
Abstract
Purpose: The chronic disease model suggests continuity of care and team-based care can improve outcomes for multimorbidity patients and reduce hospitalizations. Continuity of care following admission has had mixed effects on readmission rates; however, its effect before admission has not been well studied. Increased outpatient care organization and continuity before admission is hypothesized to reduce the odds of readmission.
Methods: In a cohort of 14,662 primary care patients from a Patient-Centered Medical Home (PCMH) practice, continuity of care in the 12 months before admission was assessed using 3 established metrics; usual provider continuity (UPC), dispersion continuity of care (COC), and sequence continuity (SECON). In addition, because these established metrics may not accurately reflect continuity in planned team-based care, a new metric called visit entropy (VE) was used to quantify the disorganization of visits. Multivariate logistic regression was performed to examine the relationship between readmission within 30 days and continuity while controlling for known readmission risk factors abstracted from an electronic medical record.
Results: Higher VE was associated with readmission (odds ratio, 1.10; 95% confidence interval, 1.02 to 1.19). The continuity measures of UPC, COC, and SECON were not associated with readmission.
Conclusions: Disorganized medical care, characterized by a higher VE, is associated with higher odds of readmission among hospitalized primary care patients. An association between traditional measures of continuity (UPC, COC, and SECON) and readmission was not found.
- Ambulatory Care
- Chronic Disease
- Continuity of Patient Care
- Electronic Health Records
- Entropy
- Hospitalization
- Logistic Models
- Odds Ratio
- Patient Readmission
- Patient-centered Care
- Primary Health Care
- Risk Factors
Hospital readmission within 30 days of discharge is common, occurring in almost 20% of US Medicare patients and costing $17.4 billion in 2004.1 Unplanned readmissions have often been considered a marker for poor quality inpatient care or ineffective hospital-to-home transitions.2⇓⇓⇓⇓–7 Various interventions using pharmacists and advance-practice nurses have been shown to assist patients with the transition process and reduce readmissions.7⇓⇓–10 A patient centered medical home provides a natural foundation on which to support the transition of patients from hospital to outpatient care.11
Continuity of care has been defined by the Institute of Medicine as longitudinal care by a single health-care provider coupled with effective and timely communication of health information.12 The chronic disease model suggests continuity of care and team-based care are necessary to improve outcomes for multi-comorbidity patients and reduce hospitalizations.13⇓⇓–16 Conversion from a walk-in clinic to a medical-home clinic was shown to reduce early readmissions.17 However, increased continuity of care following hospital discharge has had mixed effects on readmissions.18,19 Likewise, continuity of care has had variable effects on initial hospitalizations.20⇓–22 The effect of continuity of care before initial admission on the risk of subsequent readmission has not been well studied.
Jee and Cabana23 have classified measures of continuity of care into 5 broad categories that measure density of provider visits, dispersion of provider visits, sequence of provider visits, duration of provider relationships, and subjective patient estimates of continuity. Of these, the first 3 categories can be represented by mathematical formulae that attempt to derive a quantifiable and objective measure of continuity of care. The Usual Provider Continuity (UPC), a measure of density defined by Breslau and Reeb24 in 1975 as the fraction of visits made to the most frequent or primary physician, is commonly used in the literature to quantify continuity.23⇓⇓–26 Sequence and dispersion of provider visits are represented by the Sequence Continuity (SECON) and Continuity of Care (COC) indices respectively. UPC, SECON, and COC indices suffer from skewed distributions, division-by-zero problems, and the inability to distinguish planned referrals from random visits.27 Thus, they may be less valid in today's health care environment with an emphasis on team-based care. Visit Entropy (VE) represents a new continuity of care index that solves many of these potential shortcomings by measuring the disorganization of an outpatient visit pattern.27 It is based on well-established theory regarding entropy in physics and information science.27⇓–29 Patients who visit multiple different clinicians have a more disorganized visit pattern and hence higher VE than those who visit a limited set of clinicians frequently.
We hypothesize increased outpatient care organization and continuity in the 12 months before index hospitalization reduces the odds of 30-day readmission after controlling for demographic, utilization, and medical complexity factors. Because there is little agreement on an accepted measure of continuity of care, we have chosen to analyze the 4 measures of continuity of care (UPC, SECON, COC, VE) separately.23,25,27,30⇓–32
Methods
Cohort
A dataset of all hospitalizations of adult primary care patients at our institution during 2011 to 2013 was utilized for this study. Only patients giving consent for retrospective chart review research were included in the dataset. All patients were local community members and had an identified primary care physician at 1 of 5 primary care clinical sites located in and around Rochester, Minnesota. Each primary care clinical site is a PCMH. Patients were excluded from analysis if they were discharged from a psychiatric unit or obstetric labor and delivery. In addition, a small number of patients enrolled in an intensive care transitions management program for frail high-risk elders were excluded (441 patients). There were 26,278 admissions for 14,662 unique patients. The first inpatient hospital admission of every patient during the study period was selected for analysis. Data regarding demographics, dates of hospitalizations and emergency department (ED) visits, length of stay, the Charlson Comorbidity Index33, and 12 months of previous outpatient visits were obtained from the electronic health record. The study was reviewed and approved by the Mayo Clinic Institutional Review Board.
Continuity Measures
Four different measures, UPC, COC, SECON, and VE were used to quantify continuity in the analysis. The 4 measures represent density of provider visits (UPC), dispersion of provider visits (COC), sequence of provider visits (SECON), and the disorganization of provider visits (VE). These 4 continuity measures were explained and contrasted in detail previously.27 The formula for computing each measure from a patient's outpatient visit pattern is shown in Tables 1. VE quantifies the disorganization of a patient's visit pattern to health care providers. VE decreases in value as the continuity of care increases. It is minimized when a patient has perfect continuity of care by only visiting their primary physician, and it is maximized when a patient visits several unique clinicians once each. To illustrate the 4 continuity measures, Table 2 shows their values for several different visit patterns. In contrast with the other measures, VE is able to distinguish planned care referrals (case F) from unplanned visits to differing subspecialists (case D). In addition, VE correctly quantifies that 4 visits to the primary care physician (case H) has higher continuity than 1 or 2 visits to the primary physician (cases B and E). UPC, COC, and SECON all suffer from undefined division by zero when zero or 1 visits are observed (cases A and B). Although VE is defined even if no visits are observed, its scale depends on determining the maximum number of different potential providers. We assumed this to be the highest number of distinct providers visited by any patient in the year preceding admission (k = 62).
Formula Used to Calculate Continuity Measures
Value of Continuity Measures for Various Visit Patterns
Analysis
The dependent variable was readmission or death within 30 days of hospital discharge. The 30-day period matches the Centers for Medicare and Medicaid Services definition of hospital readmission. Although methods to adjust for potentially avoidable readmissions exist,34 we choose to consider any readmission to eliminate subjectivity. Independent variables include age, sex, marital status, Charlson comorbidity score, number of prior hospitalizations, number of prior ED visits, and length of stay.
All data were abstracted electronically and analyzed using R version 3.02 (http://www.r-project.org/). Bivariate statistics for the various factors and the dependent variable readmission were computed using a Wilcoxon rank-sum test for numeric data and Fisher exact test or χ2 test for categorical data. P < .05 were considered significant. For each measure of continuity, a multivariate analysis using logistic regression was conducted to adjust for known readmission risk factors.1,35⇓⇓⇓⇓⇓⇓⇓–43 Odds ratios with 95% confidence intervals were calculated. Direct comparison of the 4 non-nested models over the entire dataset using Akaike's Information Criterion was not valid due to the fact that the UPC, COC, and SECON models all excluded different data due to their inherent division-by-zero problem.
Results
The first admission of 14,662 patients was analyzed, and 1697 (11.6%) patients were readmitted within 30 days of discharge. Excluding ED visits on the day of admission, the median patient made 8 outpatient visits and saw 5 different health care providers in the 12 months preceding their admission. However, 473 (3.2%) patients had no outpatient visits in the preceding 12 months.
Table 3 shows descriptive statistics of the cohort and compares the 2 groups based on the dependent variable, readmission, or death within 30 days of discharge. Patients who were readmitted within 30 days were older, had a higher Charlson score, stayed in the hospital longer, and had more previous hospitalizations and ED visits. They made more outpatient visits (mean: 12.4 vs 9.8; P < .001) and saw more unique health care providers (mean: 7.7 vs 6.4; P < .001). Bivariate analysis showed their continuity of care was slightly lower as measured by UPC (0.37 vs 0.39; P < .001) but COC (0.12 vs 0.12; P = .101) and SECON (0.14 vs 0.15; P = .869) were not statistically different. VE was higher (3.54 vs 3.49; P < .001) indicating a more disorganized visit pattern and lower continuity of care. Figure 2 shows box plots of the difference in means for UPC, COC, SECON, and VE for patients readmitted versus those not readmitted. Histograms of each continuity measure are also shown below each box plot, highlighting the non-normal distribution of UPC, COC, and SECON.
Descriptive Statistics of Independent Variables for the Cohort by Group
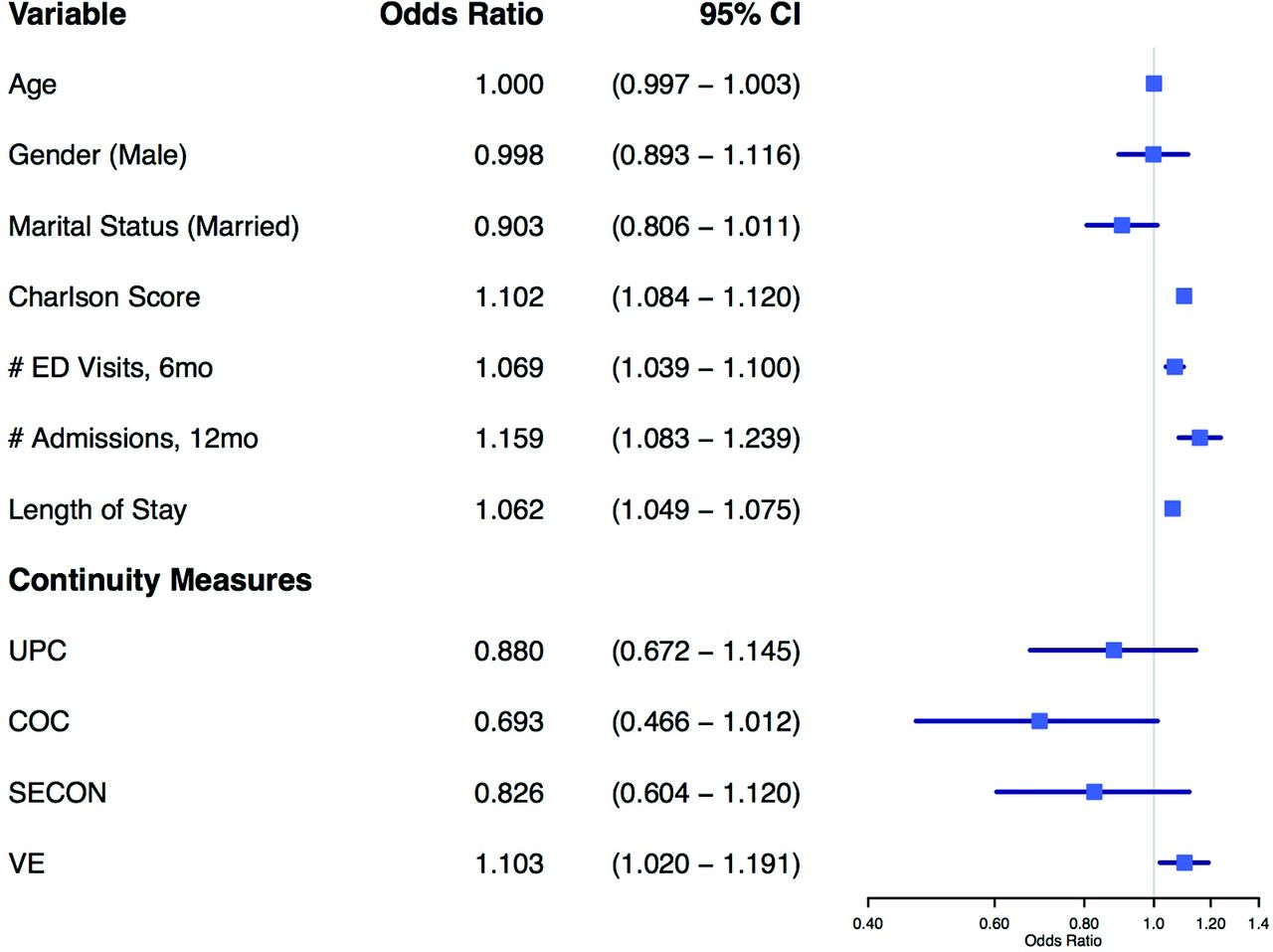
The 4 multivariate models demonstrate that once known readmission risk factors were controlled, continuity of care as measured by UPC, COC, and SECON was not significantly associated with readmission. However, VE remained a significant factor with an odds ratio of 1.10 (95% confidence interval, 1.02 to 1.19). Figure 1 shows the pooled odds ratios for each independent variable in the 4 models along with 95% confidence intervals. The forest plot also graphically shows the odds ratio 95% confidence intervals for UPC, COC, and SECON include 1.0, while VE does not.
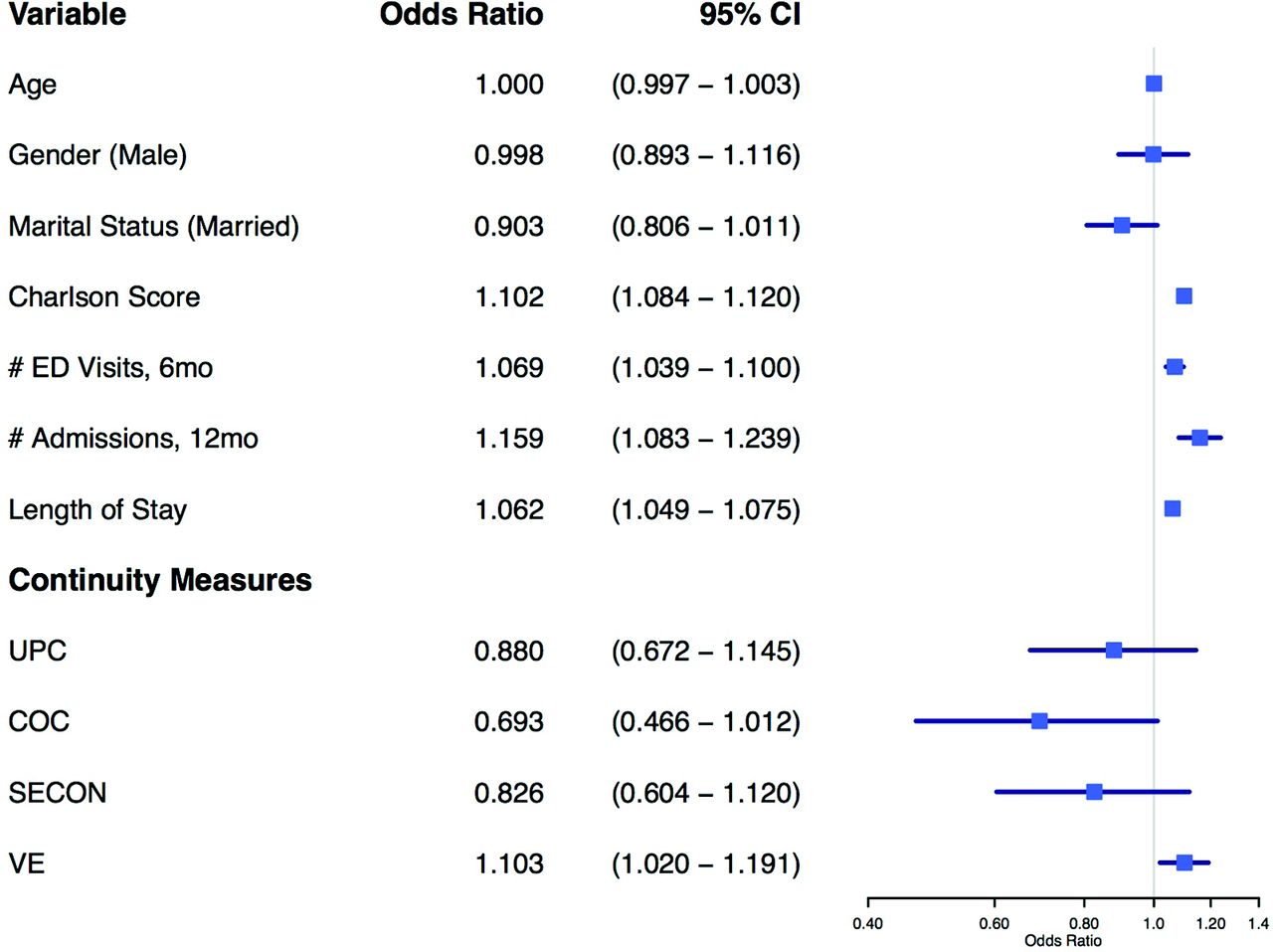
Multivariate odds ratio forest plot for independent variables and continuity measures associated with 30-day readmission. CI, confidence interval; ED, emergency department; UPC, usual provider continuity; COC, dispersion continuity of care; SECON, sequence continuity; VE, visit entropy.
Discussion
Patients with higher VE in the 12 months before hospital admission were more likely to be readmitted or die within 30 days of hospital discharge. This effect was independent of medical comorbidities or utilization factors as measured by the Charlson Comorbidity Index, the number of prior ED visits, and the number of prior hospitalizations in the multivariate analysis. Higher VE reflects a more disorganized visit pattern and a lack of continuity of care. Thus, decreased continuity of care before admission is associated with increased odds of readmission in our study. A single unit change in VE, equivalent to visiting a single physician 4 times (VE = 1.31; Table 2, Case H) versus visiting 4 different physicians once each (VE = 2.37; Table 2, Case C), produces approximately the same change in odds of readmission as an additional Charlson Comorbidity Index point. In other words, reduced continuity is as important a factor in hospital readmissions as the history of myocardial infarction, congestive heart failure, chronic obstructive pulmonary disease, or diabetes without end-organ damage.
Team-based models of care increase collaboration between primary care physicians, subspecialists, midlevel providers, care managers, nurses, dietitians, pharmacists, physical therapists, social workers, and psychologists. This comprehensive patient management by a limited set of health care providers who are familiar with the patient's “story” forms the foundation of a PCMH and may increase quality of care.11 A high-functioning care team helps to support a patient's transition of care from hospital to home, something that is essential in reducing readmissions.44 VE essentially measures the organization of care. Thus, it might prove useful in defining patients at risk for readmission due to a lack of organized care. Of course, further prospective studies are necessary to determine whether actively improving a patient's VE reduces readmission rates.
In the multivariate model, the other measures of continuity (UPC, COC, and SECON) did not show this same association. We believe that this is due to technical limitations of these measures. As shown in Figure 2, the distributions of these measures are highly skewed whereas VE has an approximately normal distribution. Having zero or 1 outpatient visit, which occurs in upwards of 50% of all primary care patients over a 1-year period,45 results in division by zero as demonstrated by the formulas in Table 1 for UPC, COC, and SECON. Division by zero is mathematically undefined, thus excluding significant numbers of patients using these measures (473, 1242, and 1242 respectively).27,46 In contrast, VE is defined even if the patient makes no outpatient visits during the study period. Furthermore, VE can distinguish planned care referrals to a limited set of subspecialists (Table 2, case F) from an equivalent number of unplanned visits to random providers (Table 2, cases C and D), thus detecting organization of care typically seen in PCMHs.27

Prior 12-month continuity measures versus 30-day readmission.
The multivariate analysis confirms many previous studies showing age, comorbidities, length of stay, and number of previous hospitalizations or ED visits are associated with increased odds of readmission.35⇓⇓⇓⇓⇓⇓⇓–43 Marital status, which may be a marker of social determinants of health, and gender have had variable associations with readmission.41,42,47 In this study, neither gender nor marital status was associated with readmission odds.
Limitations
Our study was conducted at a single academic medical institution with 5 primary care clinical sites that are PCMHs. Individual variation between patient's visit patterns within our PCMH produced the differences we observed. We did not compare a PCMH to usual care, nor did we prospectively seek to improve visit organization and continuity within the PCMH. Further study is necessary to determine whether these findings are generalizable to other primary care practices, especially community-based practices. We did not examine cost data; thus, further work is indicated to determine whether organized care that reduces remissions is less costly.
In addition, we were unable to quantify visits to out-of-network clinics and hospitals. Out-of-network outpatient visits decrease continuity. Based on the practice experience of the investigators, the out-of-network visits among our patients are mostly ED visits, a factor known to be a significant predictor of readmission.41 Our inability to quantify out-of-network outpatient visits tends to elevate measured continuity in a group more likely to be readmitted, thus perhaps understating the relationship between lack of continuity and readmission that we observed. Furthermore, many of our patients have insurance plans that actively discourage use of out-of-network providers and thus out-of-network hospitalizations are rare.
The exclusion of frail high-readmission-risk elders enrolled in a care transitions program may attenuate the observed relationship between age, Charlson score, acute medical service utilization, and the odds of readmission. This patient group's VE would be low due to the highly integrated nature of this program. Regardless, any impact on our results should be minimal given the small number of patients involved. Finally, the inclusion of planned readmissions in the analysis may attenuate the relationship between VE and odds of readmission since those with planned readmissions likely have more organized care and thus a lower VE.
Conclusion
Lower continuity of care, characterized by more disorganized visit pattern and thus higher VE, is associated with increased odds of readmission as seen in Figure 1. An association between traditional measures of continuity (UPC, COC, and SECON) and readmission was not found, perhaps because these traditional measures suffer from skewed distributions, undefined division by zero, and the inability to distinguish planned team-based care from random visits. Organized medical care, a key principle of the chronic disease model and PCMHs, is associated with lower odds of readmission among hospitalized primary care patients.
Acknowledgments
We thank Julie Maxson for her invaluable assistance in collecting the data that made this study possible. Funding for this study was provided by Mayo CCaTS Grant UL1TR000135.
Notes
This article was externally peer reviewed.
Funding: Department of Family Medicine, Mayo Clinic, Rochester, MN, Small Grant Funding, Mayo CCaTS grant UL1TR000135.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/1/63.full.
- Received for publication June 7, 2016.
- Revision received September 28, 2016.
- Accepted for publication October 3, 2016.




{kind=link}
{kind=link}