
Abstract
In the past decade the advent of target therapy has led to a silent revolution in the treatment of lung cancer. Thanks to the specificity of their target, new tailored drugs are able to achieve a larger benefit and lower toxicity and provide better quality of life than cytotoxic drugs in a limited number of patients, selected by molecular profile. Nowadays, the epidermal growth factor receptor tyrosine kinase inhibitors erlotinib and gefitinib, and the anaplastic lymphoma kinase inhibitor crizotinib, are targeted agents approved for treatment of non-small-cell lung cancer. Family physicians play an important role in the treatment, detection, and management of common toxicities and in providing emotional support. Therefore this review integrates molecular profile assessment with evidence of the efficacy and toxicity of tyrosine kinase inhibitors to provide an updated overview of the treatment of non-small-cell lung cancer, which radically changed after the advent of targeted therapies. It also aims to promote a more intensive and interactive collaboration between specialists and family physicians in the management of all phases of cancer care.
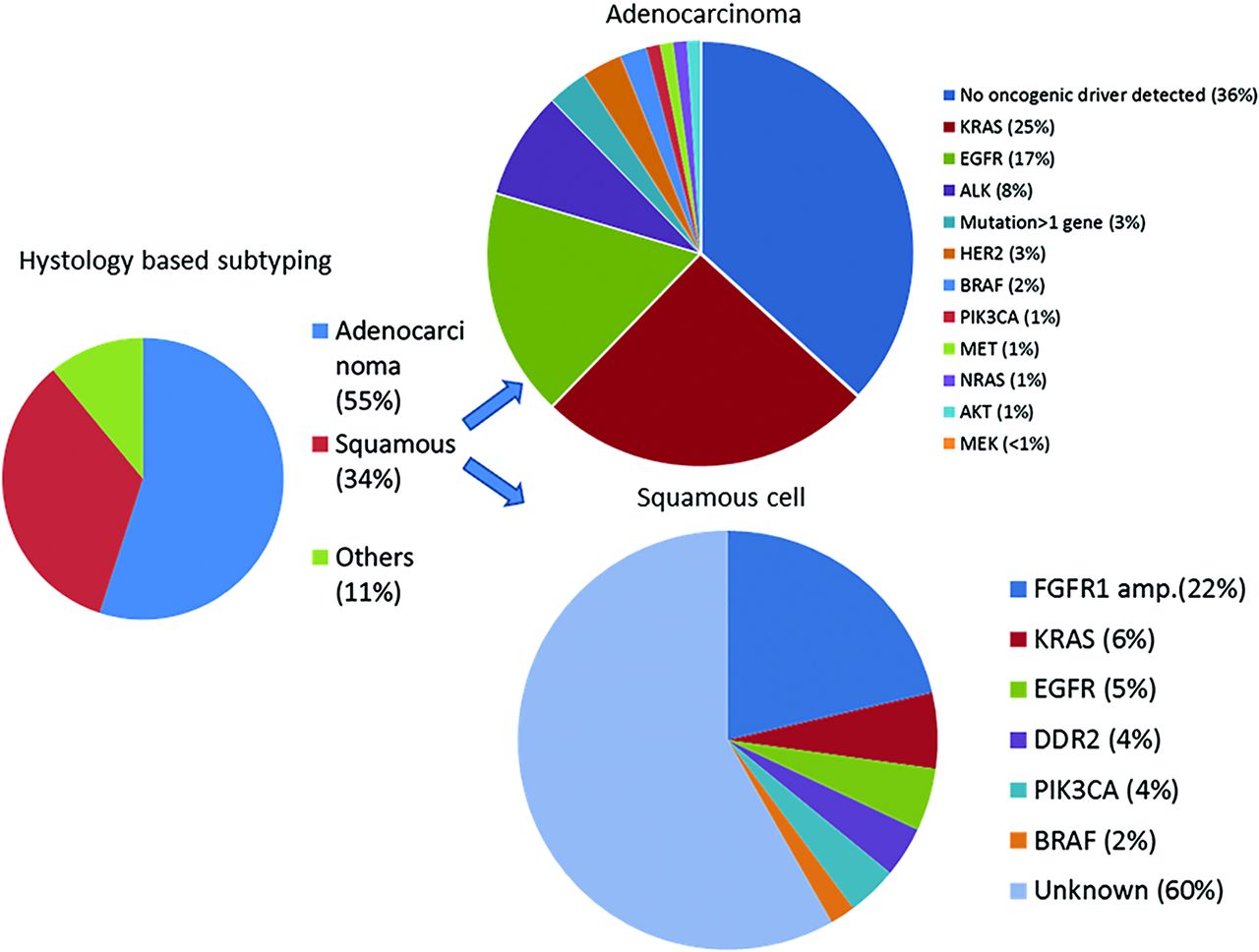
The past decade has witnessed a silent revolution in the war against cancer, thanks to the advent of new therapies, which target specific mutations related to cancer cell proliferation and survival in different types of tumors. Among all cancers, lung cancer remains the leading cause of cancer-related death in most countries, with 159,260 expected deaths in the United States in 2014. Lung cancer occurs predominately in people between 50 and 70 years old, but the risk of developing this cancer reaches a peak in people older than 70 years. Lung cancer incidence decreased in the past two decades in several countries, including the United States, following a decreased rate of smoking. At the same time, the incidence among women, including former or never smokers, is rapidly increasing.1 The discovery of “oncogenic driver mutations” and the subsequent development of tailored agents has radically changed the treatment of lung cancer in ten years, leading to the development of personalized strategies.2,3 Non-small-cell lung cancer (NSCLC) was traditionally classified, based on histologic features, as adenocarcinoma, squamous cell carcinoma, and other nonspecified subtypes, which represent about 55%, 35%, and 10% of all NSCLC cases, respectively. In the early 1990s treatment approaches available for patients with lung cancer were poor, with a median survival of 2 to 4 months.4 The introduction of platinum-based combinations with third-generation agents such as gemcitabine, vinorelbine, and docetaxel significantly improved survival outcomes, which led to a “plateau” of about 10 to 11 months' median survival; nowadays these combinations are still considered the standard of care for the majority of patients with NSCLC.5 Subsequently, significant advances have been made with the introduction of new, more specific cytotoxic drugs, such as pemetrexed, with improved efficacy, especially against the non–squamous cell carcinoma subtype. The addition of this agent led to a further improvement in survival to 12 to 13 months6 and up to14 months with the introduction of maintenance treatment.7 Furthermore, the discovery of key oncogene alterations contributed to the gradual shift of NSCLC classification from a histologic- to molecular-based profile. In fact, even when the histologic subtype is a factor when selecting among different chemotherapies, the tumor molecular features are now crucial for the selection of patients to receive new tailored agents. The first example is the discovery of specific epidermal growth factor receptor (EGFR) mutations and ALK gene rearrangements in a subset of patients with NSCLC, leading to the development of the EGFR tyrosine kinase inhibitors (TKIs) erlotinib, gefitinib, and afatinib and the ALK inhibitors crizotinib and ceritinib, which currently are the only targeted drugs approved for the treatment of NSCLC.8 New driver mutations were recently identified in both adenocarcinoma and squamous cell carcinoma, and several ongoing trials are investigating the activity of new potential target agents. The introduction of new tailored approaches in clinical practice changed the lung cancer treatment strategy; new emerging toxicities require active involvement and collaboration of family physicians in all phases of care. Family physicians, with their ongoing relationships with patients and the patient's family and caregivers, has an important role in the treatment, detection, and management of common toxicities and in providing emotional support. Family physicians are also well positioned to identify and address unmet nonmedical and medical needs that have such a crucial influence on quality of life, playing a key role in mediating the relationship between the medical oncologist and the patient. Therefore we believe that family physicians should be up to date with these radical changes in clinical oncology, especially with regard to the treatment of common malignancies such as NSCLC (Figures 1 and 2).

Molecular subsets of lung cancer.
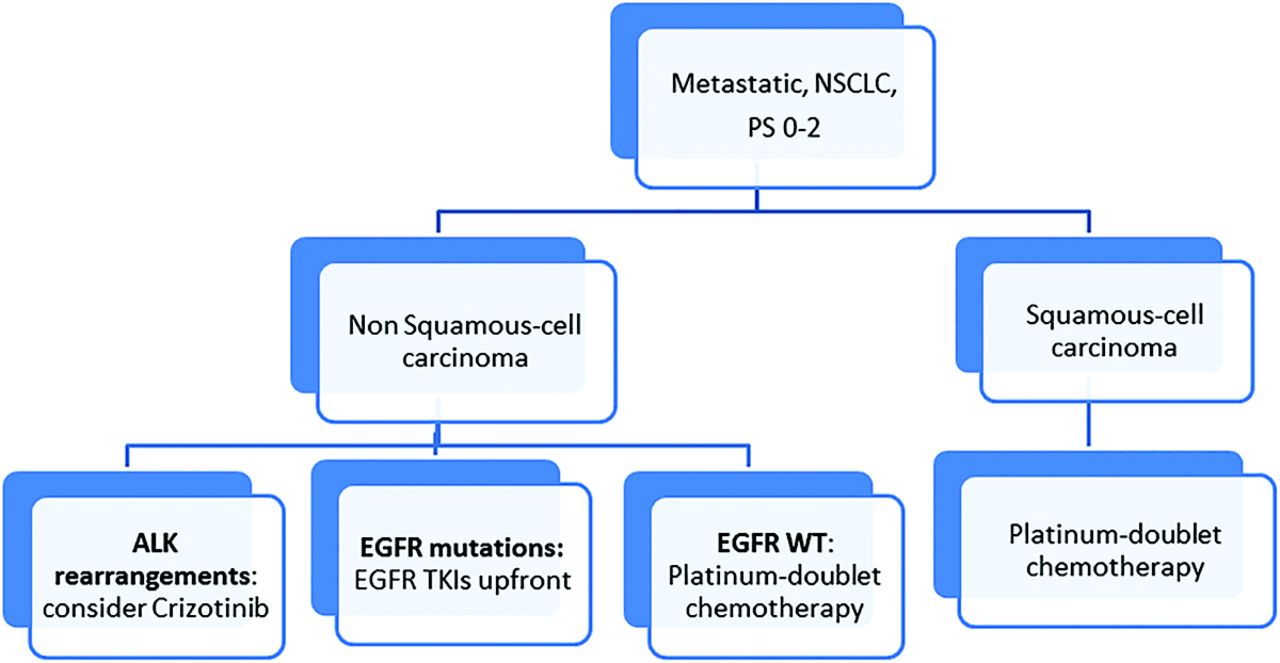
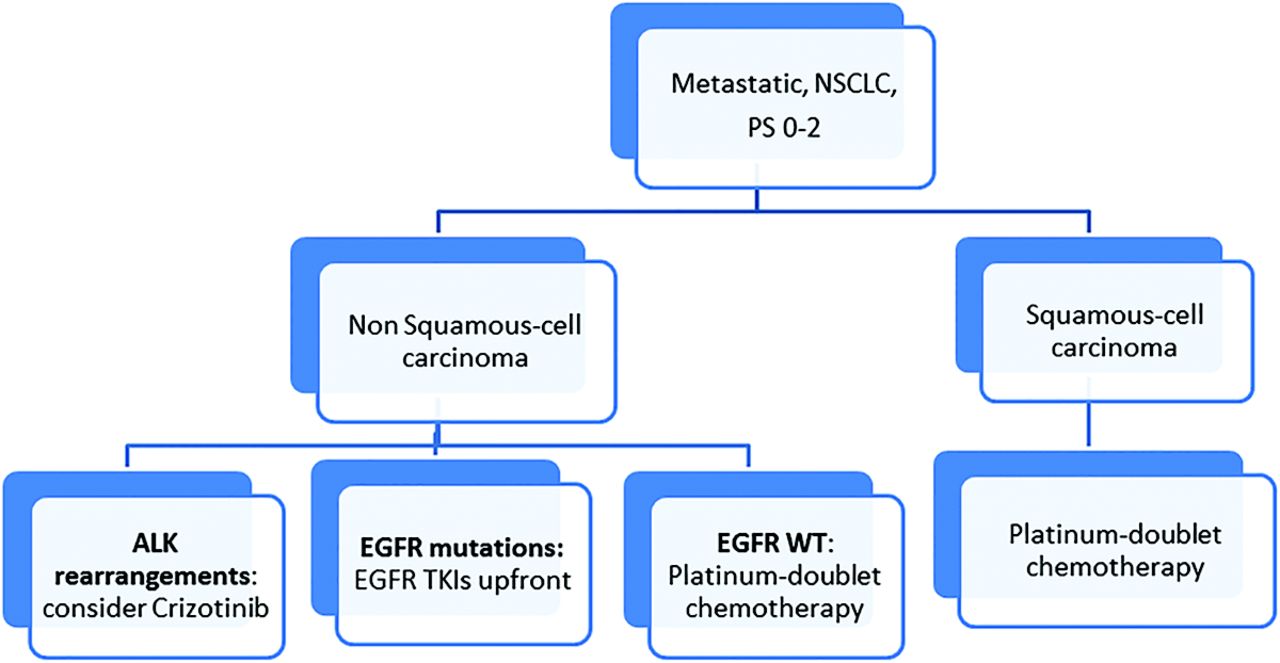
Treatment algorithm in first-line metastatic non-small-cell lung cancer (NSCLC). EGFR, epidermal growth factor receptor; PS, performance status; TKI, tyrosine kinase inhibitor; WT, wild-type.
EGFR Pathway and EGFR Inhibitors
EGFR Mutations
EGFR-activating mutations are the most frequent driver mutations in NSCLC, reported in about 40% to 60% of Asian,9⇓–11 15% to 20% of white,12,13 and about 30% of Latin-American14 patients with NSCLC; they are very important as clinical predictors of EGFR TKI sensitivity and efficacy.15 The most frequent mutations are exon19 deletions (>20 variant types) and a mutation at codon 858 in exon21 (L858R), accounting for 90% of overall EGFR mutations.16 Several in vitro studies demonstrated that these mutations increased EGFR activity and were responsible for cancer cell proliferation and survival, also leading to angiogenesis, tumor invasion, and metastatic potential. Following molecular interaction with the receptor, small-molecule TKIs specifically inhibit EGFR and are capable of inactivating the downstream aberrant signaling pathways.
EGFR TKIs
EGFR TKIs represent the mainstream in targeted therapy in NSCLC, leading to improvements in the median survival rates and quality of life for patients with tumors harboring EGFR-activating mutations. Gefitinib is available as film-coated tablets that contain 250 mg of the active compound, taken once a day. Erlotinib is available in 3 dose-strength tablets: 25, 100, and 150 mg; the recommended dose is 150 mg once a day. Both of these drugs are recommended as first-line treatment for patients whose tumors harbor EGFR-activating mutations, but erlotinib was also approved as a second-/third-line treatment for patients with unknown EGFR mutational status.17 Several randomized studies included in a recent meta-analysis, however, showed that erlotinib and gefitinib have lower efficacy than standard chemotherapy in pretreated patients with EGFR wild-type tumors18, suggesting that the EGFR mutation is a predictive biomarker for EGFR TKI efficacy in a second-line setting. Both drugs should be taken 1 hour before or 2 hours after lunch, whereas only erlotinib-treated patients should avoid drinking grapefruit juice, reduce or stop smoking, and avoid taking proton pomp inhibitors 4 hours before or 2 hours after the TKI's uptake to avoid drug's interactions. Afatinib, another TKI, has been recently approved by the US Food and Drug Administration (FDA) and European Medical Agency as a first-line treatment of NSCLC in patients whose tumors harbor EGFR-activating mutations, at a dose of 40 mg once daily.
At least 8 different clinical trials comparing front-line EGFR TKI treatment with standard platinum chemotherapy in patients with EGFR-mutated NSCLC have shown that targeted treatment is better than standard chemotherapy in this selected patient population, leading to a significant improvement in survival, which reached a plateau of 24 to 30 months11,15,19⇓⇓⇓⇓–24 (Table 1). Such findings suggest that testing tumors for specific activating mutations, and tailoring the therapeutic approach, may optimize patients' survival outcomes. Several studies showed a higher occurrence of EGFR-activating mutations in a subgroup of patients with NSCLC reporting some clinical features, such as “women, nonsmokers, Asian race and especially adenocarcinoma subtype,” which could be considered as clinical predictive factors for TKI sensitivity. Otherwise, a significant percentage of patients without the aforementioned clinical features also was positive for EGFR-activating mutations.25 Based on these findings, the American Society of Clinical Oncology recommends EGFR mutation testing before treatment with EGFR TKIs in the management of all patients with advanced lung cancer.26 While most patients with EGFR-mutated NSCLC present good initial responses to treatment with gefinitib or erlotinib, they invariably develop resistance to EGFR TKIs,25 translating into clinical disease progression usually after 10 to 12 months of treatment. In clinical practice this often interrupts the current targeted treatment and requires a switch to a standard platinum-doublet chemotherapy. In the past year, however, an improved understanding of the mechanisms of underlying resistance to EGFR TKIs emphasizes the importance of a genotype-guided approach to therapy. Several cell-based studies identified a second EGFR gene mutation, T790M, as the leading cause of acquired resistance to first-generation EGFR TKIs in about 50% of patients.27 This observation guided the development of a new generation of irreversible EGFR inhibitors, including CO1686 and AZD9291, capable of specifically targeting and inactivating the T790M mutation.28,29 Another significant group of cancers (approximately 20%) acquire resistance to EGFR TKIs following the amplification of the mesenchymal–epithelial transition (MET) factor receptor tyrosine kinase, which activates different EGFR signaling pathways.30 Other resistance-related processes include Her-2 amplification (12%), phenotypic change from NSCLC to small-cell lung carcinoma (4%), and modifications in other parallel signaling pathways.31 Several ongoing studies will contribute to an improved understanding of the molecular basis of acquired resistance, and new therapeutic approaches will improve the efficacy of anticancer regimens in NSCLC.
ALK Translocation and ALK Inhibitors
EML-ALK Chromosome Rearrangement
In 2007 Soda and colleagues32 discovered another driver mutation in NSCLC: the EML4-ALK fusion gene, which is the consequence of a chromosomal rearrangement, resulting in a fusion between the N-terminal portion of the EML4 protein and the intracellular region of the receptor ALK. EML4–ALK fusion leads to a ligand-independent, constitutive activation of the rearranged ALK receptor, which is responsible for both tumor cell proliferation and survival. ALK translocation occurs in about 3% to 7% of patients with NSCLC33 and is not mutually exclusive with EGFR and KRAS gene mutations. Data obtained from different studies show that it is more frequent in Eastern Asian patients, those with adenocarcinomas histotypes, light or never smokers, women, and younger patients. However, it was also reported in patients with squamous or adenosquamous carcinomas and in smokers, albeit at a much lower rate.33,34 Furthermore, the ALK-positive tumor phenotype seems to be associated with worse survival and an increased risk of brain and liver metastases,35 whereas it is resistant EGFR TKI therapy33,34 and has higher sensitivity to the cytotoxic agent pemetrexed.36 Immune fluorescence in situ hybridization is currently considered the standard test, approved for the detection of ALK -rearrangements in tumor samples (Figure 3).

ALK-positive fluorescence in situ hybridization image of a patient with non-small-cell lung cancer.
EML-ALK Inhibitors
Crizotinib is the first and actually the only available ALK inhibitor approved for treatment of ALK-positive patients with NSCLC, at doses of 250 mg twice daily (500 mg/day). It is a potent oral ATP competitor at the ATP-binding pocket of the ALK receptor, with additional anti-MET and anti-ROS1 activity. The approval and subsequent introduction of crizotinib in clinical practice was based on the results of phase I and II trials which showed a surprising response rate as well as a progression-free survival rate in ALK-positive pretreated patients,37⇓–39 leading to an acceleration of the drug registration procedures, definitively approved by the FDA in October 2011. This is the first report in the history of oncology that a drug is approved based only on the phase I and II data. These results were subsequently confirmed by a phase III trial (PROFILE 1007), which showed a significant improvement of response and survival rates and also in terms of quality of life for pretreated patients with NSCLC.40 Today, the drug is still recommended for the treatment of ALK-positive patients with NSCLC only when progressing after first-line chemotherapy,8 but another randomized phase III trial, PROFILE 1014, investigated the efficacy of crizotinib in a first-line setting, showing a significant survival benefit in this selected subgroup of patients.41 Unfortunately, because of the development of resistance, ALK-positive patients treated with crizotinib also relapse after a variable period of sensitivity; this may be related to a second mutation either in the ATP-binding pocket or the amplification of the ALK fusion gene. Other less frequent alterations include increased EGFR phosphorylation and mutation, Kit amplification and mutation, and KRAS mutation. Next-generation ALK inhibitors, developed to overcome crizotinib resistance, are under investigation in several early phase studies. One of these compounds, ceritinib, has shown great activity in a recent phase I study by Shaw et al,42 receiving approval by the FDA for the treatment of ALK-rearranged patients with NSCLC who had progressed or were intolerant to crizotinib. Since these second-generation target drugs have variable efficacy against some specific mutations, molecular testing after progression is required to ensure the best tailored approach43 (Table 2).
Emerging Toxicities and Management
EGFR Inhibitors' Toxicity
TKIs present a good tolerability profile, with a significantly lower incidence of side effects, such as myelosuppression, nausea, vomiting, fatigue, and neurotoxicity, when compared with chemotherapy. On the other hand, new adverse events, such as skin rash, diarrhea, and asymptomatic hypertransaminasemia, emerged as a specific result of silencing the EGFR pathway in healthy cells, whereas severe toxicities were less frequently reported.15,22,23 Skin toxicity is the most common adverse effect associated with TKIs, reported in >80% of patients treated with these drugs. Although <20% of patients have severe symptoms,44 skin toxicity is visible and often causes physical and emotional discomfort, resulting in a significant impact on quality of life.45 Such toxicity is related to dose reductions in 60% of patients or discontinuation of treatment in 32%,46 with subsequent poor clinical outcomes and an increase in management costs. Thus it is essential for family physicians to be aware of these dermatologic side effects to ensure appropriate and early management. Skin rash is characterized by a monomorphic papulopustular eruption, often confined to seborrheic areas (midfacial region and the upper trunk), which consists of erythematous follicular papules that evolve into pustules and sometimes may become infected, usually with Staphylococcus aureus, forming yellow crusts.47 The reactive treatment of skin rash depends on its severity. Differentiating low-grade toxicity (grade 2), characterized by eruption with papules or pustules covering <30% of the body surface without symptoms interfering with daily activities, from moderate to high-grade toxicity (grade 3), characterized by eruption with papules or pustules covering >30% of the body surface, with symptoms that interfere with daily activities, is important. In grade 2 toxicity, local treatment with an antibiotic (clindamycin 1% gel, erythromycin 3% gel, or metronidazole 1% gel) is recommended. In grade 3, in addition to the local treatment, systemic treatment with oral tetracyclines for 4 weeks and oral corticosteroids for 10 days is recommended. If no improvement occurs, discontinuation or interruption of treatment may be indicated. For nonresponsive and grade 4 toxicity, which is characterized by generalized rash or severe symptoms, systemic treatment with intravenous corticosteroids, antibiotics, and hydration—or even hospitalization for emergency treatment—may be considered.48,49 Although the toxicity profile between different TKIs is comparable, it seems to be somewhat worse for afatinib than for erlotinib or gefitinib. Furthermore, data reported from several trials and a recent meta-analysis50 suggested that patients reporting skin rash had better survival than those without skin toxicity. Thus rash can be considered an independent, clinical, early predictor of TKI efficacy, and providing this information to patients could help them better tolerate toxicity-related physical and emotional discomfort (Figure 4 and Table 3).

Cutaneous toxicities, or “skin rash”, caused by tyrosine kinase inhibitors in patients with non-small-cell lung cancer.
ALK Inhibitor Toxicity
Patients treated with crizotinib reported fewer toxicities and improved results in lung cancer symptom control and in global quality of life when compared with patients treated with chemotherapy. The most frequent treatment-related adverse effects were visual disorders, such as visual impairment, photopsia, blurred vision, vitreous floaters, photophobia, and diplopia. Gastrointestinal events such as nausea, vomiting, diarrhea, and constipation are generally mild, can be managed with a supportive care, and tend to decrease in severity after the first few weeks of therapy. Because elevated liver enzymes are frequently observed (40% to 70%) with grade 3 in 7% to 15% of patients, monitoring them every 2 weeks of the crizotinib therapy's duration is strongly recommended. Peripheral edema, which is a common side effect, may be managed with standard medical intervention. Finally, about 69% of patients experienced at least 1 episode of sinus bradycardia (heart rate ≤60 bpm).40 With regard to ceritinib, the most grade 3 to 4 common terminology criteria for adverse events were diarrhea, fatigue, hyperglycemia, hypophosphatemia, increased transaminases and lipase concentrations, and anemia.42
Future Perspectives and Conclusions
The introduction of the EGFR TKIs gefitinib, erlotinib, and afatinib and the ALK inhibitors crizotinib and ceritinib represent the most important innovations in NSCLC treatment over the past ten years. By targeting the main pathways of NSCLC pathophysiology, these new drugs significantly improved survival rates and quality of life in a highly selected subgroup of patients, sparing them from toxic chemotherapy approaches; for the vast majority of patients, however, chemotherapy remains the only potential treatment. Although the target agents were approved only for EGFR and ALK gene alterations,8 the number of potential biomarkers is rapidly increasing. New driver mutations were identified in both adenocarcinoma, such as K-Ras, Her-2-neu, MET, N-Ras, BRAF, MAP-2-K, PIK3CA, AKT1, ROS, and RET mutations, and squamous cell carcinoma, such as FGFR-1 amplification, EGFR mutation and amplification, PIK3CA mutation and amplification, PTEN loss, and DDR2, but >50% of mutations remain unknown.51,52 Several ongoing trials are investigating the activity of new target agents in patients with these mutations (Table 4). The rapidly growing number of targeted treatment options will lead to new insight into personalized treatment in the near future. Nowadays, new techniques such as “next-generation-sequencing” make possible the creation of a molecular–genomic profile of every patient's tumor, based on the analysis of either a single tissue sample, circulating tumor cells, or circulating tumor DNA. Therefore the need for close collaboration between health professionals, including medical oncologists, molecular biologists, pathologists, and family physicians, will increase. The role of family physicians remains critical because of their unique and privileged position of seeing patients on a daily basis; thus they should be updated by other experts on scientific discoveries relevant to their everyday practice and more frequently involved in the global view of care in all the phases.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication February 26, 2014.
- Revision received September 7, 2014.
- Accepted for publication September 25, 2014.




{kind=link}
{kind=link}
{kind=link}
{kind=link}