OR, 1.29; 95% CI, 1.02-1.63; transportation hardship: OR, 1.58; 95% CI, 1.12-2.23) and patients insured by Medicare (food insecurity: OR, 1.45; 95% CI, 1.15-1.82; transportation hardship: OR, 1.77; 95% CI, 1.30-2.42). Patients living in neighborhoods with greater deprivation (continuous variable) showed higher levels of concordance for housing instability (OR, 1.14; 95% CI, 1.03-1.25), food insecurity (OR, 1.18; 95% CI, 1.01-1.22), and transportation hardship (OR, 1.22; 95% CI, 1.08-1.37). Patients needing an interpreter were more likely than those not needing an interpreter to be concordant for housing instability (OR, 1.52; 95% CI, 1.06-2.17), food insecurity (OR, 1.70; 95% CI, 1.17-2.48), and medical financial hardship (OR, 1.78; 95% CI, 1.00-3.18). Patients receiving assistance from a family member or caregiver in filling out the YCLS were less likely to be concordant for housing instability (OR, 0.70; 95% CI, 0.55-0.89) and transportation (OR, 0.79; 95% CI, 0.58-1.07) than those filling out the survey themselves.
While significance varied across domains, each age group under 80 years was more likely to be concordant for housing instability and food insecurity than those older than 80. Patients aged 18 to 29 years, 30 to 39 years, and 40 to 49 years were more likely to be discordant for transportation hardship (see Table 3). Black, Hispanic, and Hawaiian/Pacific Islander patients were often more likely to be concordant than White patients. For housing instability, Black patients were more likely to be risk/help concordant than White patients (OR, 1.55; 95% CI, 1.21-2.00); for food insecurity, Black patients (OR, 1.44; 95% CI, 1.11-1.86), and Hispanic patients (OR, 1.66; 95% CI, 1.25-2.21) were more likely than White patients to be concordant. For medical financial hardship, Hawaiian/Pacific Islanders (vs White: OR, 3.30; 95% CI, 1.03 to 10.66) had the greatest likelihood of concordance. A significant association was found between risk/help concordance and Elixhauser score (>3) for medical financial hardship (OR, 0.64; 95% CI, 0.43-0.95).
Results of Multivariable Logistic Regression of Risk/Help Concordance by Social Risk Domain
Those who were risk/help concordant in the housing and food insecurity domains had higher odds of reporting risks in all other categories than those who reported these risks but did not ask for help (see Table 3). Patients who were concordant for transportation had higher odds of reporting housing instability than those who were not concordant.
Patterns Across Domains Among Patients Who Were Risk/Help Discordant
Patterns of help-seeking for patients who were risk/help discordant in at least 1 domain are shown in Table 4. Approximately one-third of patients who were discordant in 1 domain asked for help in at least 1 other domain. Patients who were discordant for housing instability, food insecurity, and transportation needs were most likely to request help with medical financial hardship than any other domain (34.6%, 39.3%, and 37.4%, respectively). For those discordant on medical financial hardship, housing instability was the most requested type of help (33.2%); it was also the second most requested type of help for patients who were discordant for food insecurity (32.5%) and transportation needs (34.3%).
Types of Help Requested Among Patients Who Were Risk/Help Discordant
Discussion
In this analysis of social risk questionnaire data from a large integrated health care system, more than half of patients who reported a given social risk indicated that they would like help with that social risk. We found evidence that patients responding to questionnaires in the KPNW in- and outpatient settings were most willing to ask for help with medical financial hardship. While a variety of variables were associated with asking help for domains that patients reported a risk in, there was a general pattern that variables associated with lower SES (eg, lack of commercial insurance, neighborhood deprivation index) were often (though not always) associated with higher rates of asking for help when reporting a social risk.
Our results showed 52% to 82% of patients asking for help with stated needs, depending on risk domain. This percentage is at the high end of the ranges found in the limited prior research.17,29 Studies of food insecurity—the most studied social risk in prior research—show rates of acceptance of help or enrollment in food assistance programs between 8% and 75%.16,30⇓–32 For other risk domains, requests for help with reported social risks between 3% and 21% have been documented.18,20 The only other study on requests for help by risk domain, set in an urban health clinic for young adults,19 found that patients most commonly requested help with income security (83% of those reporting a risk requested help), education (56%), and nutrition and fitness (50%). Consistent with this prior research, our results showed that patients' requests for help varied considerably by risk domain. This finding may be due to various factors: what needs patients see as most urgent or pressing, their understanding of what help is available, and the ongoing support they may already be receiving.
The most common domain in which help was requested was medical financial hardship. This finding is reflected in the high overall concordance rate and the number of patients who requested assistance with medical financial hardship while not reporting a risk in this domain. This suggests patients' requests may be context-dependent: requesting assistance with medical financial hardship in a health care context may have seemed more practical than requesting help with food insecurity. Expanding existing programs33,34 that offer assistance with paying medical bills may be an effective way of supporting all patients, regardless of reported social risks.
Factors associated with risk/help concordance included being on Medicaid or Medicare rather than commercial insurance, race, and need for interpretation. These results suggest that targeted outreach strategies may be needed to reach all populations who need assistance with social risks effectively. Medicaid insurance status was significantly associated with higher odds of risk/help concordance for all domains except medical financial hardship, presumably because patients with Medicaid insurance typically do not have copays in the integrated delivery system. Higher neighborhood deprivation was significantly associated with risk/help concordance for housing instability, food insecurity and transportation hardship. Income, poverty level, and public assistance are key elements of the NDI: those with high NDI may thus have been more likely to be a Medicaid recipient and therefore less likely to need assistance with medical financial hardship. Patients aged 18 to 29 years, 30 to 39 years, and 40 to 49 years were less likely to request help with transportation than those aged 50 years and older, most likely indicating a greater level of mobility among patients younger than 50.
Another recent study found that the number of self-reported social risks, as well as the order in which interest in receiving assistance and reporting social risks was assessed, were both associated with uptake of assistance among those screened for social risks.22 This finding points to the importance of the screening tools used to assess interest and detect social risks. Psychometric data for social risk screening tools are limited, and little is known about the validity and reliability of these tools.35 In our study, we found that some patients reported social needs without indicating social risks. This result is consistent with findings of some previous studies showing that more patients requested assistance than reported social risks.22,30 This may be related to the sensitivity of the tool to discover social needs,23 or patients' perceptions of which domains may be most appropriate for requesting assistance, regardless of risks.
Our results provide new insights into variables associated with patients accepting or not accepting assistance with reported social risks. They also demonstrate the limitations of relying on a quantitative analysis only to understand why patients do or do not accept assistance. Gaining a deeper understanding of these reasons would require engaging with patients in follow-up research to learn about their opinions, interests, and reasons for accepting or rejecting help. Ultimately, learning more about patients' perspectives is needed to inform health systems' SDoH program planning efforts and to design targeted interventions that empower as many patients as possible to receive the assistance they need.
Limitations
Our analysis used data from all KPNW patients aged 18 years and older who completed an SDoH assessment tool: primarily those admitted to inpatient care or patients who worked with patient navigators; results are generalizable to patients with similar characteristics. However, the study population is a subset of the KPNW membership and may not represent the entire patient population. As an integrated health system, KPNW may differ from other settings in its resources or inpatient perceptions when considering seeking help, so findings may not be generalizable across all health care settings. Additional variables that were not included in our analyses for various reasons may play a role in a patient's decision to request help. We decided a priori to exclude outpatient versus inpatient setting as an additional variable. Variables such as household size or income are not available in the EHR and therefore could not be included; accordingly, we used the NDI as an indirect measure of these variables.
Like most other social risk screening tools,35 the YCLS has not been assessed for reliability, and responses may also be subject to desirability bias. It was, however, developed through a rigorous process that included stakeholders from health care systems, public health, and community-based organizations.24,36 Obtaining psychometric evidence of social screening tools should be an urgent research priority. Finally, the observational study design limits our ability to make causal conclusions about the study results.
Conclusion
In this study of a large, diverse population of patients from an integrated health care system who completed a social risk screening tool, most patients who reported experiencing social risks in 4 domains also reported wanting help addressing those risks within each domain. Medical financial help was prioritized by patients in our medical setting, and several sociodemographic factors were associated with risk/help concordance. Our findings of the factors related to risk/help concordance can help shape future work that more deeply examines patients' reasons for not requesting help.
Appendix
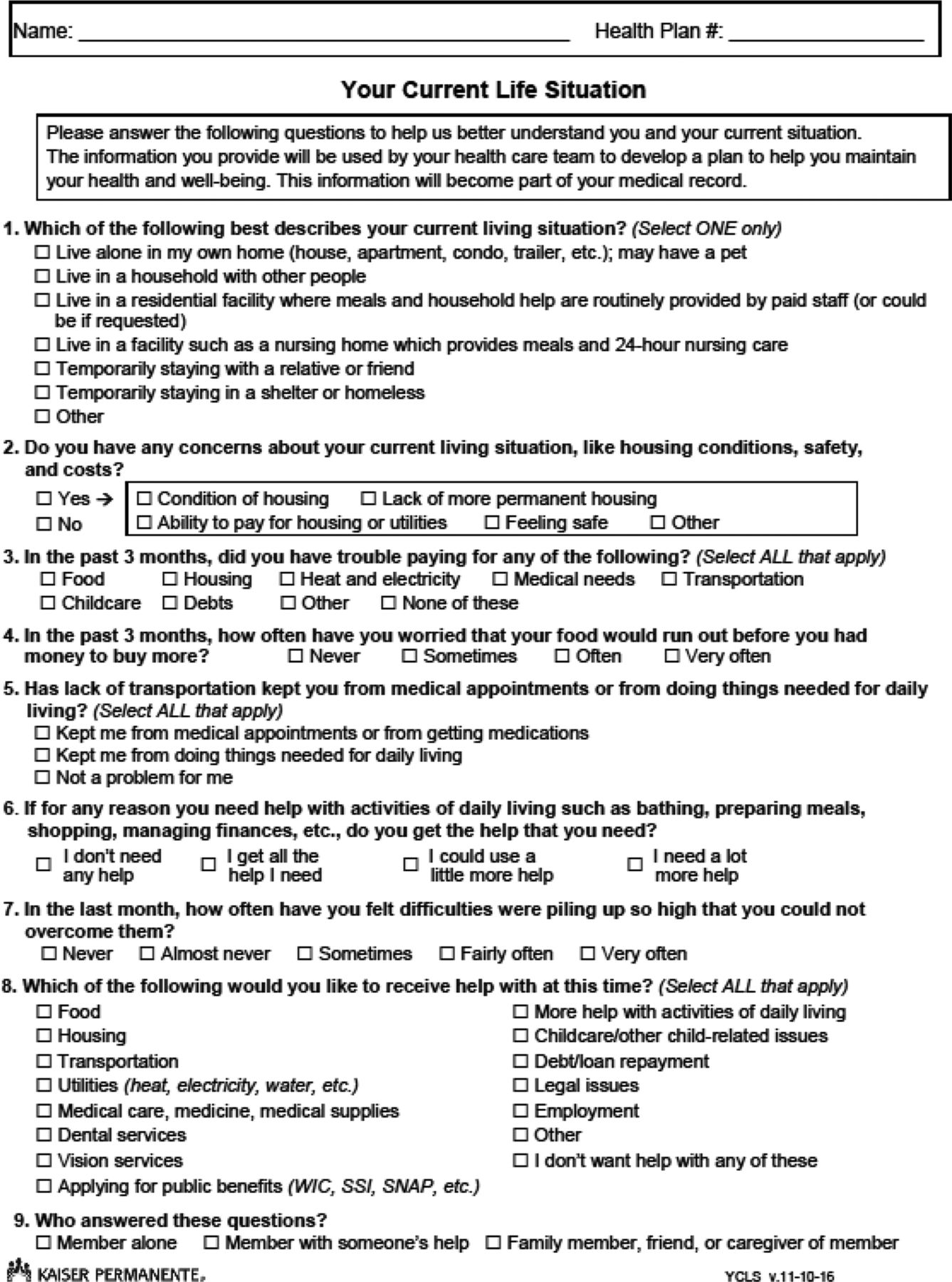
Your Current Life Situation Screening Tool
Notes
Funding: No funding was received to support this study.
Conflict of interest: MPB reports grants from AstraZeneca and Pfizer outside the scope of the submitted work. No other financial disclosures were made.
To see this article online, please go to: http://jabfm.org/content/34/5/914.full.
- Received for publication February 19, 2021.
- Revision received June 3, 2021.
- Accepted for publication June 4, 2021.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Factors Associated with Patient Engagement in a Health and Social Needs Case Management Program
- Food Insecurity Screening in Safety-Net Clinics in Los Angeles County: Lessons for Post-Pandemic Planning
- Food Insecurity Screening in Safety-Net Clinics in Los Angeles County: Lessons for Post-Pandemic Planning
- Leveraging Integrated Primary Care to Address Patients' and Families' Unmet Social Needs: Aligning Practice with National Academy of Sciences, Engineering and Medicine Recommendations
- Practical Clinical Topics, Digging Deeper into COVID-19, Social Determinants of Health, and Equity