
Abstract
Introduction: Rib series are frequently ordered for ambulatory patients who complain of rib pain or have suffered chest trauma. However, the utility of rib series has been questioned in previous studies. The objective of this study was to compare the efficacy of rib series to a single view posteroanterior chest radiograph in the clinical management of most ambulatory patients with rib pain.
Methods: We reviewed all rib series for rib pain performed between January 1, 2016 and December 31, 2016, excluding patients with suspected bony metastasis, chest or rib deformities, and follow-up studies for prior rib series. We recorded any follow-up imaging and/or surgical intervention within 30 ± 7 days, fracture diagnosis, and complications relating to rib fractures.
Results: One thousand seven hundred ninety-one rib series were performed during the study period. Of these, 1168 (65.2%) rib series were performed because of trauma as reported in the clinical indication (trauma cohort). Six hundred twenty-three (34.8%) of the rib series were performed for clinical indications which did not specify acute trauma (nontrauma cohort). There were 323 (17.9%) rib series that resulted in a fracture diagnosis and 95 (5.3%) that resulted in a possible fracture diagnosis. There were 50 (2.8%) effusions, 7 (0.4%), pneumothoraces, and 1 (0.1%) hemothorax detected. Two patients, 1 each from the trauma and nontrauma cohorts, underwent subsequent intervention during the follow-up period. In both cases, the findings which led to the subsequent intervention could be seen on the initial posteroanterior chest radiograph.
Conclusion: Single-view chest radiograph provides sufficient information for the clinical management of ambulatory patients with rib pain.
Introduction
Rib series are frequently ordered for ambulatory patients who complain of rib pain or have suffered chest trauma. However, the utility of rib series in such patients has been questioned in previous studies1,2 because they do not seem to affect the clinical management when compared with the findings of a single posterior-anterior (PA) chest radiograph. In addition, only a small percentage of rib fractures result in a complication. At a time when unnecessary radiation exposure, inefficiency, and additional costs to patients are being scrutinized, rib series for most patients should be avoided.
This study examined whether the 1-view chest radiograph is sufficient for the clinical management of ambulatory patients presenting with rib pain. We predicted that chest PA radiograph would detect any pertinent complications requiring surgical/percutaneous intervention.
Materials and Methods
The Institutional Review Board approved this study with a waiver of informed consent since it is a data-only retrospective investigation with no patient interactions. We reviewed the reports of all rib series for patients with rib pain between January 1, 2016 and December 31, 2016 who subscribe to a geographically isolated Health Maintenance Organization in which all inpatient and outpatient encounters are documented in an electronic medical record. All patients were referred from an outpatient or acute care clinic or the emergency department. However, none of these patients had suffered acute major trauma as the emergency department associated with this Health Maintenance Organization does not accept level-1 trauma patients. We excluded rib series ordered for patients with known or suspected cancer in whom a rib metastasis was suspected; patients with rib or chest abnormalities suggested on physical examination; and patients undergoing repeat rib imaging obtained in the 30-day follow-up period.
We reviewed the clinical indications for the rib series. Those who specifically reported a recent history of trauma including cough were designated as belonging to a trauma cohort. Those patients for whom the clinical indication did not specifically mention trauma were designated as belonging to a nontrauma cohort. This cohort included those patients for whom the clinical indication described such symptoms as acute or chronic rib pain without known trauma, chest pain, back or flank pain, or chest tenderness.
Rib series included a minimum of 2 oblique rib radiographs and a PA chest radiograph. For each patient, we collected data on age, gender, and any follow-up imaging and/or surgical intervention within 30 ± 7 days. For each imaging study, we recorded the reported findings related to rib fractures including the fracture diagnosis, number of fractures, pneumothorax, hemothorax, or effusion. For each case of subsequent surgical intervention or chest tube placement, we investigated the relation of the intervention to rib fracture(s), if any, as well as whether cause for the intervention could be ascertained exclusively from the PA chest radiograph. All patients who did not undergo surgical/percutaneous intervention relevant to their rib pain were deemed to have “conservative management.”
We compared the gender and age distributions among patients undergoing rib series for trauma and nontrauma related rib pain. We also compared the prevalence of fractures and gender distribution in patients undergoing rib series for trauma- versus nontrauma-related rib pain.
One of the authors, who is a practicing radiologist, reviewed all the images from those patients with pleural fluid or pneumothorax to determine if the complicating finding could be identified on the PA chest radiograph alone.
Continuous variables were analyzed with a t-test. Nominal variables were analyzed with a chi-squared test. Statistical significance was determined to be P ≤ .05.
Results
There were 1953 rib series performed during 2016 calendar year based on our review of the electronic medical record. Figure 1 delineates the number and reason for patient exclusion. There were 72 rib series ordered for patients in whom bony metastases were suspected. This included 6 patients who had recent abnormal bone scans and 8 patients with an abnormality seen on recent chest radiograph. There were 6 rib series ordered to assess for chest or rib deformities. This included 3 patients who were noted to have a “chest wall deformity,” 2 patients with suspected bony rib growths, and 1 patient with protruding ribs. Finally, 84 rib series were ordered as follow-up studies for prior rib series ordered within 30 ± 7 days. The results from these studies were not included in the analysis. Therefore, we reviewed 1791 rib series, which were performed on 878 men and 913 women. As shown in Table 1, the average age was 55.2 ± 19.4 years (range, 6 to 102 years) with women significantly older than men (t-test, P < .001). There were 1168 rib series for which the cause of the rib pain was trauma; the 603 men and 565 women had an average age of 56.4 ± 20.8 years. There were 623 rib series for which the cause of the rib pain did not specifically mention trauma; the 275 males and 348 females had an average age of 53.1 ± 19.1 years. The women were older than men in both the trauma (t-test, P < .001) and nontrauma (t-test, P < .001) populations. There were significantly more women than men in the nontrauma cohort as compared with the gender distribution in the trauma cohort (χ2, P < .01).

A flowchart description of rib series patients included and excluded from analysis.
Patient Characteristics in Trauma and Non-Trauma Cohorts
Three hundred twenty-three rib series had a diagnosis of at least 1 rib fracture. There were an additional 95 rib series which reported at least 1 possible rib fracture, resulting in an overall total of 418 subjects with definite or possible rib fractures (23.3%).
Among the 418 patients with definite or possible rib fractures, the average age was 62.1 ± 19.4 years, which was significantly older than those without rib fractures 53.2 ± 20.0 years (t-test, P < .001).
There were 94 patients who had 2 or more definite or possible rib fractures, ranging in number from 2 to 7 fractures: 58 patients had 2 rib fractures; 24 patients had 3 rib fractures; 7 patients had 4 rib fractures; 2 patients had 5 rib fractures; 1 patient had 6 rib fractures; and 2 patients had 7 rib fractures. For 1 of the patients with 7 rib fractures as well as the patient with 6 rib fractures, the reports stated that all the fractures were healed or healing and no further imaging was performed and patients were treated conservatively. In the other patient with 7 rib fractures, a small pneumothorax and pleural effusion were also noted. This 67-year-old woman had subsequent rib series and chest radiograph, which showed stable fractures and effusion with decreased pneumothorax and was also treated conservatively. All but 1 patient of the remaining 91 patients were managed conservatively with no intervention performed for a minimum of 30 days after their rib series. Only 1 patient, a 93-year-old woman with 5 rib fractures and a small effusion did not have a minimum of 30 days of clinical followup. According to the electronic medical record, the physician who ordered the study did have a telephone conversation with the patient explaining the findings and letting her know to come to the clinic for any worsening symptoms. No further office visits are recorded.
As shown in Table 2, there were 343 definite and possible fractures among the 1168 patients (29.4%) in whom trauma was the etiology for rib pain. This compares to the 75 definite and possible rib fractures among the 623 patients (12.0%) in whom trauma was not mentioned as the primary etiology for rib pain. Therefore, there was a significantly greater number of fractures or possible fractures in the trauma cohort than in the nontrauma cohort (χ2, P < .001).
Fracture Rates in the Trauma and Non-Trauma Cohorts by Gender
For both the trauma and nontrauma cohorts, women with definite or possible rib fractures were significantly older than men. In the trauma cohort, the average age for women was 66.6 ± 18.8 years versus 59.1 ± 19.8 years for men. In the nontrauma cohort, the average age for women was 66.0 ± 17.2 years versus 53.8 ± 18.0 years for men.
There were 133 trauma patients (11.4%) who underwent follow-up imaging within 1 month. There were 39 nontrauma patients (6.3%) who underwent follow-up imaging within 1 month.
Additional imaging findings reported on the rib series included 7 pneumothoraces, 50 effusions, and 1 hemothorax. Of the 7 patients with a pneumothorax, 6 also had a rib fracture. In 5 of the 6 patients with an associated rib fracture, the pneumothorax could be readily identified on the PA chest radiograph. In a 63-year-old man with nondisplaced fractures of the right third, fourth, and fifth ribs, a tiny apical pneumothorax was reported but could not be identified on any of the images by the reviewing radiologist. The patient had a follow-up PA and lateral chest radiograph the next day that did not report a pneumothorax. The 1 patient without a rib fracture was a 45-year-old man who injured himself while skateboarding. A small left apical pneumothorax was seen on the PA chest radiograph of the rib series by the reviewing radiologist. None of the patients with a pneumothorax and rib fracture underwent subsequent surgical/percutaneous intervention. Of the 51 patients with an effusion or hemothorax described on their rib series, 42 had an associated rib fracture. In all but 1 patient, the pleural fluid could be identified on the PA chest radiograph by the reviewing radiologist. In a 74-year-old woman with a single mildly displaced ninth rib fracture, a trace effusion could only be seen on 1 of the 3 oblique views of the right ribs. There were 3 patients with 1 rib fracture and 1 patient with 2 rib fractures in whom pleural fluid could be seen in the opposite hemithorax from the side of the fracture only on the PA chest radiograph. None of these patients with rib fractures and pleural fluid underwent subsequent surgical/percutaneous intervention.
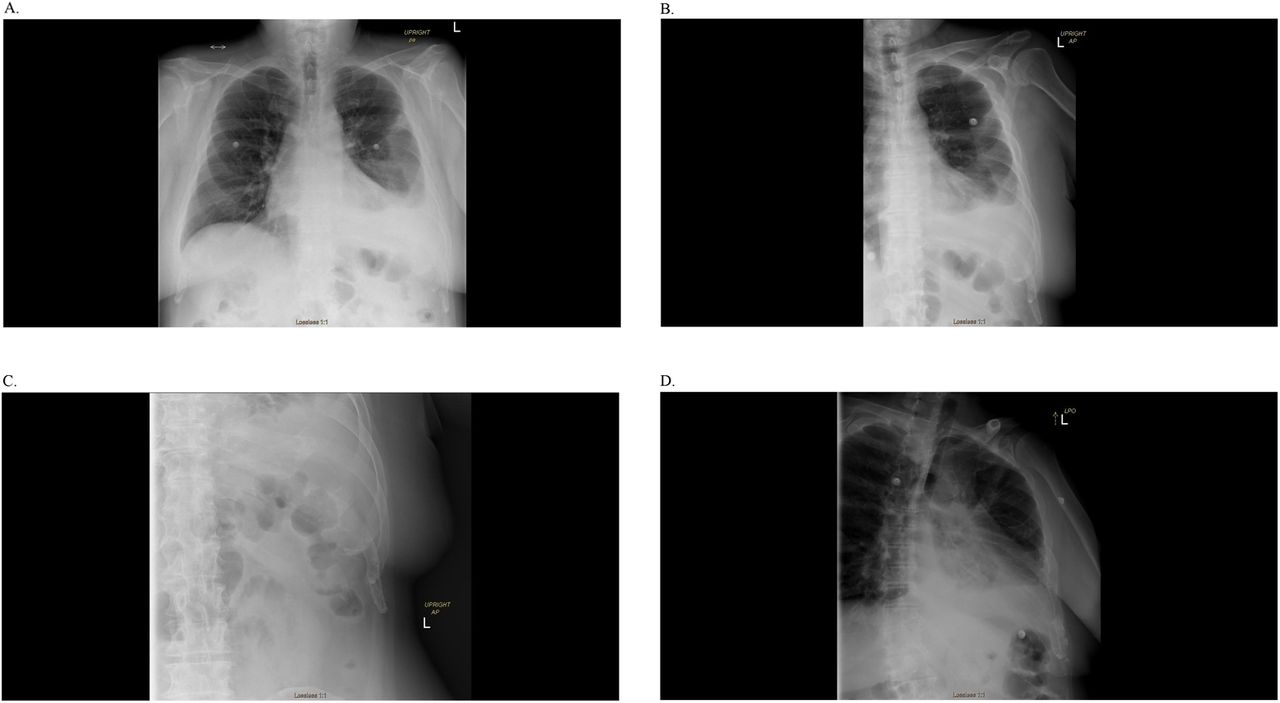
There were 2 patients, neither of whom had a rib fracture who did have a percutaneous intervention within 30 days of their rib series. The first patient was a 60-year-old man with recent trauma but no rib fracture noted to have a small to moderate left pleural effusion (Figure 2), which could be readily seen on PA chest radiograph. He underwent percutaneous left chest tube placement for the effusion 3 days later. The second patient was an 84-year-old woman with rib pain but no mention of trauma noted to have a small effusion seen on the PA chest radiograph of her rib series. She underwent a percutaneous left chest tube placement 5 days later for the effusion because of a left-sided pneumonia and concern for a parapneumonic effusion versus empyema. She did not have a rib fracture. The remaining 1789 patients who underwent a rib series were deemed to have conservative management.
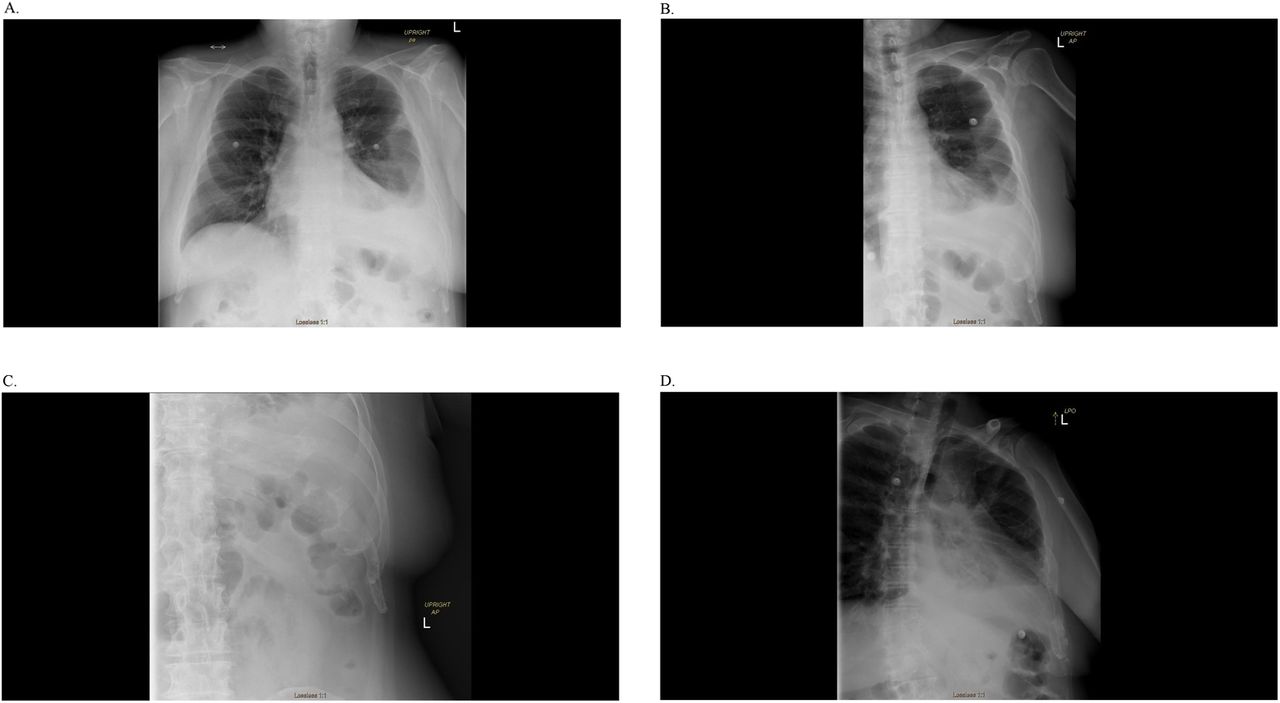
Rib series for a 60-year-old man with recent chest trauma but no rib fractures who subsequently underwent percutaneous chest tube placement for pleural effusion 3 days after rib series images were taken. A, PA chest radiograph demonstrating moderate left pleural effusion, and B–D, oblique radiographs showing no other significant findings.
Discussion
Rib fractures are a common thoracic injury.3 Despite rib series being the initial study chosen for the evaluation of rib pain and rib trauma,2 they rarely provide additional information that affects subsequent clinical management than a single view PA chest radiograph.
While imaging can be used to diagnose rib fractures, it is the presence of associated complications such as hemothorax or pneumothorax that most commonly affect patient management. Without these complications, patients are most frequently treated with conservative therapy.2 Chest radiographs are less accurate at fracture detection than rib series.4 However, a 2014 study found that the clinical management of most patients did not correlate with the presence of rib fractures. Those diagnosed with more than 1 fractured rib (63.1%) were just as likely as those diagnosed with no fracture (64.5%) to receive medical therapy.2 The presence of a complication has been identified as the sole clinically relevant factor that determines the need for surgical intervention.5
PA chest radiographs result in less radiation to patients than rib series. They are also more time efficient and less costly than rib series. The average effective radiation dose is less for a single PA chest radiograph (0.02 mSv) as opposed to a rib series (0.105 ± 0.04 mSv).1 The same study found that the mean turnaround time, that is, from the time when the examination was ordered to when the final report was rendered by a radiologist, to be 61.8 (± 64) minutes for a PA chest radiograph versus 133.5 (± 129.8) minutes for a rib series.1 Finally, the 2020 Medicare global fee reimbursement of a PA chest radiograph is $25.98 while the reimbursement for a unilateral rib series is $41.50.6
The overall rate of rib fractures in our patient cohort is similar to that reported by prior studies of ambulatory patients. Shuaib et al1 evaluated 422 patients, of which 74 (17.5%) had abnormal findings and 30 (7.1%) of those had a complicated finding such as pneumothorax, hemothorax, pulmonary contusion, but only 1 patient required overnight hospital admission and there were no surgical interventions.1 Hoffstetter et al2 evaluated 669 ambulatory patients in a retrospective study, of which 157 (23.5%) had a rib fracture.2 Hemothorax and pneumothorax were diagnosed in 12 (1.8%), of which 6 were missed on the rib series but seen on the chest radiograph. None of their 157 patients required surgical intervention. DeLuca et al7 prospectively evaluated 100 consecutive ambulatory patients referred for rib series. They found 29 patients with a rib fracture, 13 of whom had an associated hemothorax, pneumothorax, lung contusion, and atelectasis. Only 3 of the complications could be detected on the rib series while all 13 complications could be seen on a chest PA radiograph. These authors concluded that the presence of a rib fracture did not influence therapy, but the presence of a complication, such as hemothorax or pneumothorax, did influence therapy in 3 out of 13 cases.
In a more recent study published in 2018, the authors reported rib series as having greater sensitivity for detecting rib fractures as well as a significant positive relationship between the presence of rib fracture and the likelihood of administration of narcotic analgesia.8 We believe that while rib fractures may be correlated with the eventual need for narcotics, the decision to prescribe them should not be based on the presence or absence of rib fracture, but the clinical failure or inadequacy of non-narcotic pain medications to appropriately relieve pain. Of the 339 patients evaluated in the study, 53 (15.6%) had at least 1 fracture. No pneumothoraces, mediastinal widening, or lung contusions were found, and none of the patients required hospitalization.8
With 1791 rib series, our population is much larger than previous studies but the patient populations are similar. Our fracture rate of 23.2% is within the range reported by prior studies (15.6% to 29%).1,2,7,8 While our rate of complicating findings (3.2%) is similar to that of the study by Hoffstetter2 et al, it is significantly lower than that reported by both deLuca et al7 and Shuiab et al.1 However, the interventions in all 3 of the aforementioned studies as well as this investigation are extremely low.1,2,7
There is no gender difference in the prevalence of rib fractures, which was also noted in a prospective study of 699 adults that found no statistically significant difference in the number of fractures between men and women.9 These authors also noted that the median age for fracture among women was significantly older than from men. In this study, women were older than men among all patients receiving a rib series. Women were also significantly older than men among those who suffered a definite or possible rib fracture in both the trauma and nontrauma cohorts.
Patients in the trauma cohort were significantly older than those in the nontrauma cohort. Furthermore, we found that those with a definite or possible rib fracture were likely to be older than those without a fracture. The heightened likelihood of falling in elderly populations may partly contribute to the greater prevalence of rib fracture.9 Furthermore, osteoporosis in the elderly could also be a factor since bone brittleness increases the risk of rib fractures as has been demonstrated in both women and men.10,11
Ultrasound (US) has been shown to be a sensitive method for the detection of rib fractures. In a study of 20 patients with no evidence of rib fracture by radiograph, Turk et al12 found that US could identify a fracture in 18 of these patients. US can also be utilized to demonstrate both pneumothoraces and pleural effusion, which can complicate rib fractures and could change their management.13,14 The additional advantages of US is the lack of ionizing radiation and the ability of this study to be performed in the physicians office rather than having to send the patient to the radiology department. The use of US is likely to increase as more primary care physicians are trained in its use.
Limitations of this study include its retrospective nature and applicability to broader populations. However, a prior small prospective study came to a similar conclusion about the lack of utility of rib series.7 Therefore, it is unlikely that a larger prospective study is necessary to confirm the consistent findings between the previous smaller prospective and retrospective studies and this investigation. The results of the current study should be limited to ambulatory patients with suspected rib trauma or rib pain. Patients who suffer severe trauma are treated differently and often undergo total-body scanning, usually with Computed Tomography in addition to radiography of their extremities. These patients would not benefit from nor would they likely be amenable to a conventional rib series, which requires patients to be able to stand to take the PA chest radiograph and oblique views of the ribs. Finally, suspected child abuse patients may benefit from complete rib series including cone-down images as has been suggested by 2 previous studies to detect and document the findings of intentional child trauma.15,16
The American College of Radiology Appropriateness Criteria recommends PA chest radiograph for patients with suspected rib fracture resulting from trauma.17 Our data suggest that this can be expanded to include patients with rib pain even in the absence of known trauma. We should note that patients with an active cancer diagnosis, suspected cancer, suspicious bony lesions, and prior imaging abnormalities of the ribs may still benefit from a rib series. However, these patients represent a small minority of all patients for whom a rib series was ordered. In this cohort, only 77 (4.1%) patients had an active cancer diagnosis or prior abnormal imaging for which a rib series was recommend.
>The 1791 rib series we reviewed demonstrate that a PA chest radiograph is sufficient to evaluate ambulatory patients with suspected rib fracture regardless of a trauma or nontrauma origin. The complications associated with rib fractures can be readily identified on the chest radiograph as the 2 patients with subsequent percutaneous interventions had effusions that could be detected with the PA chest radiograph. Additional views of the ribs are unnecessary and may burden the patient with more radiation, higher cost, and longer interval for radiology results.
Conclusion
Rib series are unnecessary in the evaluation of ambulatory patients with suspected rib trauma because it does not affect patient management.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: None.
To see this article online, please go to: http://jabfm.org/content/34/1/144.full.
- Received for publication June 4, 2020.
- Revision received August 1, 2020.
- Accepted for publication August 3, 2020.




{kind=link}
{kind=link}