
Abstract
Background: National guidelines for treatment of asthma include recommendations for providing written asthma action plans (AAPs) to improve outcomes through patient self-management. However, AAP completion rates remain limited in practice.
Methods: We developed a team-based approach for the delivery of care to asthma patients in a primary care setting that involved integration of an electronic clinical quality management system and provision of written AAPs by registered nurses.
Results: The percentage of patients with AAPs increased after implementation of clinical reminders and nurse-led provision of written AAPs.
Conclusion: Proper training, use of an electronic clinical reminder system, and enhanced engagement of registered nurses can improve AAP completion rates in a team-based primary care setting.
National guidelines for treatment of asthma include recommendations for providing written asthma action plans (AAPs) to support patient self-management.1 However, research indicates that AAP completion rates often remain low despite such recommendations.2–4 Proactive, clinic-based approaches to asthma management have shown promise in increasing the use and ownership of AAPs, but they involve extensive provider training and/or health care worker time commitments.1,5
During the period 2005 to 2006, our academic health center reported low AAP completion rates (7.5%; 884 of 11,785 patients) despite existing guidelines, AAP templates, and feedback from a quality improvement team. With no formal process in place for implementing clinic practice change, we piloted a team-based approach to increase the number of patients with written AAPs at 5 community-based family medicine clinics. The clinics handled 1300 to 2500 patient visits per month with staffing levels of 8 to 17 physicians and 2 to 4 registered nurses (RNs). A clinical quality management system (CQMS, Crimson Care Registry, Ann Arbor, MI) provided reminders to the physician at the time of the office visit. The system was capable of monitoring management for patients with chronic conditions, producing lists of patients with persistent asthma, delivering evidence-based reminders for asthma management, and tracking provider-generated responses.
Methods
Our team-based approach involved CQMS reminder use and nurse engagement in AAP development to increase the number of asthma patients with written AAPs. Because merely educating physicians to provide AAPs does not necessarily lead to changes in practice, we used RNs and the CQMS.5 A family medicine physician, an outpatient pulmonary care RN, and a family medicine outpatient RN (both RNs are certified as asthma educators) developed a 2-hour educational program for delivery to RNs, faculty, and residents. National guidelines for patient education shaped topic selection and AAP template design. Physicians received a 15-minute introduction to the new AAP prompts, RN referral process, AAP templates, and educational materials.4,5 Patients met with RNs for 1 hour or less after regularly-scheduled office visits as a follow-up to physician recommendations or in response to telephone invitations made by clinic staff using CQMS-generated patient lists.
After receiving an institutional review board nonregulated determination, we reviewed Blue Cross/Blue Shield's Physician Group Incentive Program (PGIP) and CQMS data to examine AAP response rates between June 2007 and December 2009. We analyzed data descriptively and by simple linear regression over time (PASW Statistics 18.0; SPSS/IBM, Chicago, IL).
Results
From 2006 to 2009, we educated 14 RNs, 30 residents, and 56 faculty. RNs wrote ∼98% of the AAPs based on physician and RN reports. Inclusion criteria for persistent asthmatics in the PGIP database somewhat differed over time because of changes in the reporting criteria of our internal health system, with a total of 10,071 to 11,686 recorded per year during the study period. Physician responses to the CQMS reminders remained high, ranging from 78% (993 of 1276) in 2007 to 90% (1481 of 1647) in 2009 (P = .121). Responses to AAP reminders included “completed today” (26%), “ordered for upcoming visit” (9%), “did not address due to more pressing health concern at visit” (13%), “discussed/deferred” (49%), and “refused” (3%).
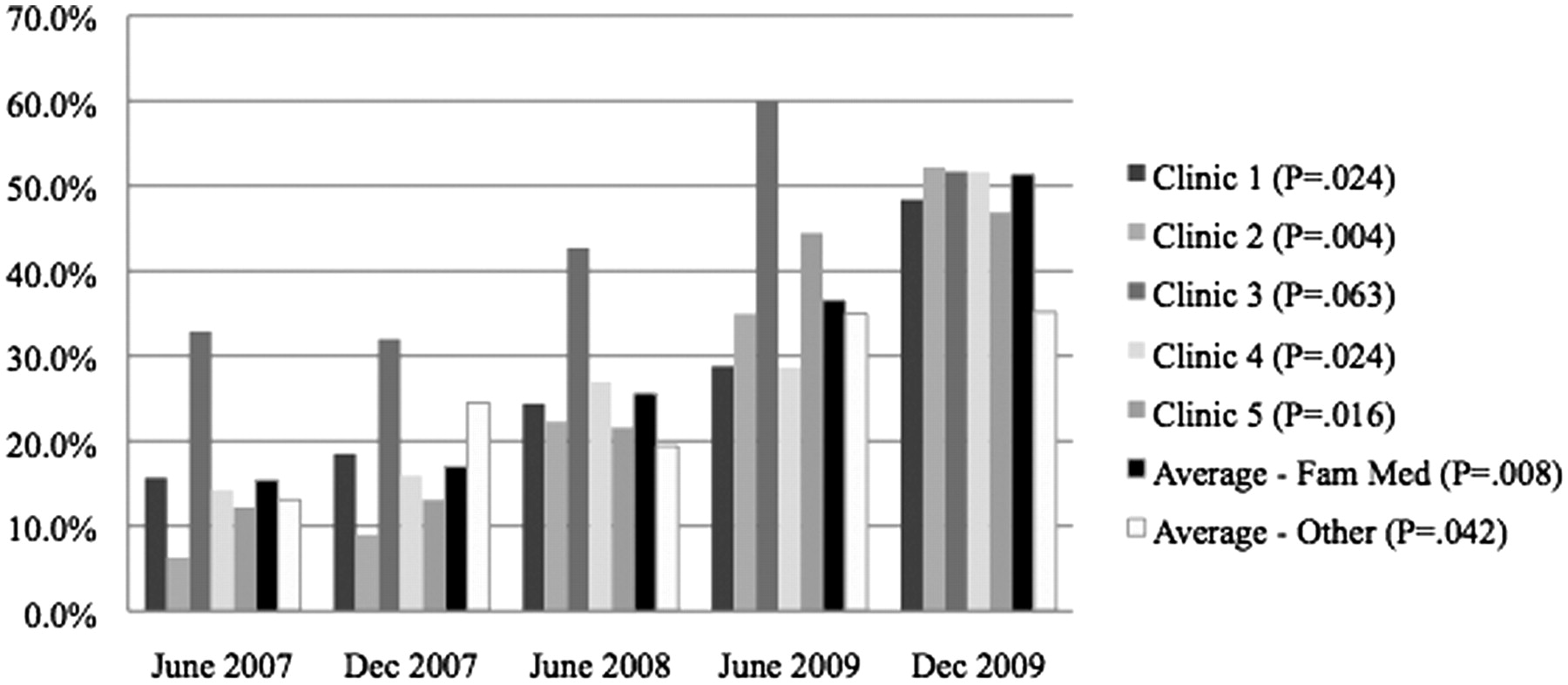
From June 2007 to December 2009, the total number of patients provided with written AAPs increased significantly over time at most family medicine clinics, and at a level that exceeded other primary care clinics within the health system (Figure 1). Clinic 3 served as the pilot site, and AAP rates remained highest there for the majority of the study period, only showing a slight decline in late 2009 after reaching saturation.
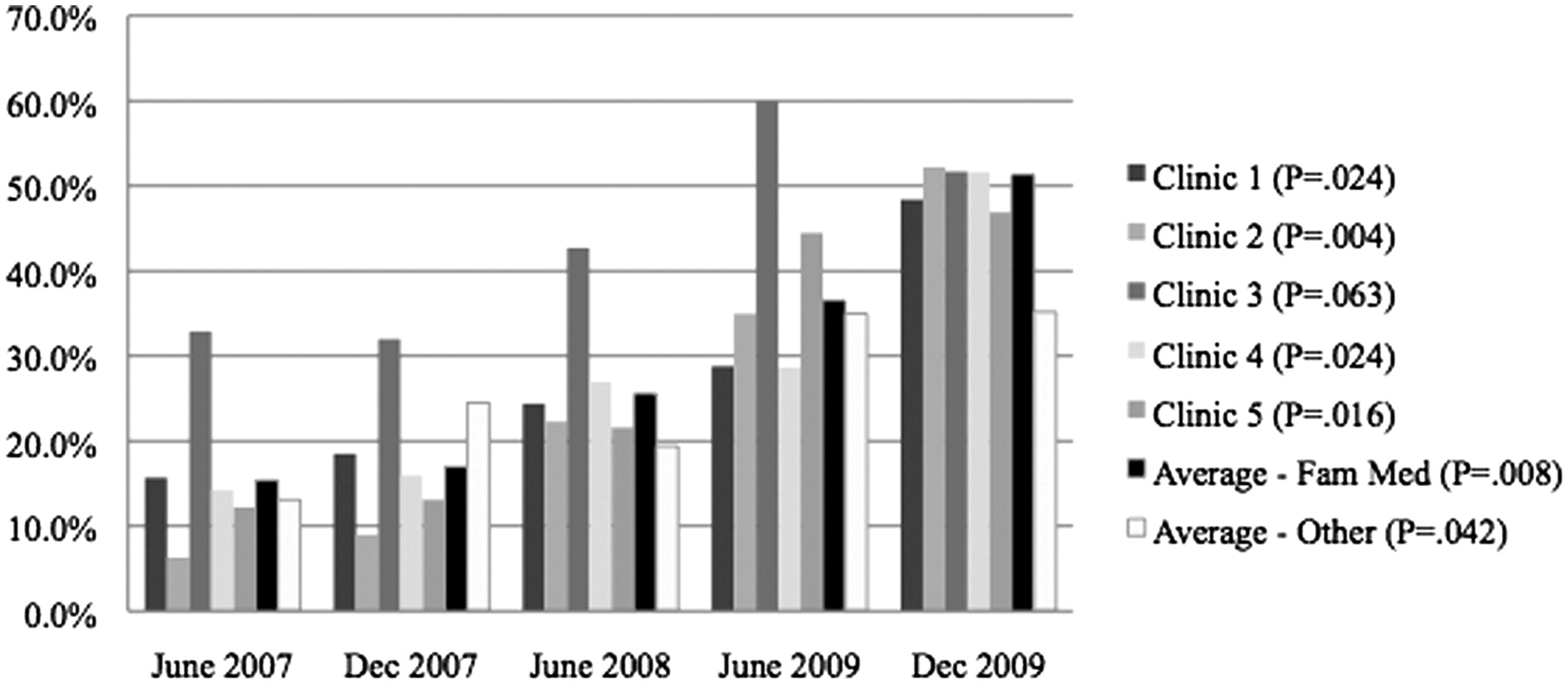
Asthma action plan rates (cumulative %) for patients with persistent asthma. Results are based on the Physician Group Incentive Program chart review. Physician Group Incentive Program data from December 2008 was not available. Average-Other represents cumulative asthma action plan completion rates for the departments of internal medicine and pediatrics.
Discussion
In this study, AAP completion rates increased over time, with the largest and most rapid increases attributed to easily adopted clinical processes, as recommended by Ring et al5 following a systematic review of research about promoting AAP use. PGIP funding during this time was only used for development of the database and was not used for other asthma care improvement activities.
AAP completion rates rose throughout the institution, but the greatest improvements were shown in family medicine clinics that systematically implemented asthma training programs, use of clinical reminders, and enhanced RN engagement. Although our review was limited to retrospective analysis of data from a single family medicine department, the results suggest that proper RN and physician training coupled with the use of clinical reminder systems can significantly improve the number of AAPs provided to primary care patients.
Conclusion
Practices with low AAP completion rates may find a team-based approach helpful in increasing the provision of written AAPs for patients with persistent asthma.
Acknowledgments
The authors gratefully acknowledge the support of Lee Green MD and Timothy Morris MS from the Department of Family Medicine at the University of Michigan for their assistance with data collection for this project.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication April 29, 2011.
- Revision received September 1, 2011.
- Accepted for publication September 6, 2011.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Impact of team-based community healthcare on preventable hospitalisation: a population-based cohort study in Taiwan
- Interdisciplinary Primary Care Team Expertise and Diabetes Care Management
- Use of Asthma APGAR Tools in Primary Care Practices: A Cluster-Randomized Controlled Trial
- Planning for Action: The Impact of an Asthma Action Plan Decision Support Tool Integrated into an Electronic Health Record (EHR) at a Large Health Care System
- Share the Care™: Building Teams in Primary Care Practices