
Abstract
Background: The purpose of this study was to elucidate the effects of injection at trigger points on pain and sleep disturbance in patients with nocturnal calf cramps (NCCs).
Methods: Patients with NCCs that occurred at least once per week and who had myofascial trigger points (MTrPs) on the gastrocnemius muscles were enrolled in the study for 9 months. At the first visit (T0), we measured the intensity of NCC pain on an 11-point numeric rating scale, recorded the frequency of NCCs, and calculated the Insomnia Severity Index (ISI). We then checked for MTrPs on the gastrocnemius muscles and injected 1–2 mL of 0.25% lidocaine into each of the trigger points. At 1 (T1), 2 (T2), and 4 (T3) weeks after the first visit, we repeated the process performed at T0.
Results: Twelve patients completed the treatment schedule and attended the follow-up visits. Mean values of the numeric rating scale pain score, frequency of cramps, and ISI declined significantly at T1, T2, and T3 compared with baseline (all P < .01). Of 12 patients, 10 had clinical insomnia before treatment, and this number decreased significantly to 3 patients at T2 and 1 patient at T3 (P = .012 and P = .001, respectively).
Conclusions: These preliminary data show that injection at MTrPs in patients with NCCs not only alleviated pain and reduced the frequency of cramps but also lessened the severity of insomnia as measured by the ISI. A larger randomized controlled trial is needed to confirm these findings and determine whether the effect lasts over the long term.
Nocturnal leg cramps are sudden, involuntary, painful contractions of the lower extremity in the nighttime, most often in the calf muscles, that gradually lessens. During a calf cramp, the affected muscles become firm and the foot and toes are held in plantarflexion.1,2 While cramps last from a few seconds to several minutes, pain and tenderness may remain for hours after the cramp itself ends.3 One third of adults experience nighttime calf muscle cramping, the prevalence increases as one ages, and 38% to 50% of elderly people suffer from night cramps.4,5 Athletes and pregnant women are also prone to cramps.6,7 Nocturnal leg cramps reportedly occur frequently in the calf muscles.8 In most subjects (73%) the cramps occur only at night; 20% of patients report cramps during the day and night, and 7% have only daytime cramps.9 The etiology of nocturnal leg cramps is unclear, but diseases, including neuromuscular disease, diabetes mellitus, hypocalcemia, and peripheral vascular disease, and medications, such as oral contraceptives, diuretics, and steroids, are reported to predispose people to nocturnal leg cramps.1,3
Cramps are generally a benign and transient problem. Therefore patients do not usually feel anxious when nocturnal leg cramps occur with low frequency and as a sporadic condition. Frequent nocturnal leg cramps can, however, cause pain and significant distress.1,4 Although nonpharmacologic treatments, including stretching and massage,10 and pharmacologic treatments, including quinine sulfate,11 magnesium,12 and gabapentin,13 have been suggested for the management of nocturnal leg cramps, no treatment has yet demonstrated adequate efficacy and safety.1,8
Nocturnal leg cramps are a common problem that may adversely affect sleep.1 One study reported that patients with nocturnal calf cramps (NCCs) experienced sleep disturbance as well as pain and that NCCs disrupted the quality of sleep.2 However, studies considering sleep disturbance from the aspect of treatment efficacy are difficult to find. Prateepavanich et al14 revealed that trigger point (TrP) injection into the gastrocnemius muscles was effective for NCCs in the aspects of pain intensity, frequency, and duration of cramps, but they did not look into the efficacy with regard to sleep disturbance. The purpose of this study was to elucidate the effects of TrP injection into the gastrocnemius muscles on pain and sleep disturbance in patients with NCCs.
Methods
After acquiring approval from the institutional review board of Severance Hospital, Yonsei University Health System (ref. 4-2012-0197), we registered this study at www.clinicaltrials.gov (identifier NCT01804556). Participants were enrolled in this study from our outpatient department for pain management between April and December 2013. Before enrollment, written informed consent was obtained from all participants. We studied male and female patients, aged 20 to 80 years, who visited our outpatient department for pain management of NCCs at least once per week. In this study a muscle cramp was required to occur exclusively at night while at rest and not be preceded by physical exercise. Patients with myofascial TrPs (MTrPs) on the gastrocnemius muscles were included in this study. According to criteria determined by Simons and Travell,15 a diagnosis of MTrPs of the gastrocnemius muscle requires the following: (1) a well-defined, tender, hypersensitive, palpable nodule located within a taut band of the upper gastrocnemius muscle; (2) a typical referred pain pattern; and (3) a local twitch response elicited by snapping palpation of the MTrP. To identify the nodule located within a taut band, the patient lies in a prone position and the clinician uses flat palpation—examination using finger pressure, proceeding across the muscle fibers at a right angle to their length while compressing them against a firm underlying structure, such as bone. A local twitch response is a transient contraction of essentially those muscle fibers in the tense band that are associated with MTrPs. The response is elicited by a sudden change of pressure in the MTrP, usually produced by transverse snapping palpation of the MTrP across the direction of the muscle fibers (taut band), like plucking violin strings. For all patients, a skilled clinician with 4 years' experience in diagnosing MTrPs performed the physical examinations (Figure 1A and B). Patients were excluded if they suffered from electrolyte disorders or congenital musculoskeletal disease or had taken sleeping pills or a sedative in the preceding 4 weeks. Patients also were excluded if they refused to be recruited, had other pain or disease requiring treatment on a preferential basis, were unable to communicate, or had cognitive impairment. Before the examination, we recorded patients' history of spine surgery and whether they were taking medications that can affect the occurrence of cramps, such as diuretics, statins, calcium channel blockers, and anticonvulsants. The patients were requested not to change their medication during the study period.
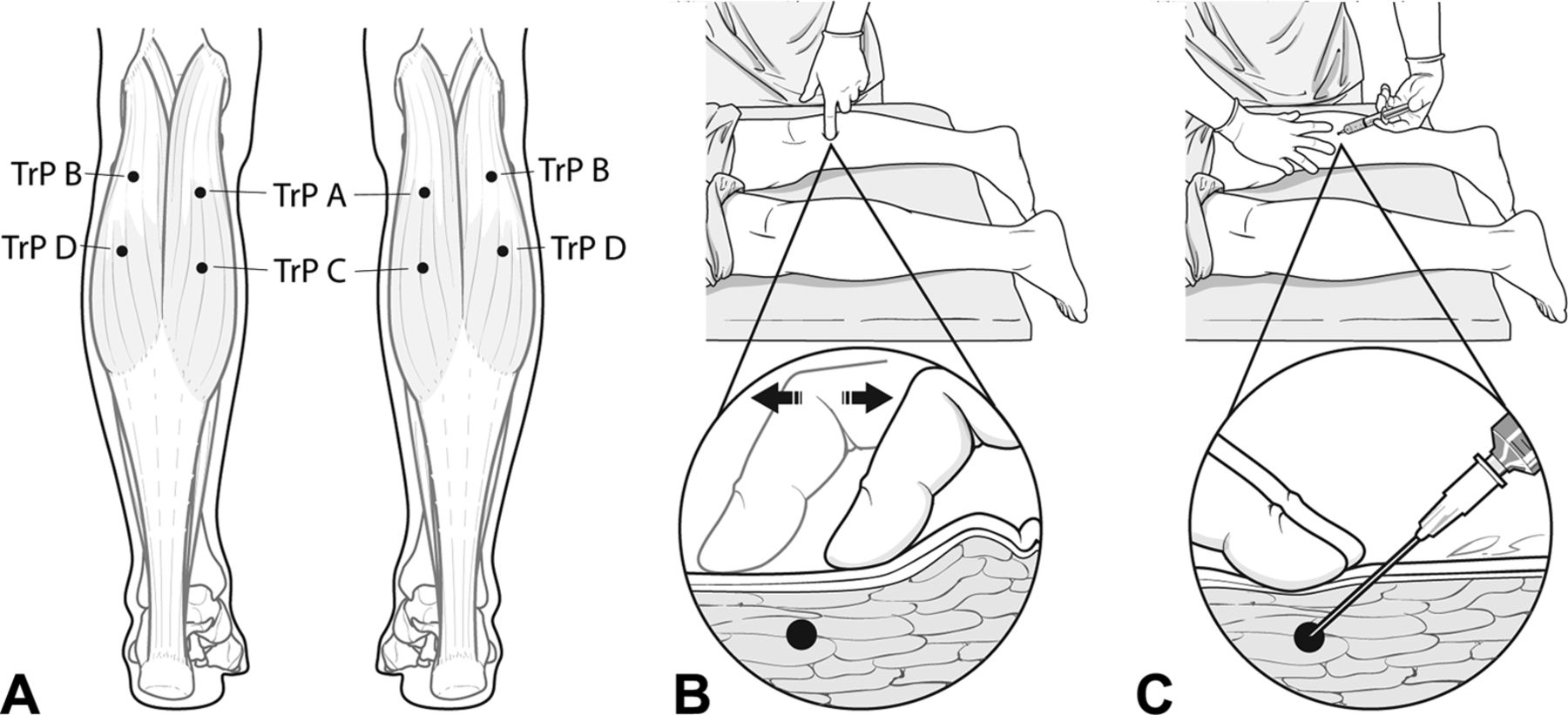
A: Locations of myofascial trigger points (TrPs) in the gastrocnemius muscle, where we identified myofascial TrPs in patients with nocturnal calf cramps in this study. B: Flat palpation, which compresses the muscle against the underlying bone to identify taut bands that harbor myofascial TrPs. C: Injection technique. The TrP is positioned between 2 fingers to prevent the TrP from sliding during injection. The fingers are pressed downward and apart to maintain pressure and ensure hemostasis. A 25-gauge, 1.5-inch needle is inserted between the fingers that have located the TrP. The needle penetrates the skin 1 to 2 cm away from the TrP so that the needle can approach it at an acute angle (30°) to the skin. The syringe, filled with 0.25% lidocaine, may be held between fingers of the injecting hand and thumb pressure used against the plunger. Ensure that the needle tip is positioned on the TrP, and then inject 1–2 mL of lidocaine.
At the first visit (T0), we measured the pain intensity of NCCs using an 11-point numeric rating scale (NRS; 0 = no pain, 10 = the worst pain), recorded the frequency of NCCs (FC), and surveyed patients using the Insomnia Severity Index (ISI). The ISI is a brief self-report questionnaire assessing the nature, severity, and impact of insomnia.16 A higher score on the ISI indicates greater insomnia severity,17 and clinical insomnia is determined by a cutoff score of 15 on the ISI.18,19 This study recorded whether subjects had clinical insomnia, along with the ISI score. We then checked for MTrPs on the gastrocnemius muscles and injected 1 to 2 mL of 0.25% lidocaine into each of the TrPs14,20 (Figure 1C). One week later (T1), if the patients came to the hospital, we again recorded the NRS pain score, FC, and the ISI score; rechecked MTrPs; and repeated TrP injection only in cases in which MTrPs existed. If the patients did not come in, we surveyed the NRS pain score, FC, and the ISI over the phone. Two weeks after the first visit (T2) we repeated the process performed at T0. Four weeks after the first visit (T3) we surveyed the NRS pain score, FC, and the ISI face to face or over the phone.
Statistical Analysis
Sample size calculation was based on NRS pain score as the primary outcome. Previous study has demonstrated that the standard deviation (SD) of the NRS pain score is 2.4.14 Assuming a 5% 2-tailed significance level (α = 0.05) and power of 80% (β = 0.20), a sample size of 11 patients was required to detect a mean difference of 2 in NRS pain score.21 To allow for possible dropouts, 13 patients were recruited at the beginning of the study. Continuous data are presented as mean ± SD or median (range). The normality of the data distribution was assessed using the Kolmogorov-Smirnov test. Categorical data are reported as both frequency and percentage. For normally distributed data, comparisons of the variables with the baseline values at each time point were analyzed using repeated measures analysis of variance; for non-normally distributed data, the Friedman test and Wilcoxon signed rank test were used for analysis. Prevalence changes of clinical insomnia were assessed by the Fisher exact test. The statistical analysis was conducted using SPSS software version 18.0 for Windows (SPSS Inc., Chicago, IL). A P value <.05 was considered statistically significant.
Results
A total of 13 patients met the inclusion criteria, 12 of whom completed the treatment schedule and attended a follow-up. Patient characteristics, calf cramps profile at baseline, and clinical presentations during the study period are described in Table 1. The average age of the patients was 63.1 ± 10.2 years, and the average symptom duration was 36.0 ± 13.5 months. During the research period, none of the patients visited a hospital at T1, and only the patient interviews were assigned at T3 according to our study protocol. Therefore no MTrP injection was performed at T1 or T3. Five subjects had MTrP injection only once at T0 because they reported sufficient improvement of symptoms and they did not want additional treatment at T2. Five patients (2, 4, 8, 9, and 11) reported that they were afraid to tense up their legs for fear of calf cramps.
Mean values of NRS pain score, FC, and the ISI score declined significantly at T1, T2, and T3 compared with baseline (all P < .01; Table 2). However, no significant differences were found between T1 and T2, T1 and T3, and T2 and T3. Using an ISI score of 15 as a cutoff value for clinical insomnia, 10 of 12 patients had insomnia before treatment, and this number decreased significantly to 3 patients at T2 and 1 patient at T3 (P = .012 and P = .001, respectively; Figure 2). There was a significant correlation between the difference in number of MTrPs at T0 to T2 and the difference in NRS pain score at T0 to T3 (Spearman ρ = 0.795; P = .002). During the study period, no subjects experienced complications or serious adverse events associated with the procedure.

Prevalence of clinical insomnia determined by a cutoff score of 15 on the Insomnia Severity Index (ISI) at each time point during treatment with myofascial trigger point injection(s) for patients with nocturnal calf cramps. T0, baseline; T1, 1 week after the first injection; T2, 2 weeks after the first injection; T3, 4 weeks after the first injection. *P < .05 vs T0.
Discussion
In this study we found that MTrP injection into the gastrocnemius muscle can reduce the severity of insomnia, as well as the FC and degree of pain among patients with NCCs. This finding suggests that sleep disturbance should also be considered in the treatment of NCCs.
A previous study showed that local anesthetic injection into the MTrPs of the gastrocnemius muscle in patients with NCCs is as effective as oral quinine, which used to be generally used for the prevention and treatment of nocturnal leg cramps.14 Whether MTrPs can be the source of NCCs, however, is not yet clear. According to evidence of the suggested pathophysiology of muscle cramps, cramps arise from spontaneous discharges of the motor nerves rather than from within the muscle itself.22 Other causes may include abnormal excitability of the terminal branches of motor axons23 and hyperactivity of the motor unit caused by disinhibition at the level of the spine.22 Roeleveld et al,24 however, showed that the temporal and spatial surface electromyographic characteristics of muscle cramps indicate that the cramp is initiated close to or even at the muscle fiber level. Ge et al25 concluded that increased nociceptive sensitivity at MTrPs may underlie the association between MTrPs and muscle cramps, and the motor endplate region and latent MTrPs thereabouts are potential candidates for the origin of muscle cramps based on the results of an experiment in which nociceptive input at latent MTrPs induced muscle cramps. Ge et al reported that treatment of MTrPs could provide therapeutic relief for muscle cramps. In the present study MTrP injection into the gastrocnemius muscle was effective in relieving the pain of NCCs, corresponding with the results of a study by Prateepavanich et al.14
Insomnia is a clinical condition characterized by difficulty initiating or maintaining sleep, accompanied by symptoms such as irritability or fatigue during wakefulness.26 In general, painful conditions and sleep disturbance may influence each other,27,28 and nocturnal episodes of pain in particular are reported to change sleep architecture, induce phases of arousal, and even trigger awakening.29 Hawke et al2 showed that NCCs had a substantial connection with reduced quality of sleep and, by extension, affected health-related quality of life. Blyton et al8 showed that most patients with NCCs were awakened by cramps and remembered cramp outbreaks at irregular times or in the middle of sleep. In addition, NCCs seem to have a negative influence not only on sleep maintenance but also on sleep initiation. According to the aforementioned survey by Blyton et al, the most commonly suggested cause of cramps was sleeping position and movement from this position. Participants who identified the particular movements that induced cramp described plantarflexion of the ankle joint as the trigger.8 In the present study several patients (2, 4, 8, 9, and 11) complained that they adopted an uncomfortable posture to avoid this movement for fear of calf cramps, and this physical strain may interrupt the initiation of sleep. Recent studies suggest that sleep fragmentation may be more critical to chronic pain than the quantity of sleep.29,30 Considering that night cramps occur at one or multiple points during the night, they may be a predisposing factor for sleep fragmentation, and this may cause a vicious cycle of night cramps and sleep disturbance. MTrP injection in patients with NCCs may therefore play a role not only in treating myofascial pain syndrome but also in stopping this vicious cycle.
The ISI has greater benefits than other available measures of clinical insomnia. Its specificity and its relative simplicity to administer and to score make it a popular insomnia screening tool in busy clinical settings.17,19 Although it is not used to definitively diagnose insomnia, the ISI was designed and validated with reference to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria for insomnia,16 and the recommended cutoff indicates whether a sleep disorder justifies clinical attention.18 In addition, the ISI is sensitive to improvement in sleep over the course of both pharmacological and nonpharmacological treatments for insomnia.31 In this study, after MTrP injection, the mean values of the ISI decreased and the number of patients whose ISI score was >15 declined. Therefore we can conclude that MTrP injection into the gastrocnemius muscle for the treatment of NCCs can also be helpful in improving sleep disturbance. In addition, it indicates that in the case of treatment for pain accompanied by sleep disturbance, an accurate measurement of sleep disturbance is needed, not just a check of whether the patient is experiencing sleep disturbance.
This study has some limitations. First, a limited number of patients were available to be recruited for this study. The effects of MTrP injection in patients with NCCs were so distinct, however, that pain and sleep disturbance before and after treatment were significantly different despite the small number of subjects. Second, because of a lack of a control group in this study, the outcomes could not be considered definite findings. Further studies comparing the effect of MTrP injection and physical therapy with a drug such as gabapentin are needed. In addition, more study to verify the treatment effects of MTrP injection in patients with lumbar spinal canal stenosis, which is reported to include a high prevalence of nocturnal leg cramps, will be valuable.5 Third, we did not consider other factors that may have an effect on pain and sleep disturbance in patients with NCCs. Because the present research was a simple observational study on a small scale, it was difficult to handle many variables. Furthermore, even though no patients in this study had secondary causes of cramps, such as hypovitaminosis D, statin therapy, and cirrhosis, it is possible that local TrP injection produces a limited effect if the patients have such diseases or are taking medication.32 Therefore larger and controlled studies are needed.
Conclusion
MTrP injection into the gastrocnemius muscle in patients with NCCs not only alleviates pain and reduces the FC but also lessens the severity of insomnia as measured by the ISI. Considering the pilot nature of this study, however, its results could not be considered definite findings, and a larger study with a control group and a longer follow-up period is needed. As the clinical features of night cramps cause instantaneous severe pain and long-lasting soreness during sleep, rather than a persistent pain, measurement of sleep disturbance needs to be considered once a decision about the treatment effect of night cramps is made.
Acknowledgments
The authors thank Dong-Su Jang, MFA, Medical Illustrator, for his help with the illustrations in this article.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication May 14, 2014.
- Revision received July 29, 2014.
- Accepted for publication August 5, 2014.




{kind=link}
{kind=link}