
Abstract
Background: National guidelines recommend different pharmacologic management of hypertension (HTN) without comorbidities for Black/African Americans (BAA) compared with non-BAA. We sought to 1) identify if these recommendations have influenced prescription patterns in BAA and 2) identify the differences in uncontrolled HTN in BAA on different antihypertensive medications.
Methods: We constructed a linked retrospective observational cohort using 2 years of electronic health records data, comprising of patients aged 18 to 85 with HTN on 1- or 2-drug regimens, including angiotensin-converting enzyme inhibitors (ACE), angiotensin receptor blockers (ARB), thiazide diuretics, or calcium channel blockers (CCB). We examined prescribing differences and HTN control in BAA versus non-BAA.
Results: Among 10,875 patients identified, 20.6% were identified as BAA. 46.4% of BAA had uncontrolled HTN (≥140/90 mmHg) compared with 39.0% of non-BAA (P < .001). 61.8% of BAA were treated with 1-drug compared with 68.4% of non-BAA. Of BAA on monotherapy: 41.3% were on thiazide, 40.1% on CCB, and 18.6% on ACE/ARB. Of non-BAA on monotherapy, 27.7% were on thiazide, 30.1% were on CCB, and 42.3% were on ACE/ARB. Of BAA patients on 1 drug, 45.2% had uncontrolled HTN compared with 38.0% of non-BAA (P < .001). Of BAA on 2 drugs, 48.2% had uncontrolled HTN compared with 41.1% non-BAA (P < .001). For each drug regimen, there was more variation in HTN control within each group than between BAA and non-BAA.
Conclusions: Providers seem to be following race-based guidelines for HTN, yet HTN control for BAA remains worse than non-BAA. An individualized approach to HTN therapy for all patients may be more important than race-based guidelines.
Background
Race-based guidelines for medical care have recently become controversial.1⇓⇓⇓⇓⇓–7 Skin color is increasingly recognized as a poor proxy for precision medicine, and many have highlighted the potential harms of using race as a factor in clinical decision-making.4,7⇓⇓–10 For example, well-intentioned medical organizations, relying on data from clinical trials, have long recommended different standards for interpreting kidney and pulmonary function testing for Black/African Americans (BAA) compared with others, even as many have suggested that relying on such guidelines may lead to delayed diagnosis and treatment for BAA populations. 2,6,11⇓⇓–14 In this context, it may be valuable to reevaluate widely accepted race-based guidelines for managing hypertension (HTN) in BAA.15 The Eighth Joint National Committee in 2014 (JNC8), the American College of Cardiology/American Heart Association in 2017 (ACA/AHA), and European Society of Cardiology 2018 guidelines all recommend a unique approach to initial therapy for BAA, stating that individuals in this group without comorbidities should receive either a thiazide diuretic or a calcium channel blocker (CCB) as initial therapy, whereas angiotensin-converting enzyme inhibitors (ACE) and/or angiotensin receptor blockers (ARB) should be considered as initial therapy only for BAA with certain comorbidities while non-BAA individuals can be prescribed any of those 3 classes of medicines regardless of comorbidities.16⇓–18 These guidelines echoed sentiments in the International Society on Hypertension in Blacks (ISHB) consensus statement in 2010 that recommended that first-line treatment consist of a thiazide diuretic or CCB over an ACE/ARB in BAA populations, but not other populations.19
Race-based HTN treatment guidelines have been based on evidence from clinical trials and intended to rectify disparities in HTN control in BAA populations.20,21 However, the interpretation of this evidence has come under scrutiny.15 JNC8 and ACA/AHA recommendations are based on results from the Anti-HTN and Lipid-Lowering treatment to Prevent Heart Attack Trial (ALLHAT) and the African American Study of Kidney Disease and Hypertension study (AASK). ALLHAT found in the primary outcome of coronary heart disease there was no difference for BAA when using thiazide, CCB, or ACE. While based on a prespecified secondary outcome of strokes, there was a significant benefit from using CCB/thiazide medications compared with ACE for BAA. However, this finding has been challenged, as the treatment regimen for patients on ACE included a β blocker, which is no longer considered an appropriate regimen for any patient with HTN and no other comorbidities.15,22 The AASK Trial evaluated BAA populations with chronic kidney disease and the effects of medications in those populations. While ACE was not as effective at lowering blood pressure (BP) in BAA, it was found that they did prevent the progression of kidney disease.23 It has been pointed out that avoiding ACE to treat BAA with uncomplicated HTN could lead to worse outcomes for those whose progression of kidney disease is not immediately recognized in primary care.15,24
Given the current concerns about health equity in the United States, we must examine whether and how race-based guidelines for HTN treatment have influenced the practice patterns of primary care clinicians and whether there is evidence of a beneficial impact from following such guidelines on clinical outcomes for BAA with HTN. In this study, our objective was to evaluate electronic health record (EHR) data to identify if these race-based guidelines have influenced health care provider prescribing practices in BAA groups and evaluate the HTN control for BAA and non-BAA patients with uncomplicated HTN who were prescribed 1 or 2 drugs. We additionally examined predictors of uncontrolled HTN among BAA patients.
Methods
Study Design
This study is a retrospective, observational cohort analysis using 2 years of linked EHR data from 3 health systems affiliated with the San Francisco Bay Collaborative Research Network (sfbaycrn.org). The 3 health systems were comprised of 1 academic and 2 county-run systems with a total of 31 primary care clinics. The study included all patients aged 18 to 85 years at the beginning of the study period with a hypertension diagnosis and at least 1 primary care provider care visit between October 15, 2013, and October 14, 2015, for 2 of the 3 health systems, and between May 1, 2014, and April 30, 2016, for the third health system. These 2-year periods were different due to local constraints and Health System 1 to pull data retrospectively to match the dates from the other 2 health systems. All the data were collected using a 1-time extraction of EHR data. HTN diagnosis in each was defined using the Ninth International Classification of Disease visit diagnosis codes 401 and 405 during the study period or a problem list diagnosis indicating “hypertension.” Initial exclusion criteria during data extraction were pregnancy-related HTN and end-stage renal disease.
Study Population
For this subset analysis, inclusion criteria encompassed: 1) patients on 1-drug regimens that included either ACE/ARB, thiazide, or CCB; 2) patients on 2-drug regimens on ACE/ARB and/or thiazide and/or CCB. Exclusion criteria included: individuals with diabetes, chronic kidney disease (CKD), not currently on any HTN medications, on 3 or more HTN medications, or 1- or 2-drug regimens including drugs other than ACE, ARB, thiazide, or CCB. Patients with diabetes and CKD were excluded as we did not have data on microalbuminuria, a case in which ACE/ARB are indicated as the first line in BAA populations per national guidelines. Patients on 3 or more medications were excluded as this meets the diagnosis of resistant HTN and is outside the scope of this study. Finally, patients on other medications other than ACE/ARB, thiazide, or CCB were excluded as they are not recommended for initial HTN therapy in any guideline recommendations.
Measurements
The primary outcome was prescription patterns in BAA and non-BAA groups. Our secondary outcome of interest was uncontrolled HTN at a patient's most recent primary care visit, which we defined as a BP reading of stage 2 HTN or greater (≥140/90 mmHg). Controlled HTN was considered Stage 1 HTN or below (<140/90 mmHg). We chose this cutoff because there are multiple recommendations for optimal BP for adults, elderly adults, and BAA in particular. JNC8 guidelines recommend that for adults 18 to 59 years of age, <140/90 mmHg is the ideal goal, while adults 60 years or older without comorbidities should have a treatment goal of <150/90 mmHg.16 ACA/AHA guidelines recommend a treatment goal for all adults to be <130/80 mmHg regardless of age.17 The European Society of Cardiology recommends for adults aged 18 to 59 years, treatment goals should be <130/90 mmHg, and for adults 60 years and older, the goal should be <140/90 mmHg.18 Finally, the ISHB consensus statement recommends a goal BP of <135/85 mmHg in BAA without comorbidities in all ages. We chose our cutoff for all ages because it represented a compromise between the different guidelines, balancing the more stringent ACA/AHA guidelines and the relatively liberal JNC8 guidelines for different age groups. Furthermore, clinician leaders representing these practices settings in our practice-based research network agreed that this cutoff represents a level of control that would be expected to trigger additional intensified medical therapy.
We also collected race and ethnicity (as identified in the EHR), age, sex, body mass index (BMI, calculated from height and weight data), smoking status, preferred language, insurance status, and number of primary care visits during the 2-year study period. Age, BMI, smoking status, and insurance status were collected for the first visit during the study period. For the purpose of this study, a list of all the medications listed as currently prescribed for HTN was pulled in the 1-time extraction of EHR data at the last visit available. Medications (including combination drugs) were broken down into respective medicines and classes.
Analysis
We reported population characteristics stratified by BAA population and non-BAA population. Initial analyses evaluated proportion of cohorts with controlled HTN or uncontrolled HTN on 1- and 2-drug regimens using the proportional z-test. In addition, we examined median systolic and diastolic BP (SBP and DBP) for all participants on each possible treatment regimen, stratified by BAA and non-BAA. We used Pearson's χ2 test for bivariate analysis of categorical data and Student's t-test for continuous data. Multivariate logistic regression models were used to evaluate the association of uncontrolled HTN for both 1- and 2-drug regimens in the BAA subgroup with the following covariates: age as a continuous variable, insurance status (categorical variable: insured, uninsured, and unknown), number of primary care provider (PCP) visits over the 2-year study period (categorical variable: 1 to 2, 3 to 4, or ≥5 visits), and health system where primary care was delivered.
All analyses were performed with SAS 9.4 and STATA 16 data analytics software. The value of P = .05 was used as the cutoff level for statistical significance. Further details on our methods to define our research cohorts and extract/clean/link data from the EHR data can be found in an earlier publication.25 The Institutional Review Board approved the study at the University of California, San Francisco, with a waiver for informed consent.
To improve transparency, we followed the REporting of studies Conducted using Observational Routinely collected health Data (RECORD) guidelines when presenting our study.26
Results
Sociodemographic and Baseline Characteristics
For our subset analysis, 10,875 participants met inclusion criteria. Mean age for this cohort was 56.2 (standard deviation [SD], 12.0) years. The majority (57.8%) of the cohort were female, 94.0% had some form of health insurance (private, Medicare, or Medicaid), and 18.3% were current smokers. One-fifth (20.6%; n = 2245) of the cohort were identified as BAA in the EHR. Of note, a higher proportion of BAA were smokers (38.7%) compared with non-BAA (13.0%) (P < .001), and a higher proportion of BAA was obese (BMI ≥ 30) (52.2%) as compared with non-BAA (34.9%) (P < .001). (Table 1).
Sociodemographic and Baseline Characteristics
Pharmacological Treatment Characteristics
Of the total cohort, 67.1% were on 1-drug regimens and 32.9% were on 2-drug regimens. Among BAA patients, 61.8% were on 1-drug and 38.2% were on 2-drug regimens; whereas 68.4% of non-BAA patients were on 1-drug regimens and 31.6% were on 2-drug regimens. Among BAA patients on 1-drug regimens: 41.3% were on thiazide, 40.1% on CCB, and 18.6% on ACE/ARB. Among non-BAA patients on 1-drug regimens: 27.7% were on thiazide, 30.1% on CCB and 42.3% on ACE/ARB. Among BAA patients on 2-drug regimens: 35.8% were on thiazide+CCB, 44.3% on thiazide+ACE/ARB and 19.8% were on CCB+ACE/ARB. Among non-BAA patients on 2-drug regimens: 19.8% were on thiazide+CCB, 49.4% on thiazide+ACE/ARB and 30.8% on CCB+ACE/ARB. (Table 2)
Pharmacological Treatment Characteristics
Median Blood Pressure by Race and by Drug Regimen
Median SBP and DPB for each treatment regimen for BAA and non-BAA populations did not exceed 140 mmHg or 90 mmHg. (Figures 1a and 1b) There were minimal between-group (BAA vs non-BAA) differences in median blood pressure for any regimen. There was some within-group variation. For BAA patients on 1-drug regimens, those on thiazides had the lowest observed median SBP (134 mmHg), while those on ACE/ARB had the lowest observed median DBP (82 mmHg). For non-BAA patients on 1-drug regimens, those on ACE/ARB had the lowest observed median SBP (133 mmHg), and those on CCB and ACE/ARB had the lowest observed median DBP (79 mmHg). For BAA patients on 2 drug regimens, those on thiazide+ACE/ARB had the lowest observed median SBP (135 mmHg) while those on CCB+ACE/ARB had the lowest observed median DBP 82 mmHg). Among non-BAA patients on 2 drugs, those on thiazide+ACE/ARB had the lowest observed median systolic BP (132 mmHg), while those on CCB+ACE/ARB had the lowest observed median diastolic BP (78 mmHg).
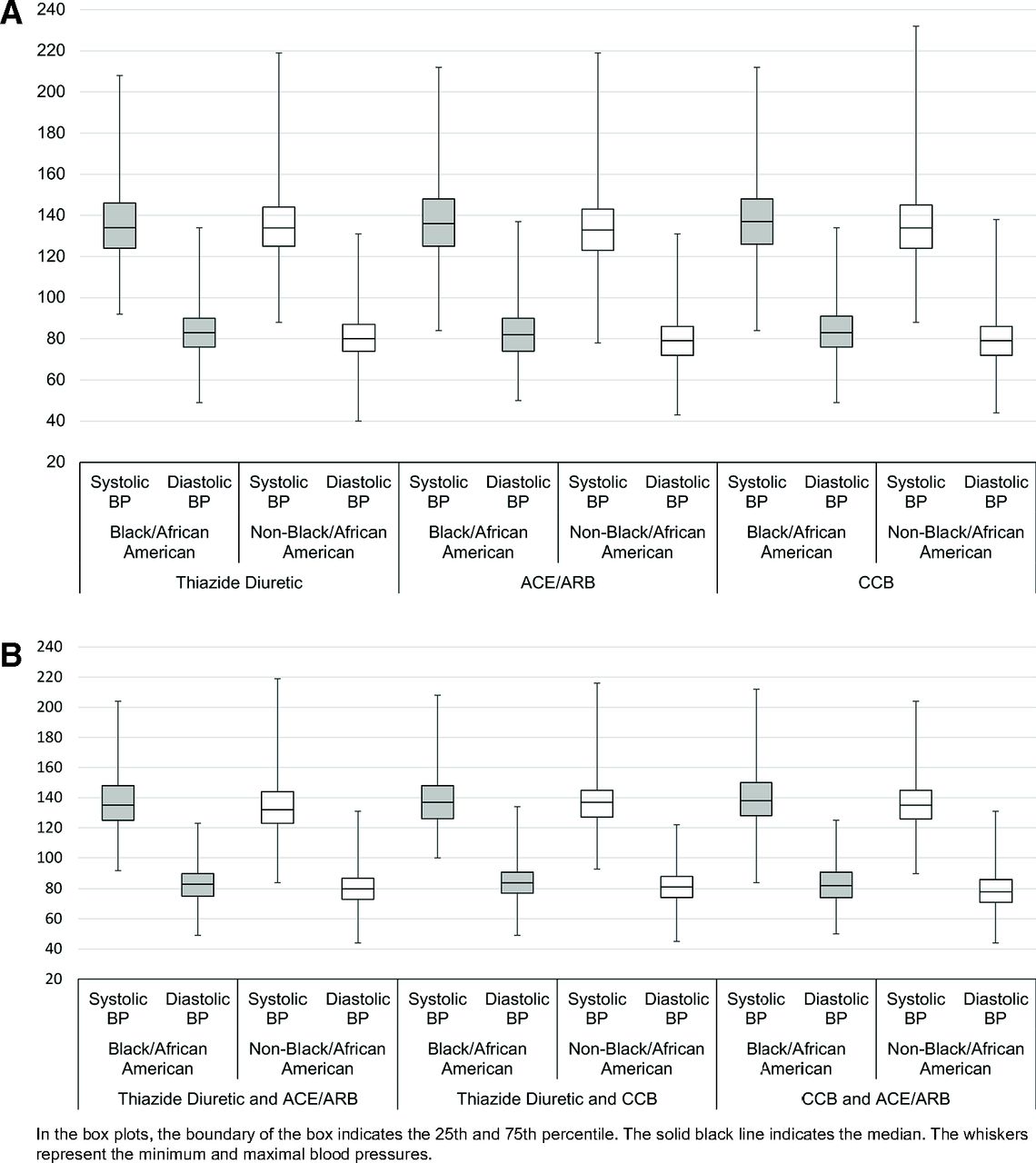
Median and interquartile ranges of blood pressures for Black/African Americans and Non-Black/African Americans on 1-drug regimens. Figure 1b) Median and interquartile ranges of blood pressures for Black/African Americans and Non-Black/African Americans on 2-drug regimens. Abbreviations: BP, Blood Pressure; CCB, Calcium Channel Blocker; ACE, Angiotensin-Converting Enzyme Inhibitor; ARB, Angiotensin Receptor Blocker.
HTN Control by Race
Overall, more of the BAA patients had uncontrolled HTN (BP ≥140/90mmh) compared with the non-BAA patients (46.4%; 95% CI, 0.44-0.48 vs 39.0%; 95%CI, 0.38-0.40; P < .001). Of BAA patients on 1-drug regimens, 45.2% (95% CI, 0.43-0.48) had uncontrolled HTN compared with 38.0% (95% CI, 0.37-0.39) of non-BAA (P < .001). Of BAA patients on 2-drug regimens, 48.2% (95% CI, 0.45-0.52) had uncontrolled HTN compared with 41.1% (95% CI, 0.39-0.43) of non-BAA (P < .0001).
Odds of Uncontrolled Blood Pressure among BAA Patients
In our adjusted models, we found that BAA patients on 1-drug regimens including CCB and ACE/ARB medications had higher odds of uncontrolled HTN compared with BAA patients on thiazides (adjusted odds ratio [aOR]=1.53; 95% CI, 1.19-1.97 and aOR = 1.70; 95%CI, 1.25-2.33, respectively). Of BAA patients on 2-drug regimens, there were no significant differences between the 3 treatment combinations. Of note, BAA patients with more than 2 visits to their primary care providers during the study period had significantly lower odds of uncontrolled HTN than those with only 1 to 2 visits. (Table 3)
Odds of Uncontrolled Blood Pressure (≥140/90 mmHg) Among Black/African American Patients on One- and Two-Drug anti-Hypertensive Regimens
Discussion
Our study revealed that prescribing practices for uncomplicated HTN were markedly different for BAA versus non-BAA populations in the health systems we examined, with a strong preference for thiazide diuretics and CCB as initial monotherapy and relatively less use of ACE/ARB in 1-drug or 2-drug regimens for BAA patients. This indicates that primary care clinicians in these settings have, to a large extent, been practicing in accord with race-based HTN treatment guidelines that have been developed and disseminated in the last decade. Despite these findings, we also found evidence of continued disparities in HTN control for the BAA group relative to those in the non-BAA group, regardless of the treatment selected. Though BAA patients in this cohort who were prescribed thiazides did have better blood pressure control on average than those on monotherapy with other medications, we did not observe such benefits for individuals prescribed CCB, and across all drug regimens for both BAA and non-BAA, there was far more variation within groups than between groups, suggesting that response to medication prescribed is highly individual, regardless of race.
Our findings suggest that race-based hypertension prescribing guidelines have influenced clinical practice but likely with relatively limited benefit for BAA patients. Other factors may be more important than choice of drug based on skin colors, such as dose titration, the addition of second or third drugs, medication adherence, dietary and lifestyle interventions, such as advocating for smoking cessation, reducing alcohol consumption, and achieving weight loss. Our finding that more frequent clinical follow-up was associated with hypertension control among the BAA patients suggests that there may have been more time during more frequent visits to attend to these important clinical factors.
In addition, social and environmental factors that can contribute to hypertension disparities, such as lack of access to healthy food, unstable housing, social isolation, difficulties paying bills, may also be important risk factors that deserve greater attention.15 Finally, a factor that deserves specific focus is the role of implicit bias in medicine. It has long been known that race plays an implicit and often negative influence on clinician decision-making.27 Many studies have shown that BAA often receives poorer care and less referrals than non-BAA populations.27⇓⇓–30 At the least, race-specific medication guidelines provide a poor proxy for precision medicine, and at worst they may reinforce negative stereotypes suggesting that BAA patients are both genetically different from other races and that they should therefore be presented with a more limited set of treatment options. These guidelines may also distract clinicians from a more important type of precision medicine, including targeted interventions that address known social determinants of health and a clinician's own implicit biases that disproportionately and negatively impact BAA patients.31⇓⇓–34 Furthermore, use of these race-based HTN guidelines could have negative clinical consequences for BAA patients. For example, BAA has up to 4 times the prevalence of CKD, and 1 potential reason could be delayed use of ACE/ARB medications in the early stages of CKD due to reliance on race-based clinical guidelines.35 Further study is needed to understand if preferentially avoiding ACE/ARB in BAA could contribute to well-documented disparities in long-term HTN outcomes. Finally, BAA patients do not make up a monolithic group; instead, individuals present a rich array of experiences and circumstance, and each person deserves to be treated as a unique individual.36,37 Instead of using race as a proxy for precision medicine, we should be searching for more biologically sound pharmacogenomic approaches that are precise and individualized.
Our study, which relies on cross-sectional clinical data, had several limitations. First, our study used EHR reported race/ethnicity. EHR reported race often underestimates BAA race when compared with self-report.38 Next, we may not have excluded all individuals with comorbidities from our analyses, as the accuracy of such data in the EHR is dependent on clinician documentation. In addition, in our analyses, we did not have access to drug doses or changes in medication prescribing patterns that may have taken place over time. Furthermore, medication lists can be inaccurate due to poor documentation. Another important limitation is this study's inability to control how blood pressure was measured. There are potential differences in how individual health care providers and clinics within and across the health systems collect blood pressure readings. This inconsistency could be reflected in our data. Another consideration is medication adherence. EHR data cannot measure adherence to medication regimens accurately, and this study was not aiming to estimate adherence to medications.39 However, while these EHR-related limitations are real, they should be evenly spread across the entire cohort and equally distributed across BAA and the non-BAA subgroups. Finally, though the population studied was socioeconomically and racially heterogeneous, our study was conducted in the San Francisco Bay Area, and our findings may not be generalizable to other geographical areas in the United States. Future studies could address these limitations to provide more definitive conclusions to our research questions.
In conclusion, our study shows that while primary care providers often seem to follow race-based prescribing recommendations for HTN, disparities in HTN control for BAA patients relative to other populations persist. While race-based HTN guidelines are well-intentioned, now is the time for more research to understand better the clinical outcomes and possible unintended negative consequences of such guidelines for individuals they are intended to help.
Acknowledgments
The authors would like to acknowledge the clinical leaders and medical informatics teams at each health system without whose participation and assistance this research would not have been possible.
Notes
This article was externally peer reviewed.
Funding: This research was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (UL1 TR001872). JKH was supported by the National Research Service Award (NRSA) grant (T32HP19025).
Conflict of interest: The authors declare that they have no conflicts of interest.
Availability of data and materials: The study protocol, raw data, and/or programing code supporting the conclusions of this article are available from the corresponding author on reasonable request.
To see this article online, please go to: http://jabfm.org/content/35/1/26.full.
- Received for publication July 6, 2021.
- Revision received August 24, 2021.
- Accepted for publication August 25, 2021.




{kind=link}