
Abstract
Objective: Although people with severe mental illness (SMI) have high rates of diabetes and other metabolic disorders, adherence to recommended screening guidelines is low. This study aimed to compare primary care clinicians' and psychiatrists' attitudes toward metabolic monitoring and treatment of patients with SMI.
Methods: Primary care clinicians and psychiatrists within 1 large urban integrated public health system were recruited to participate in this online survey study. Multivariate logistic regression analyses were used to examine if clinician characteristics were associated with attitudes or perceived barriers toward metabolic monitoring and treatment.
Results: Response rates were 77% (164/214) of primary care providers and 69% (56/81) of psychiatrists completing the survey. There were no significant differences in age or race/ethnicity between provider groups, although primary care clinicians were more likely to be women when compared with the psychiatrists (69% vs 39%, P < .001). Psychiatrists were more likely than primary care clinicians to believe that psychiatrists should conduct metabolic monitoring even if patients had a primary care provider (80% vs 60%, P = .011) However, fewer psychiatrists than primary care clinicians believed that psychiatrists should treat identified cardiometabolic abnormalities (15% vs 42%, P < .001).
Conclusion: Systemic problems with care coordination and these varying expectations likely contribute to poor cardiometabolic outcomes in this vulnerable population.
- Diabetes Mellitus
- Logistic Regression
- Mental Health
- Mental Disorders
- Metabolic Diseases
- Primary Health Care
- Psychiatry
- Public Health
- Surveys and Questionnaires
- Vulnerable Populations
People living with severe mental illness (SMI; eg, schizophrenia and bipolar disorder) experience premature mortality and die, on average, 25 years earlier than the general population, most often from cardiovascular disease.1⇓⇓⇓⇓–6 In fact, as age expectancy increases, the gap in life expectancy between these groups may actually be widening.6
In addition to multiple lifestyle risk factors, second generation antipsychotic medications can cause metabolic abnormalities, which increase cardiovascular disease risk.7⇓⇓⇓–11 In a meta-analysis, Mitchell et al (2011) found that 1 in 3 patients with schizophrenia suffer from 3 or more cardiovascular risk factors.9 Even in first-episode patients, studies have shown increases in weight12⇓⇓–15 and cholesterol levels,12,13 within the first 9 to 12 months of treatment. Early screening is particularly important, as rates of metabolic syndrome seem to increase with age and duration of illness.9
Unfortunately, cardiovascular risk factors are likely to be underdiagnosed and undertreated among individuals with SMI.16⇓–18 Even during medical or surgical hospitalizations where risk factors for cardiovascular disease, such as obesity and smoking, were identified, people with SMI received fewer diet consults and smoking cessation interventions when compared with nonpsychiatric populations.18 In addition, these people with SMI were less likely to be diagnosed with laboratory-confirmed cardiovascular risk factors than their nonpsychiatric counterparts, even when controlling for demographic variables.18
There have been national efforts to reduce cardiovascular morbidity and mortality by encouraging screening, monitoring, and treatment of people who take antipsychotic medications.19⇓⇓–22 The American Association of Clinical Endocrinologists include the diagnosis of schizophrenia as a risk factor for prediabetes and diabetes mellitus.33 The American Diabetes Association has even mapped out standard procedures for screening patients with SMI as part of their routine medical care.19 These guidelines recommend baseline screening and continued metabolic monitoring of body mass index, waist circumference, blood pressure, fasting blood glucose, and fasting lipids.19,20 Despite these guidelines and psychiatrists' acknowledgment of their importance, monitoring rates continue to be low.23⇓⇓–26
This lack of metabolic monitoring raises the issue of accountability. Our prior work has examined the beliefs of community primary care clinicians and psychiatrists, respectively.27,28 In this article, we compare these responses from within an integrated public delivery system. To our knowledge, this is the first survey study to compare opinions of 2 key specialties regarding whose role it is, or should be, to monitor and treat metabolic abnormalities among people with SMI.
Methods
Setting and Sample
All primary care clinicians (physicians, nurse practitioners, and physician assistants) and psychiatrists were approached from safety-net clinics in 1 large urban integrated public health system. The system includes clinics operated by the public health department and by affiliated community health centers. The primary care and mental health clinics do not share electronic health records. Clinician participants were surveyed between December 2009 and February 2011.
Study Procedures
The recruitment methods for psychiatrists and primary care clinicians have been described previously.27,28 Briefly, clinicians were offered an opportunity to participate in an anonymous survey about metabolic monitoring of people taking antipsychotic medications. Potential participants were contacted by a research coordinator and asked to complete a survey either on article or online. The survey was distributed to the psychiatrists first and was adapted for the primary care clinician sample. To meet inclusion criteria, a provider must have (1) primarily treated adults and (2) spent 5% or more of their time in direct patient care. A $5 gift card was offered to all respondents regardless of survey completion. Follow-up e-mails were sent 2 weeks after initial survey distribution. Study procedures were approved by the University of California, San Francisco Committee on Human Research (number 10–03254).
Measures
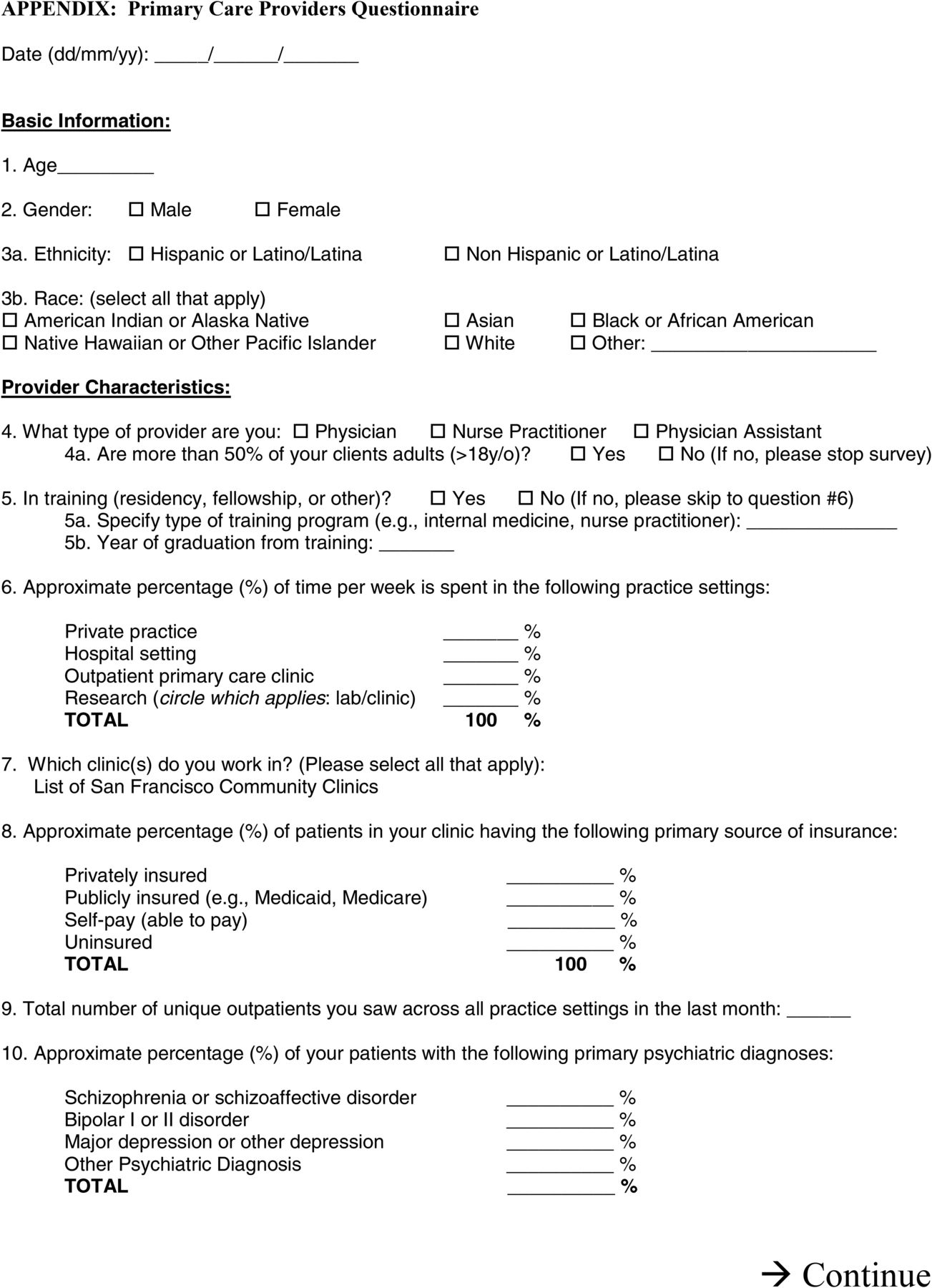
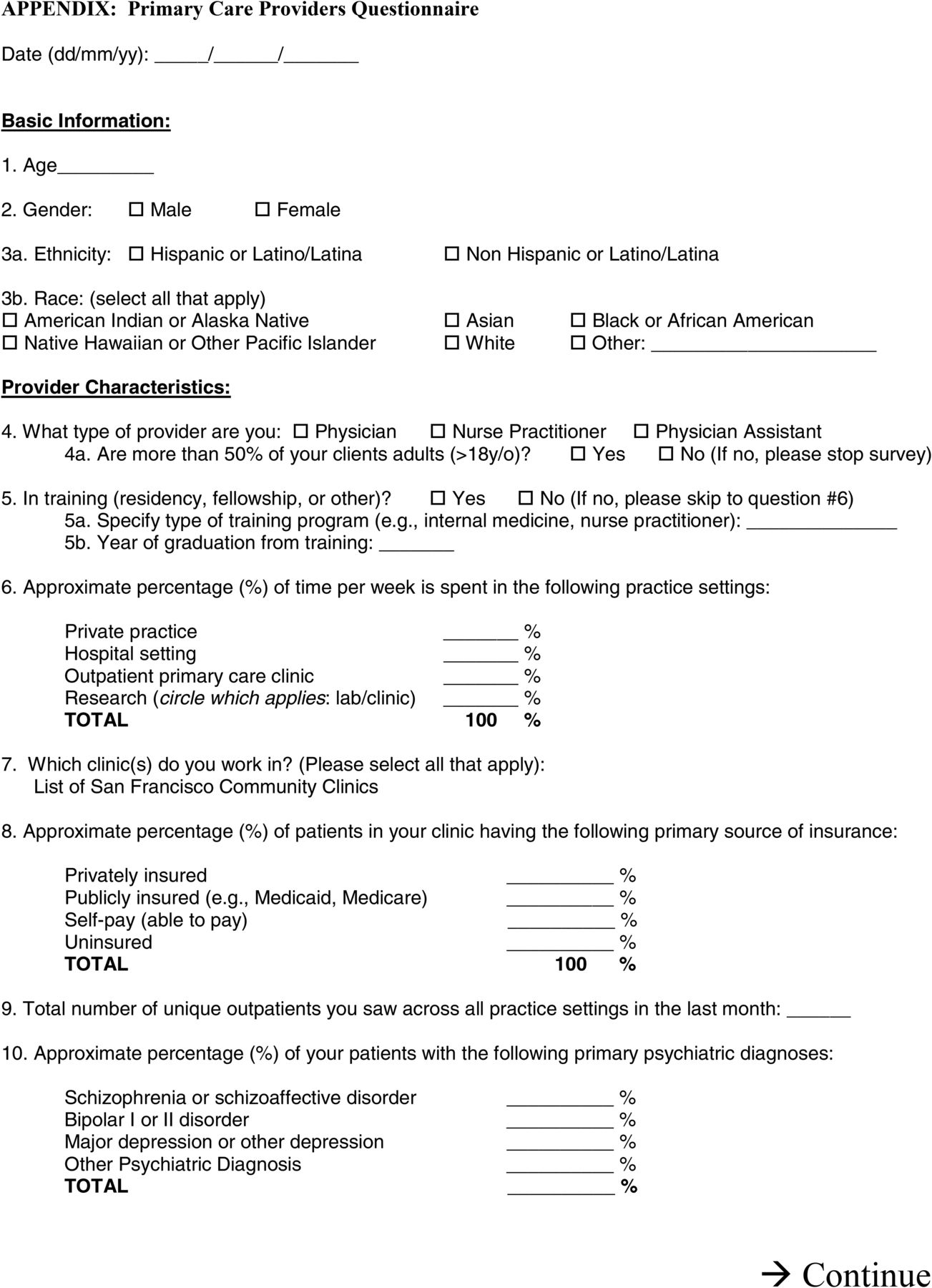
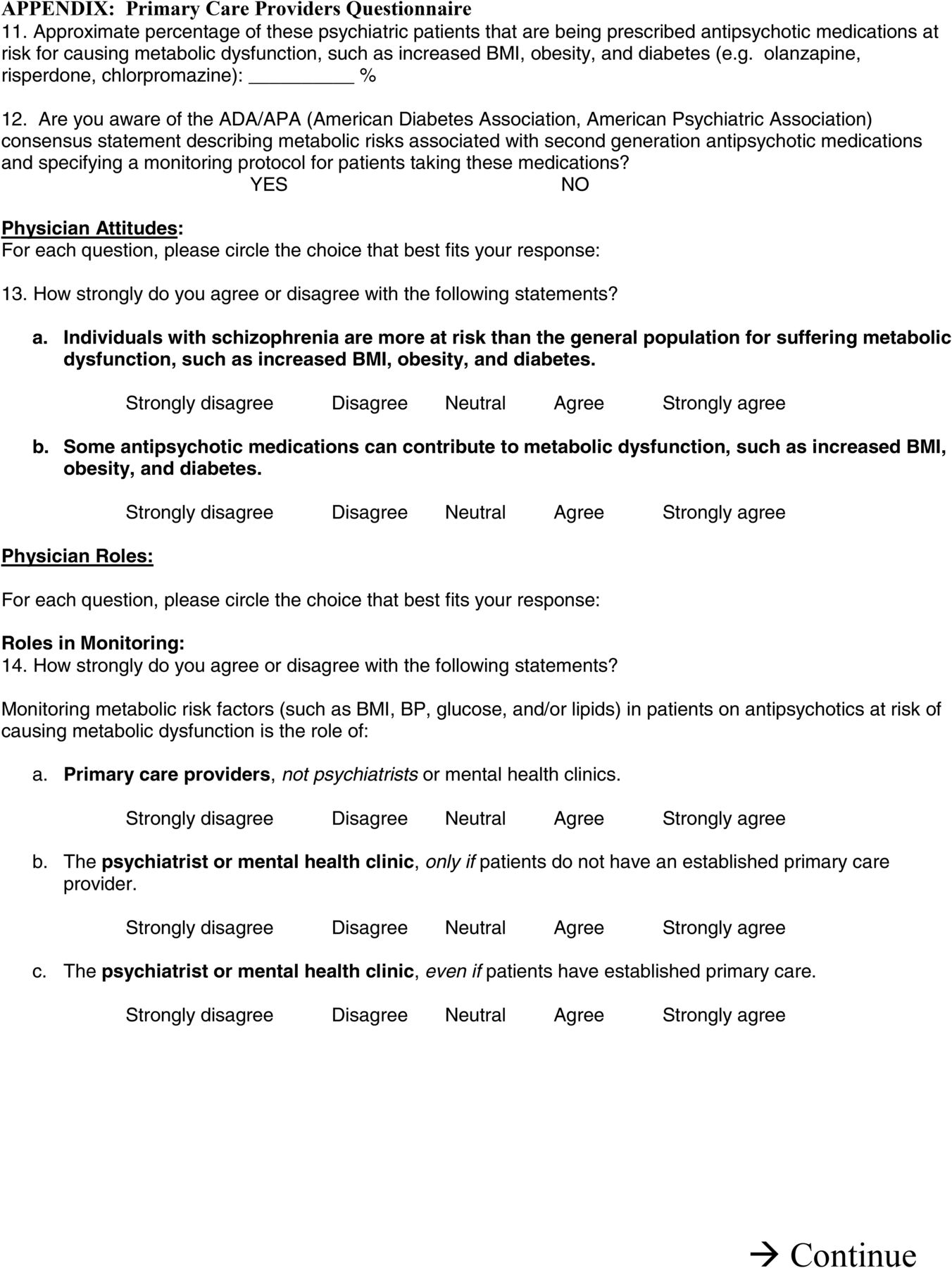
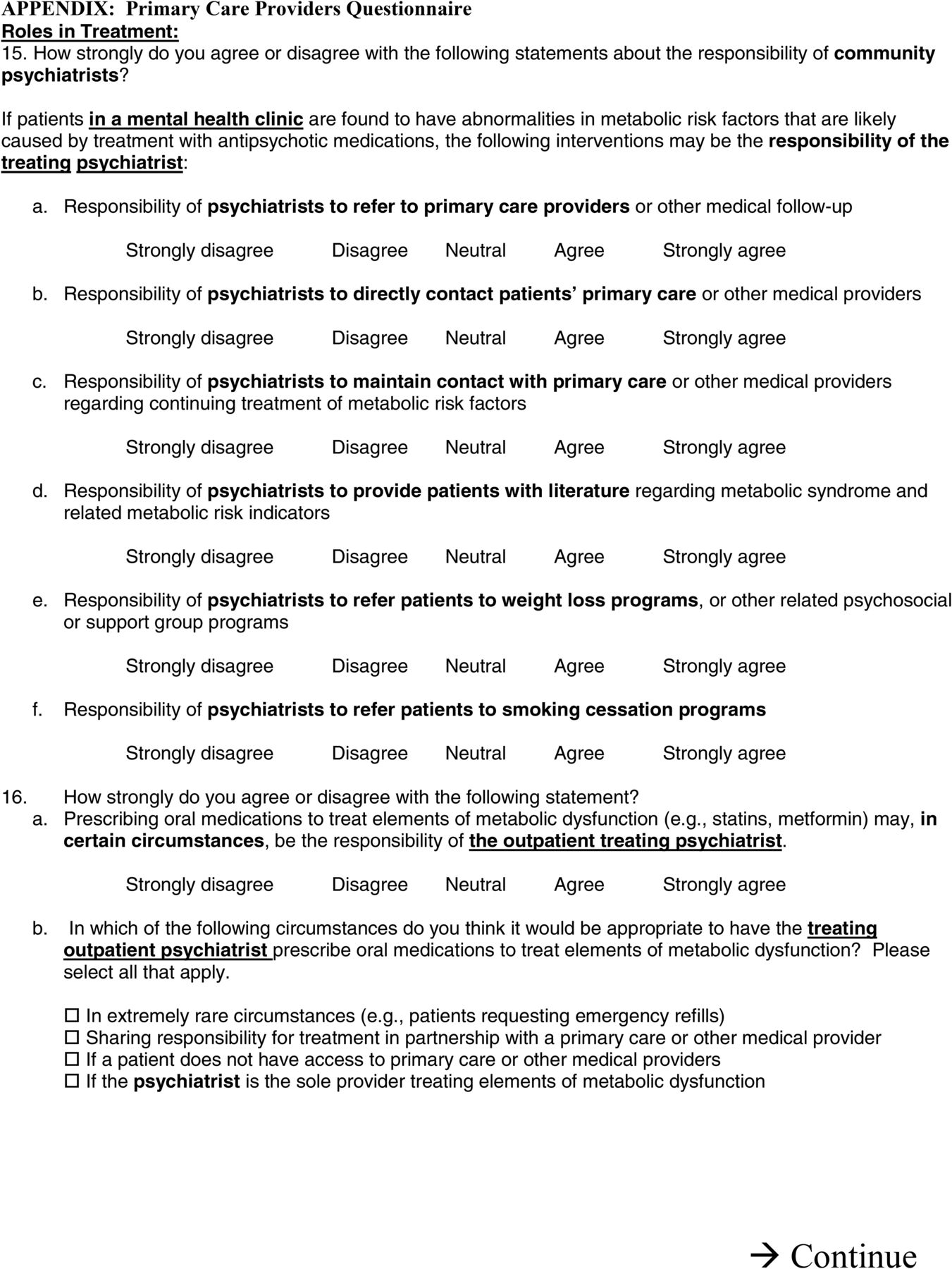
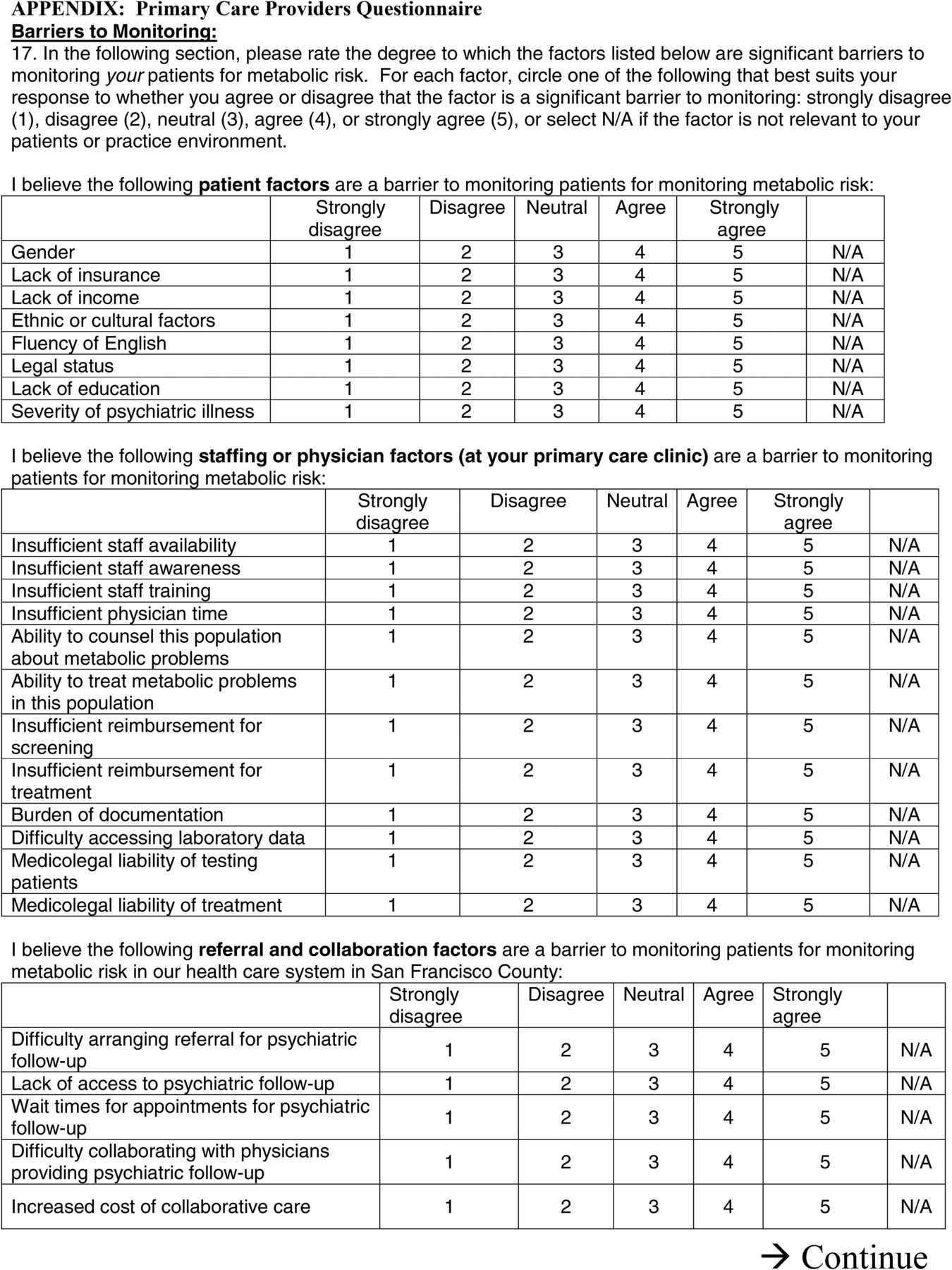
In addition to clinician demographic and practice questions,29,30 the survey included questions about perceived roles of providers in metabolic monitoring and/or treatment of metabolic abnormalities and barriers to metabolic monitoring of patients on antipsychotic medications. Questions were drawn from the literature and expert consultation as described previously.23,24,27⇓⇓–30
Attitudes about roles were rated on a 5-point Likert scale. Because responses were skewed, these were reduced to: (1) “Disagree” (including “strongly disagree,” “disagree,” and “neutral” responses), and (2) “Agree” (including “agree” and “strongly agree” responses).
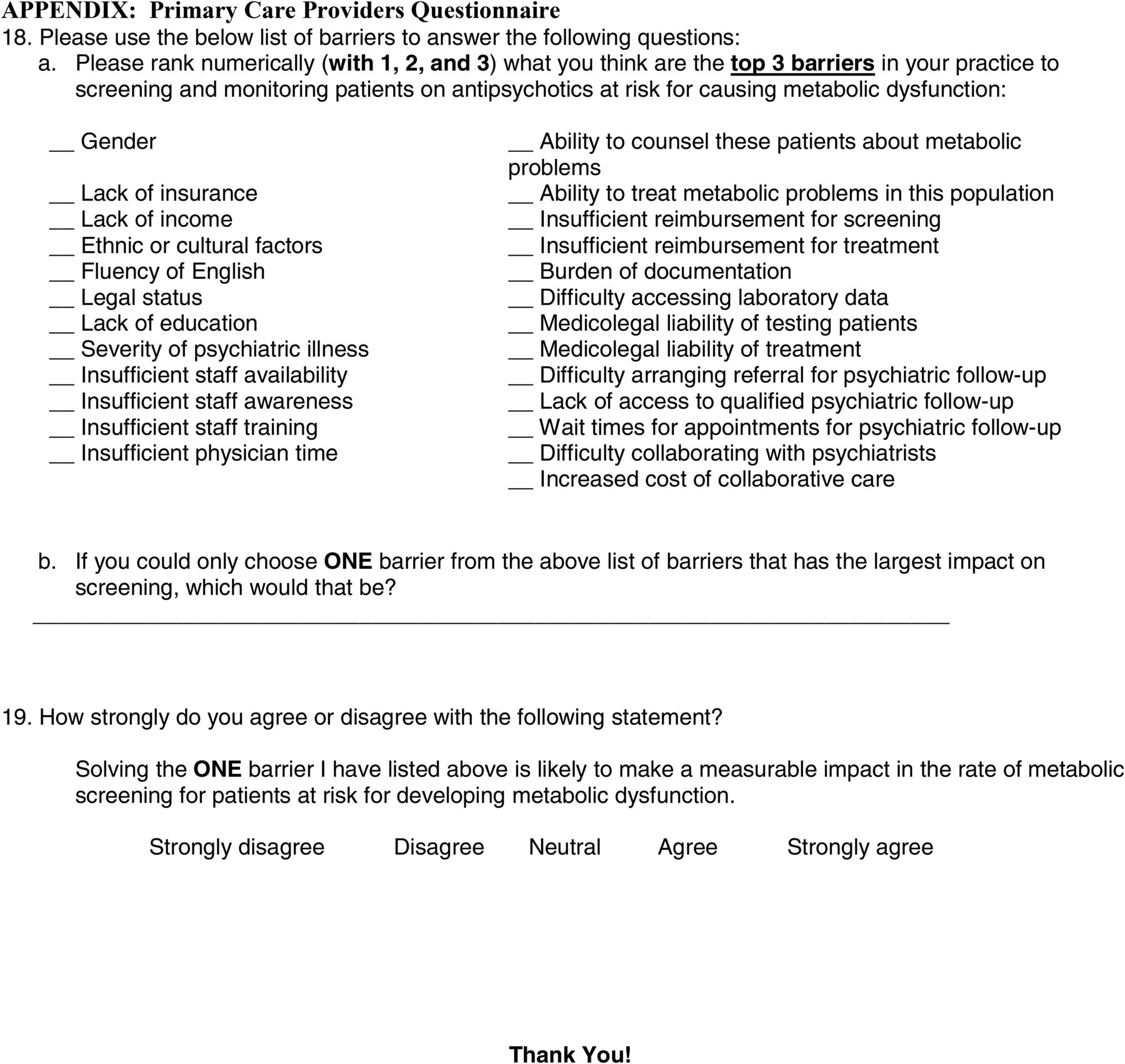
Respondents were asked to identify the 1 “top barrier” that had the largest impact on metabolic screening from 25 possibilities. Questions about care coordination were collapsed into 1 category (“Difficulty with care coordination”). The survey is publicly available online (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3780562/).
Data Analysis
The t tests and χ2 tests were used to determine if any clinician demographic characteristics were related to attitudes toward metabolic monitoring or treatment. Multivariate logistic regression analysis was used to examine if clinician characteristics might be associated with attitudes toward metabolic monitoring and treatment. Logistic regressions were used to determine whether clinician characteristics were associated with perceived barriers to metabolic monitoring.
Results
All 81 psychiatrists in this urban safety-net public health system were approached to participate; 69% (56/81) responded and 86% (49/56) of these met inclusion criteria. All 214 primary care clinicians in this urban safety-net public health system were approached to participate; 77% (164/214) of primary care clinicians responded and 98% (160/164) of these met inclusion criteria. Most primary care clinicians were physicians (62%, 99/160), whereas 36% (57/160) were nurse practitioners and 2% (4/160) were physician's assistants.
In terms of demographic information, the primary care clinicians were more likely than psychiatrists to be women (69% vs 39%, P < .001), but otherwise there were no significant differences between providers in age or race/ethnicity. In addition, there were no significant differences in opinions between medical doctor primary care clinicians and non-medical doctor clinicians for the questions highlighted below.
When asked about monitoring metabolic risk factors, clinicians were asked about specific circumstances. For example, most primary care providers (66%, 102/154) believed that “primary care providers, not psychiatrists,” should monitor metabolic risk in contrast to only 30% (14/47) of psychiatrists (P < .001, t = 4.637, df = 199) (Table 1).
Preferences for Type of Clinician Who Should Be Conducting Metabolic Monitoring of People with Severe Mental Illness
A significant proportion of both primary care clinicians (60%, 93/156) and psychiatrists (80%, 39/49) agreed that the “psychiatrist or mental health clinic, even if patients have established primary care” should monitor for metabolic risk factors, with psychiatrists believing this even more strongly (P = .011, t = −2.576 df = 203) (Table 1). In contrast, less than half of primary care providers (42%, 66/158) and fewer psychiatrists (15%, 7/48) believed that the psychiatrists' role is to “prescribe oral medications to treat elements of metabolic dysfunction (eg, statins…),” with a significantly lower proportion of psychiatrists believing that they should play this role (P < .001, t = 3.536, df = 204).
Sixty percent (114/191) of both clinician groups reported either severity of mental illness or difficulty with care coordination as 2 barriers. There were no significant differences in reported “top barriers” between the psychiatrists and primary care clinicians. Insufficient provider time, insufficient staff availability, and difficulty accessing laboratory data were reported by close to 20% of providers overall as key barriers.
Discussion
To our knowledge, this is the first study to compare psychiatrists' and primary care clinicians' opinions on provider and system-level factors that affect monitoring and treatment of metabolic abnormalities among people with SMI. Understanding clinicians' anticipated role in screening for these risk factors is a key component to increasing the rate at which patients with SMI receive medical treatment for these symptoms.
Our findings suggest a sizable disconnect between where (and by whom) clinicians believe metabolic monitoring should be done and where (and by whom) treatment should be initiated. Despite endorsing the practicality of psychiatrists monitoring metabolic abnormalities, a majority of clinicians in both groups believed that the treatment of metabolic dysfunctions is the role of the primary care clinician exclusively. This disconnect between where monitoring and treatment should occur undoubtedly contributes to the poor rates of treatment for metabolic abnormalities among this vulnerable population.
Despite initiatives to improve cardiometabolic screening and treatment among people with SMI,19⇓⇓–22 they are still woefully underscreened26 while being at greater risk for early mortality compared with the general population. Part of this problem—as highlighted in this study—is lack of ownership over who should be doing the screening. One solution to this potential lack of coordinated care among providers could involve colocating primary care clinicians in community mental health care settings. A study by McGinty et al (2015) indicates veterans with SMI tend to receive better comprehensive medical care in the Veterans Health Administration, which offers multiple providers at 1 location and includes a nationwide network of electronic medical records that assist with patient care. They found that compared with Veterans Health Administration patients, Medicaid patients had the lowest adherence to national guidelines on medical care and screening over time.31 Integrated health care systems provide the greatest ability to coordinate patient care but are costly and difficult to implement nation-wide.32 Therefore, it may be worth considering having on-site physicians at community mental health clinics (the psychiatrists) perform metabolic monitoring and initiating first-line treatment for relatively easy to treat metabolic abnormalities (eg, dyslipidemia). This could be facilitated through a standardized consultation with a designated primary care physician.
This study's primary limitation is that it relies on a single urban community safety-net health system. In addition, the clinicians were not asked to choose between specific clinician groups in questions regarding monitoring or treatment, making findings of role preferences less than definitive. Although these aspects are beyond the scope of this article, we believe this study is an important first step in qualifying the role psychiatrists and primary care physicians play in the identification and treatment of metabolic and cardiovascular risk factors in patients with SMI.
Acknowledgments
The authors thank Nicholas S. Riano, MAS, for his assistance in the preparation and submission of this manuscript.
Appendix




Notes
This article was externally peer reviewed.
Funding: This study was funded by a pilot grant from the Center for Aging in Diverse Communities funded by grant P30-AG15272 under the Resource Centers for Minority Aging Research program by the National Institute on Aging, National Institutes of Health (Dr. Mangurian, pilot PI; Dr. Perez-Stable, PI). In addition, Dr. Mangurian was supported by the National Center for Research Resources, the National Center for Advancing Translational Sciences, and the Office of the Director, National Institutes of Health (NIH), through UCSF-CTSI grant KL2 RR024130 and a NIH/National Institute of Mental Health Career Development Award (K23MH093689). Drs. Schillinger and Fuentes-Afflick were supported by the Clinical Research Network funded through NIH/NCCR UCSF-CTSI grant UL 1 RR024131. Dr. Dean Schillinger was also supported by the National Institute of Diabetes and Digestive and Kidney Diseases for The Health Delivery Systems-Center for Diabetes Translational Research (P30DK092924). Dr. Dilley was supported by a Substance Abuse and Mental Health Services Administration grant (1H79TI024339).
Conflict of interest: Ms. Giwa is currently working as an advisory consultant at PricewaterhouseCoopers. Ms. Brosey is currently working as a Clinical Trial Associate at Aerotek, Inc. The remaining authors have no conflicting or competing interests to report. The contents and views in this manuscript are those of the authors and should not be construed to represent the views of the National Institutes of Health or any of the sponsoring organizations and agencies of the US government.
To see this article online, please go to: http://jabfm.org/content/32/3/418.full.
- Received for publication June 19, 2018.
- Revision received January 4, 2019.
- Accepted for publication January 5, 2019.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}