
Abstract
Introduction: Despite the Affordable Care Act's insurance expansion, low-income Latinos are less likely to have a primary care provider compared with other racial/ethnic and income groups. We examined if community-based health care navigation could improve access to primary care in this population.
Methods: We surveyed adult clients of a community-based navigation program serving predominantly low-income Latinos throughout Los Angeles County in 2019. We used multivariable logistic regression models, adjusting for sociodemographic characteristics, to calculate odds ratios for differences in access to primary care and barriers to care between clients who had experienced approximately 1 year of navigation services (intervention group) and clients who were just introduced to navigation (comparison group).
Results: Clients in the intervention group were more likely to report having a primary care clinic than the comparison group (Adjusted Odds Ratio [aOR] 3.0, 95%CI: 1.7, 5.4). The intervention group was also significantly less likely to experience several barriers to care, such as not having insurance, not being able to pay for a visit, and not having transportation.
Conclusions: Community-based navigation has the potential to reduce barriers and improve access to primary care for low-income Latinos. In addition to expanding insurance coverage, policymakers should invest in health care navigation to reduce disparities in primary care.
- Access to Health Care
- Affordable Care Act
- Health Policy
- Hispanic Americans
- Los Angeles
- Minority Health
- Poverty
- Primary Health Care
Introduction
Primary care plays a critical role in providing patients with high-quality care through disease prevention and management.1 Yet fewer than two thirds of Latinos report having a primary care provider.2 Disparities in access to primary care are most pronounced for Latinos and persons with lower incomes.3⇓–5 While having insurance is strongly associated with access to routine care, barriers such as out-of-pocket costs, narrow networks, and provider availability can impede use of necessary services.6 Implementation of the Affordable Care Act (ACA) significantly reduced uninsurance rates, including for Latinos and those with low incomes; however, equivalent gains in access to primary care were not similarly achieved.5,7⇓⇓–10 For example, in California, in the year after the ACA's expansion, low-income adults with Medicaid (free or near-free public insurance for low-income people) were less likely to be accepted by a new doctor than in the year prior.11 Clearly insurance expansion alone is not sufficient to mitigate disparities in health care access.
Aside from uninsurance, several factors may contribute to lower rates of access to primary care among low-income Latinos, including immigration status, language barriers, lower levels of education, and low rates of public and private insurance acceptance among primary care providers.12⇓⇓⇓⇓–17 In combination, these factors further exacerbate the difficulties of navigating a complex health care system.
The problem of accessing primary care is particularly acute in Los Angeles County, where almost half of the residents identify as Hispanic or Latino, and 1 in 5 live below the federal poverty level. Yet after the ACA's implementation, a third or more of residents from these communities report difficulty getting medical care when they need it.18,19 In addition, hundreds of thousands of undocumented immigrants living in Los Angeles are generally ineligible for comprehensive Medicaid or subsidies to purchase plans on the state's ACA marketplace.20 Like most states, California's Medicaid program relies on a largely managed care system. Many residents find the complex network of managed care plans and independent provider associations challenging to navigate, further complicating their ability to get needed care.21,22 Qualitative interviews with Los Angeles County safety-net patients suggest that systemic barriers—long wait times for an appointment, difficulty finding an accepting provider—and gaps in knowledge about the health care system can contribute to decreased use of primary care.23
Health care navigators can complement the ACA's coverage expansion initiatives by helping people find and use health care services.24⇓⇓–27 Effective programs tend to include frequent interactions between navigators and their clients.28⇓⇓⇓–32 One study of a neighborhood-based intervention to identify and provide health care resources to Latinos through community health events found that primary care use increased for study participants 1 year later.33 This study was limited to examining the effects of 5 health events in 2 suburban neighborhoods in North Carolina, and the prepost outcome analysis did not include statistical testing. Yet most studies examining the impact of navigation programs have been focused on those initiated in a clinical (emergency department or hospital-based) as opposed to community setting.34⇓⇓⇓–38 To our knowledge, few studies have examined how community-based navigation programs might improve access to primary care for low-income Latinos, a population with 1 of the lowest rates of primary care use in the country.
The Los Angeles County Children's Health Outreach Initiative (CHOI) program, operated by the Los Angeles County Department of Public Health, funds and coordinates health care navigation services for people of all ages. While there are many community organizations that assist with insurance outreach and enrollment, CHOI employs a multitouch model of outreach, enrollment, utilization, and retention/renewal (OEUR) to foster long-term access to health care.39 CHOI's trained navigators, often recruited from the targeted communities, organize outreach events (such as community presentations on the benefits of insurance), enroll eligible clients in insurance plans, help clients make medical appointments, refer clients to social services, and facilitate insurance renewal.40 As part of the OEUR model, navigators are trained to help clients find an appropriate primary care clinic or provider. In addition, CHOI navigators engage in several formal “touches” or follow-up calls with their clients—at 30 days, 6 months, and 11 months after intake—to ensure that their clients are receiving necessary health services. The community-based CHOI agencies served more than 10,000 people from 29 different locations throughout Los Angeles County in 2019. An internal audit of CHOI agencies showed that 75% of CHOI clients were still enrolled in health care coverage 14 months after their initial intake.41 While the CHOI agencies have demonstrated their capacity to enroll clients in health care coverage, whether they effectively help their clients access primary care and overcome barriers to health care is not known.
In this study, we examine the impact of a community-based navigation program with an OEUR model on access to primary care for a predominantly low-income Hispanic population. We also evaluate the effects of community-based navigation on reducing specific barriers to primary care.
Methods
We conducted a quasi-experimental evaluation of CHOI navigation using surveys of CHOI clients who had received 11 to 13 months of CHOI services (intervention group) and clients who had only received an initial intake appointment with CHOI agencies (comparison group). We have 2 main outcomes: having a primary care clinic and having a regular provider. We defined a primary care clinic as a “clinic, health center, hospital clinic, doctor's office, Kaiser or HMO where 1 goes for regular or primary care.” We defined a regular provider as 1 or more personal doctors or primary care providers, including general doctors, physician assistants, or nurse practitioners but excluding specialists. Additional outcomes included having a checkup in the past year (only asked if patients had a primary care clinic), difficulty getting medical care when needed, and having an emergency department visit in the past year that did not result in a hospitalization. Lastly, we asked participants if they experienced barriers that may have led to delaying or avoiding care, including insurance and cost-related barriers, clinic-level barriers, and knowledge barriers. All outcomes are self-reported.
Study Setting and Participants
We selected 9 community-based CHOI agencies, with 29 different sites located throughout Los Angeles County, in the study. The agencies are geographically distributed across Los Angeles and use navigators that are representative (linguistically and culturally) of the population they serve. The agencies operate independently but are funded by the Department of Public Health to conduct health care navigation as part of CHOI. In addition, the agencies use the same OEUR model, have a shared electronic record system for all clients (allowing clients to be followed across agencies and longitudinally), and have monthly meetings and trainings to ensure consistent process across agencies and sites. Clients were referred to CHOI agencies from the health care system (hospital, emergency department, clinic, or health plan) or the community (friend or family member, school, Women, Infants, and Children program, other community agencies, brochure or advertisement, Department of Public Social Services, or the Los Angeles County information hotline).
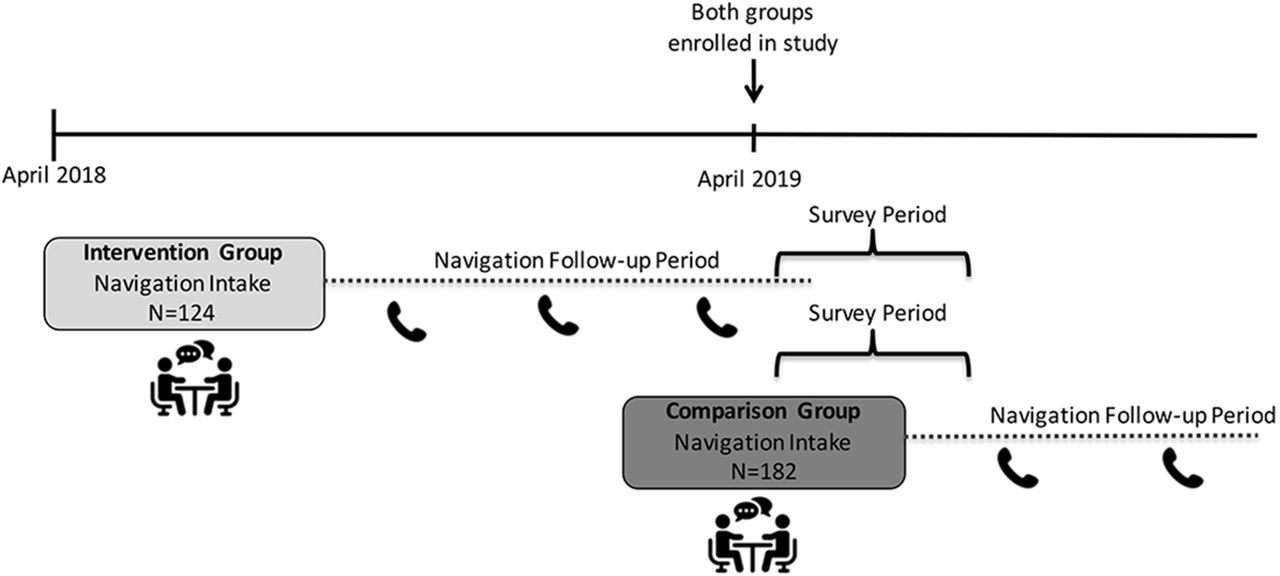
We surveyed 2 groups of CHOI clients: an intervention and a comparison group. We recruited participants in the comparison group from new CHOI clients presenting for their initial intake appointment. These clients had an intake appointment between April and October 2019 to assess their insurance and health care access needs but had not received follow-up navigation from CHOI navigators. Participants in the intervention group had their intake appointment with CHOI between February and November of 2018, 11 to 13 months before being surveyed. CHOI navigators had called these clients 30 days and then 6 months after their intake to assist with additional insurance enrollment or health care access needs. This included assisting clients with finding a clinic or primary care provider that was in their insurance plan network, language and gender concordant (if requested), and geographically accessible. Navigators may have provided additional support for services such as assistance with medical transportation, paying medical bills, or filling out medical forms, when necessary. We recruited participants in the intervention group from clients contacted as part of routine 11 to 13 month follow-up after their intake appointment.
CHOI navigators recruited both intervention and comparison group participants on a rolling basis, between April and October of 2019. Eligible study participants were CHOI clients between the ages 18 to 64, and spoke either English or Spanish (Figure 1). During recruitment, CHOI navigators assessed clients' eligibility and collected basic demographic information including race/ethnicity, age, employment, education level, and insurance or health care coverage type. Navigators provided eligible and interested clients with a study phone number and informed them that they would receive a phone call from a research assistant within a week. After recruitment, research assistants from the study team who were trained in conducting phone surveys attempted to contact interested clients in their preferred language (English or Spanish) up to 3 different times. Participants who completed the 10 to 15 minute long survey received a $10 gift card. All study activities were approved by the Department of Public Health's Institutional Review Board.

Study design.
Survey Design
We primarily used or modified existing validated survey questions on access to care, health care use, and general health to develop our survey instrument (see the Appendix).19,42 We translated the survey from English to Spanish and then back translated the questions to ensure accuracy. Questions asking about specific barriers to care had been cited in the literature or were barriers frequently observed by CHOI navigators. Surveys were reviewed by CHOI navigators, pretested with CHOI clients in both English and Spanish, and modified to improve question comprehension and increase the instrument's validity and reliability.
Statistical Analysis
We calculated differences in sociodemographic characteristics between the intervention and comparison group and compared them using a chi square (or Fisher's exact) test. We calculated unadjusted percentages of outcomes and barriers for the comparison and intervention groups. We created multivariable logistic regression models to calculate odds ratios and confidence intervals for differences in outcomes and barriers between the comparison and intervention groups. The models adjusted for age, race/ethnicity, sex, education, language, federal poverty level (FPL), employment, self-reported health status, and referral source. All tests were 2-sided with an α level set at 0.05 for statistical significance. All analyses were performed using Stata 16.1 (StataCorp, College Station, TX) and SAS 9.4 (SAS Institute, Cary, NC).
Results
We surveyed 306 participants: 182 (59%) in the comparison group and 124 (41%) participants in the intervention group (Table 1). Of the 442 clients who were screened and found to be eligible for the study, 69% completed the survey. Response rates were similar between the comparison and intervention groups. Most participants in both groups were Hispanic and had incomes below 100% of the FPL. The majority were referred to the CHOI program from community organizations rather than from the health system. Participants in the intervention group were more likely to be 45 years or older (35% vs 22%, P < .001), not have completed high school (70% vs 49%, P < .004) and consider Spanish to be their primary language (86% vs 68%, P < .001) compared with the comparison group. Most chose to take the survey in Spanish.
Characteristics of Study Participants
Participants in the intervention group were 3 times more likely to report having a primary care clinic (adjusted odds ratio [AOR] 3.0, 95% CI, 1.7, 5.4) and more than 2 and a half times more likely to report having a primary care provider (AOR 2.6, 95% CI, 1.5, 4.4) compared with participants in the comparison group (Table 2). Participants in the intervention group were also 60% less likely to report having a somewhat or very difficult time getting care when they needed it (AOR 0.4, 95% CI, 0.2, 0.6). There was no significant difference between the groups in having a checkup (AOR 1.9, 95% CI, 0.7, 4.9) or an emergency department visit that did not result in a hospitalization in the past year (AOR 1.0, 95% CI, 0.4, 2.4). To isolate the impact of community navigation beyond insurance enrollment, we examined a subgroup of participants with Emergency Medicaid, which provides coverage only for an emergency department visit and associated hospitalization for most people. These people were ineligible for comprehensive insurance. We found that 68% of those with Emergency Medicaid in the intervention group had a primary care clinic compared with 37% in the comparison group (P = .002) (Appendix Table A1).
Differences in Access to Primary Care and Health Care Use Among Children's Health Outreach Initiative (CHOI) Clients
More than 80% of participants in the comparison reported having a barrier compared with 69% of people in the intervention group (data not shown). The most common barrier cited in both comparison and intervention groups was lack of health insurance (Table 3). Clients in the intervention group were less likely to experience several barriers to primary care, including not having health insurance (AOR 0.3, 95% CI, 0.2, 0.5), not being able to afford to pay for a visit (AOR 0.4, 95% CI, 0.3, 0.7), not having a usual source of care (AOR 0.4, 95% CI, 0.2, 0.7), not knowing how or where to get care (AOR 0.4, 95% CI, 0.2, 0.7), and not having transportation (AOR 0.4, 95% CI, 0.2, 0.9) (Table 3). CHOI services were not associated with reductions in other barriers, including visit(s) not being covered/approved by a health plan, not getting a timely appointment, not being able to contact the clinic, not liking their clinic or provider, long wait times to see a doctor, clinic being closed, not being able to take time off work to get care, fear of getting medical care, and language, communication, or cultural barriers.
Differences in Barriers to Medical Care Among Children's Health Outreach Initiative (CHOI) Clients
Discussion
We found that community-based health care navigation that used the OEUR model was associated with improved access to primary care among low-income Latinos. Although barriers to primary care were prevalent among all participants, clients who underwent community-based navigation experienced fewer barriers, particularly barriers related to insurance, cost of care, and knowledge.
While other studies have demonstrated patient navigation can effectively increase rates of primary care visits, most navigation interventions were initiated in the clinical setting, after an emergency department visit or hospitalization, and typically focused on patients with multiple comorbidities or those that had a higher risk of hospital readmission.28⇓⇓⇓–32 We examined a community-based navigation program, which can open the door to primary care for those who have had limited experience with the health system. In addition, the agencies we studied serve primarily low-income Latinos, a group that suffers from lower rates of primary care. Similarly to other successful navigation interventions, the OEUR model employs several “touches,” or interactions with clients, to provide clients with assistance on multiple occasions. We speculate that the improved access to care may have been partially mediated by enrolling patients in insurance. However, since those without comprehensive insurance coverage (Emergency Medicaid) in the intervention group were also more likely to have a primary care clinic than their counterparts in the comparison group, we also believe that assisting clients with other barriers to care, such as the cost of care, transportation, and where to get care, were instrumental in increasing access to primary care. Notably, clinic-level barriers, such as obtaining a timely appointment and difficulty contacting the clinic, were prevalent and equally problematic in both the comparison and intervention groups. Given the predicted physician shortage the nation is facing, efforts to improve clinic accessibility by increasing our safety-net-serving primary care workforce are critically important.43 Bringing Medicaid reimbursement rates to be on par with Medicare or private insurance is a first step to increasing Medicaid acceptance rates among providers and potentially growing the workforce. Expansion of safety-net clinic hours, with adequate support and compensation for providers and staff, could also help to improve access for working families. In addition, while initiatives that promote continuity of care in the safety net and grow the racial/ethnic diversity of providers may not directly impact access to care, they are important for the patient experience and quality of care and could improve primary care use.44,45
It is also important to consider the underlying factors that drive the need for health care navigation in the United States. Care fragmentation caused by high rates of insurance churning (loss and gain of insurance), changes in insurance plans, and narrow or changing provider networks can leave people confused about where and how to get care or worried that they will incur unaffordable out-of-pocket costs. In the United States, access to insurance and the type of insurance (ACA marketplace or employer based or Medicaid) can change based on a person's income, employment status, and immigration status. Care fragmentation for low-income persons is associated with disruptions in physician care and medication adherence and negative health outcomes.46 In California, as is the case in most states, Medicaid services are organized using managed care plans, which in turn contract with independent provider organizations. While such contracting may reduce health care costs, it also limits where enrollees can go to get care, potentially reducing both the number of visits and continuity of care.47
Several limitations in our study should be noted. First, the intervention group only included participants who navigators could reach by phone a year after their intake. Thus, we may have included participants with more stable life circumstances and perhaps, by relation, more stable access to care, in the intervention group. However, participants in the intervention were less likely to speak English and had a lower level of education compared with the comparison group, characteristics that are associated with lower rates of primary care. Though we did adjust for these differences in addition to other characteristics, there may have been unmeasured confounders that we could not adjust for. Second, we surveyed the comparison group soon (median time of 9 days) after their intake, yet clients may have benefited from navigation services during that period, thus not fully reflecting their challenges with accessing care before receiving community-based navigation. Third, we relied on self-reported outcomes and were unable to verify primary care empanelment or office visits. We worked with the community agencies to develop a feasible study design to measure the impact of their program in a short period of time. Largely due to support from the navigation agencies and the Los Angeles Department of Public Health, we achieved a high survey completion rate. Importantly though, since this study was not a randomized controlled trial, more rigorous evaluations of community-based navigation are needed to confirm our findings.
Conclusion
Community-based health care navigation is an important supplement to insurance expansion policies that can improve access to primary care. CHOI's OEUR model of outreach, enrollment, utilization, and renewal, which employs several “touches” with clients, has the potential to be replicated elsewhere and may benefit regions with similarly high rates of insurance churning, managed care plan enrollment, immigrants, racial/ethnic minorities, and low-income people as Los Angeles County. Millions of Americans, having lost their jobs and as a result their employee-sponsored insurance during the COVID-19 pandemic, are enrolling in Medicaid and marketplace plans.48,49 There is an urgent need for enhanced community-based health care navigation that can assist people not only with finding new health care coverage but also a clinic and primary care provider. Although the previous administration's public charge policy penalizing some immigrants for using public services has been reversed, embedded fear has discouraged many immigrants from accessing health care, increasing the need for culturally sensitive, community-based navigation from a trusted source of information.50 The new administration recently increased navigator funding 8-fold from last year,51 changing course from the previous administration's dramatic cuts of nearly 90%52,53 and demonstrating a clear understanding of the critical importance of navigators.
Policy efforts both nationally and in California, such as a national or state-based single payer program, aim to decrease underlying fragmentation in health care through financing and delivery system reform.54,55 Yet these policy solutions are politically contentious and have uncertain outcomes. While broader policy solutions are necessary, the success of the CHOI program and OEUR model shows that community-based navigators are capable of narrowing the gap in access that the ACA's insurance expansion alone has been unable to completely close. By providing navigators with additional support and training to connect clients to primary care, we may begin to see concomitant gains in disease prevention and management that we hoped to achieve under the ACA.
Acknowledgments
The authors would like to acknowledge the contributions of Ashley Recinos, Ricardo Poynton, Vanessa Mariscal, Lancer Shul, and the Children's Health Outreach Initiative Agencies' directors and staff.
Appendix
Subgroup Analysis on Children's Health Outreach Initiative (CHOI) Clients with Emergency Medicaid
Notes
This article was externally peer reviewed.
Funding: This work was supported by grants UL1TR001855 and UL1TR000130 from the National Center for Advancing Translational Science (NCATS) of the U.S. National Institutes of Health and the Gehr Family Center for Health Systems Science and Innovation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest: Study authors have no conflicts of interest to report.
To see this article online, please go to: http://jabfm.org/content/35/1/44.full.
- Received for publication June 21, 2021.
- Revision received August 29, 2021.
- Accepted for publication September 9, 2021.




{kind=link}