
Abstract
Objective: The objective of this study was to determine what proportion of veterans previously screened for colorectal cancer (CRC) using fecal immunochemical testing (FIT) would be willing to undergo a second round of FIT screening.
Methods: Patients in the Iowa City Veterans Affairs Health Care System (<65 years old, asymptomatic, average risk, overdue for CRC screening) who completed a mailed FIT (April 2011 to May 2012) were contacted 1 year later by telephone to collect demographic and recent CRC screening information, and were offered a second mailed FIT if eligible.
Results: Of 204 veterans who completed initial FIT testing, 159 were eligible to participate in a second round of FIT screening; 132 (83%) participated in the telephone survey, and 126 (79%) completed a second annual FIT, with 10 (8%) individuals testing positive. The majority of participants (67%) reported being more likely to take a yearly FIT than a colonoscopy every 10 years. Participants overwhelmingly reported that the FIT was easy to use and convenient (89%), and they were likely to complete a mailed FIT each year (97%).
Conclusions: Those willing to take a mailed FIT seem satisfied with this method and willing to do it annually. Population-based or provider-based FIT mailing programs have the potential to increase CRC screening in overdue populations.
The most recent US Preventive Services Task Force colorectal cancer (CRC) screening guidelines recommend average-risk adults aged 50 to 75 years receive colonoscopy every 10 years; sigmoidoscopy every 5 years, with a midinterval high-sensitivity fecal occult blood test (FOBT) every 3 years; or annual high-sensitivity FOBT or fecal immunochemical testing (FIT).1 Several barriers to colonoscopy, such as distance from health care facilities and transportation to and from the facility, have been reported.2,3 These issues are particularly relevant to the US Department of Veterans Affairs Health Administration (VHA) because over 3 million (36%) of enrolled veterans reside in rural areas.4
The VHA recently approved the use of FIT, a high-sensitivity FOBT that can be administered at home. Advantages of FIT over guaiac FOBT include higher sensitivity for detection of significant adenomas and CRC, lack of diet or medication restrictions, and the need for only 1 sample.2,3
We previously demonstrated the effectiveness of an initial mailing of a FIT to eligible patients overdue for CRC screening.2,3 Although annual FIT screening is recommended, little is known regarding patients' willingness to participate in repeated annual FIT screenings. Therefore, the objective of this study was to determine what proportion of patients who previously screened negative with FIT would be willing to complete a second round of annual FIT screening, and what proportion would screen positive.
The 2 mailed FIT interventions have been described previously.2,3 In the initial 2 interventions, 232 participants completed a FIT. Of these participants, 28 (12%) had positive FITs and were referred for follow-up care, whereas those who tested negative (n = 204) were included in this prospective follow-up study to determine their willingness to complete a second annual FIT.
Approximately 1 year after completing their initial FIT, potentially eligible patients received a recruitment letter explaining the study, followed by a telephone call to assess eligibility and willingness to take a brief survey. Immediately following the survey, participants were asked to take a second annual FIT. Those who agreed were mailed an OC FIT-CHEK kit (Polymedco, Cortlandt Manor, NY) with instructions and a preaddressed, postage-paid envelope to return the FIT.
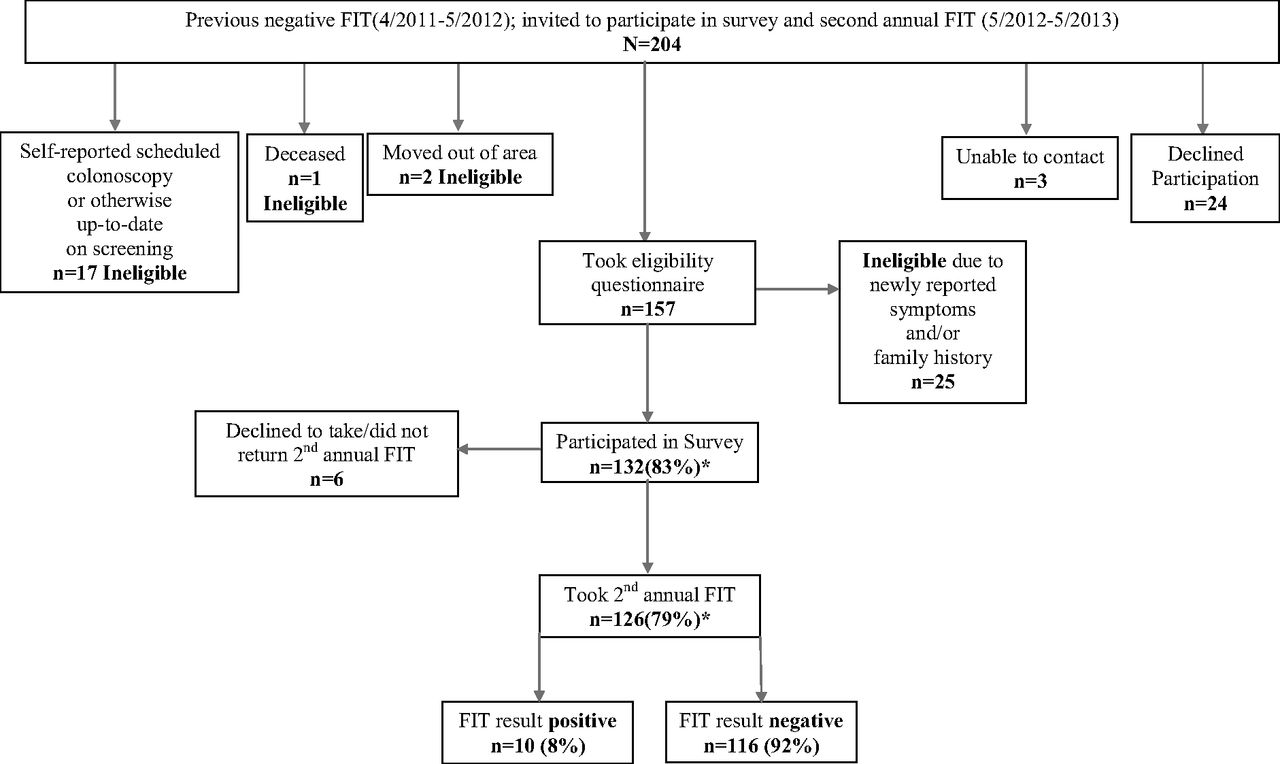
Of those eligible (n = 159), 132 (83%) participated in the survey and 126 (79%) returned a second annual FIT. There were 10 positive FITs (8%), and these patients were referred for follow-up care (Figure 1). Participants overwhelmingly reported the FIT was easy to use and convenient (89%), and they would be likely to complete a mailed FIT each year (97%) (Table 1). There were no significant differences between FIT participants versus nonparticipants by age, sex, or rurality (data not shown).

Study population, Iowa City VA Health Care System. *Percentage calculated from the total eligible to participate. Of 204 invited to participate, 45 were ineligible (2 moved out of the area, 1 was deceased, 17 self-reported scheduled colonoscopy or otherwise being up to date on screening, and 25 reported new symptoms and/or family history on the eligibility questionnaire given before the survey). This left 159 potentially eligible to participate. Three were unable to be contacted and 24 declined participation, but were included in these 159 potentially eligible patients. FIT, fecal immunochemical testing.
Few studies have examined patients' willingness to participate in follow-up FIT after their initial screening. In this group of largely rural veterans initially overdue for CRC screening, 79% participated in a second annual mailed FIT. Similarly, a population-based FIT screening program in Amsterdam demonstrated that 85% of participants completed a second biennial mailed FIT.5
Several limitations should be considered when interpreting the study results. Because of the limited sample size, we were unable to conduct subgroup analyses. Although the original cohort was identified based on regular VHA use, 17 participants reported scheduled or up-to-date CRC screens from outside the VHA, which we were unable to verify. Furthermore, this sample of veterans who previously participated in a FIT intervention may not be generalizable to other clinic populations. This is, however, one of the few studies to present data on repeated FIT testing in the United States.
Conclusion
FIT mailing programs seem to be an effective method to provide CRC screening for overdue patients, especially those who face barriers to colonoscopy. Providers should consider offering FIT as an option along with other evidence-based methods.
Acknowledgments
The authors thank Stacy Wittrock and Ashley Cozad for their efforts in coordinating this study. The authors also acknowledge Lindsey Davenport-Landry in the Iowa City Veterans Affairs laboratory for her work managing all the laboratory aspects of this project.
Notes
This article was externally peer reviewed.
Funding: This research was supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, Veterans Rural Health Resource Center-Central Region (VRHRC-CR), and the Veterans Affairs Health Services Research and Development (HSR&D) Service, Center for Comprehensive Access and Delivery Research and Evaluation (CADRE) (CIN 13-412). This work was also supported by the University of Iowa Holden Comprehensive Cancer Center, which is funded in part by NIH/NCI P30 CA086862.
Conflict of interest: none declared.
Disclaimer: The views expressed in this article are those of the authors and do not necessarily represent the views or policy of the Department of Veterans Affairs or the United States Government.
- Received for publication August 25, 2014.
- Revision received December 29, 2014.
- Accepted for publication January 9, 2015.




{kind=link}