Abstract
Background: Intrauterine devices (IUDs) are one of the most effective, long-lasting, and convenient contraceptive methods available in the United States. Unfortunately, the anticipated pain and anxiety associated with an IUD insertion procedure deter many people from using this contraceptive method.
Methods: A literature review was conducted on PubMed by searching the terms “IUD insertion”, “pain management”, “anxiety”, “gynecologic procedures”. The Cochrane database was also searched for reviews about pain management methods during IUD insertions. Findings were summarized using the American Academy of Family Physicians’ Strength of Recommendation Taxonomy (SORT) scale.
Results: Pharmacologic methods that can be used to reduce pain with IUD insertion include naproxen, tramadol, lidocaine paracervical blocks, 10% lidocaine spray, lidocaine-prilocaine cream, and EMLA cream. Non-pharmacologic methods for reducing pain or anxiety during gynecologic procedures include pre-insertion counseling, “verbal analgesia”, lavender aromatherapy, distraction with music or television, using Valsalva maneuver instead of tenaculum during IUD insertion, and use of heating pad during procedure.
Conclusion: Moderately effective pharmacologic and non-pharmacologic methods exist for reducing pain and anxiety with IUD insertion. These treatment methods should be offered to create a more comfortable experience for patients. Additional research is needed to determine the comparative efficacy of these methods.
- Anxiety
- Contraceptives
- Evidence-Based Medicine
- Intrauterine Devices
- Pain Management
- Reproductive Health
- Women's Health
Introduction
Half of all pregnancies in the US, about 3 million annually, are unplanned.1 Unplanned pregnancies impose a significant socioeconomic burden on individuals and society. Individuals with unintended pregnancies are more likely to receive late prenatal care and as a result, their infants are at greater risk of being born with a low birth weight, dying in the first year of life, and are at greater risk of not receiving adequate resources for healthy development.2 It is crucial to increase access to effective contraceptive methods, especially now that abortion care has become more restricted with the Dobbs vs Jackson Women’s Health Decision.3
Intrauterine devices (IUDs) are one of the most effective, long-lasting, and convenient contraceptive methods available in the US The failure rates of IUDs and implants are less than 1% per year, significantly lower than other contraceptive options.4,5 IUDs are also very cost-effective, with studies showing that individuals who use an IUD or etonogestrel implant may save thousands of dollars over a 5-year period compared with the use of birth control pills, condoms, patch, or vaginal ring.6
Unfortunately, the anticipated pain and anxiety associated with an IUD insertion procedure deter many people from using this contraceptive method. In one study of nulliparous and parous women who underwent IUD insertion, 17% of nulliparous women reported severe pain with placement of the IUD and 11% of parous women reported severe insertion-related pain.7 Certain past experiences may increase anxiety and pain with IUD insertions as well, such as a history of sexual trauma, previous negative experience with a pelvic examination, or awareness of potential pain learned from a friend or family member.8,9 Transgender patients who struggle with pelvic exams may also have more fear and anxiety with IUD insertions.10 Publications on pain and anxiety related to IUD insertion have mostly been systematic reviews that did not offer guidance on how to apply this information to clinical cases. This article will summarize the available research about pharmacologic and nonpharmacologic methods for decreasing pain and anxiety with IUD insertions and explain how to apply this information in clinical medicine.
Methods
A literature review was conducted on PubMed by searching the terms “IUD insertion,” “pain management,” “anxiety,” “gynecologic procedures.” The Cochrane database was also searched for reviews about pain management methods during IUD insertions. Articles that discussed methods for reducing both pain and/or anxiety were reviewed since anxiety levels influence pain scores.9 Because data about nonpharmacologic methods for decreasing pain is more limited than pharmacologic means, we expanded our search to include nonpharmacologic methods for reducing pain in gynecologic procedures in general, not just with IUD insertions. Tables 1 and 2 were created using the American Academy of Family Physicians’ Strength of Recommendation Taxonomy (SORT) scale.11
Results
Pharmacologic Methods for Reducing Pain and Anxiety with IUD Insertion
Multiple systematic reviews have shown that both naproxen and tramadol decrease pain with IUD insertion, with tramadol having a greater effect on pain reduction.12,13–14 Naproxen can also decrease pain after IUD insertion, with one study showing that pain scores were lower 5 and 15 minutes after IUD insertion among patients who took naproxen, compared with placebo.15 Pain scores were also lower with tenaculum placement, during uterine sounding, and with IUD insertion among patients treated with lidocaine and prilocaine cream, eutectic mixture of local anesthetics (EMLA) cream, or 10% lidocaine spray before the start of the procedure.12,16⇓⇓–19 Patients who received a paracervical block during the procedure also reported decreased pain with tenaculum placement, uterine sounding, and IUD insertion compared with placebo and pain scores were also lower 5 minutes after IUD insertion.8,12,20–21 These recommendations are summarized in Table 1.
Effective Pharmacologic Methods for Reducing Pain with IUD Insertion
Generally, lidocaine gel has not been showed to be effective for reducing pain with IUD insertion.12,22 One study found that self-administered 2% vaginal lidocaine gel before IUD insertion helped to reduce pain with tenaculum placement but had no effect on pain level with IUD insertion.23 A novel 4% lidocaine formulation was shown to be effective for reducing pain with IUD insertion in a phase 2 clinical trial, but further studies of this lidocaine formulation are needed before its use can be medically recommended.24
Cervical ripening methods are also not effective at reducing pain with IUD insertion. There is a strong recommendation to avoid misoprostol because it is associated with cramping and higher pain scores during IUD insertion.12,25 A recent meta-analysis of vaginal dinoprostone use vs placebo with IUD insertion showed statistically significant reduction in pain scores with tenaculum placement, sounding of uterus, and IUD insertion but these results were not clinically meaningful.26
Nonpharmacologic Methods for Reducing Pain and Anxiety with Gynecologic Procedures
The data about nonpharmacologic methods for decreasing pain with IUD insertions and other gynecologic procedures is limited.
A preprocedure counseling appointment is recommended. During this visit, the clinician should review what to expect during the IUD insertion procedure and discuss measures that can be taken to minimize discomfort. This visit is also an opportunity to provide reassurance and build a trusting relationship with the patient. These measures will help to alleviate a patient’s anxiety and may decrease patient’s pain during the procedure.7,27–28
Creating a calm, relaxing environment for the patient during the procedure can help to minimize discomfort during the IUD insertion as well. For instance, lavender aromatherapy has been shown to reduce anxiety during IUD insertions as well as during intrauterine insemination procedures.29–30 Music has been shown to reduce anxiety and perception of pain during hysteroscopy and colposcopy.28,31⇓–33 Watching television during reproductive health care procedures, including IUD insertions, has a been effective at reducing anxiety.34 Holding a warm compress to the lower abdomen during a procedure can also serve as a distraction and minimize discomfort.7
Since higher levels of anxiety contribute to higher levels of pain during gynecologic procedures, it is important to take steps to minimize patient’s anxiety.9,12 “Verbal analgesia” is effective at reducing pain and anxiety during gynecologic procedures.7,35⇓–37 Verbal analgesia is a technique in which the clinician calms and relaxes the patient by providing reassurance throughout the procedure multiple times using a low voice volume and slow rate of speech.35 With this “verbal local” approach the clinician maintains continuous communication with the patient and explains each step of the procedure in a soothing, calming tone. One study that analyzed use of verbal analgesia during IUD insertion showed that verbal analgesia has the same analgesic effect as 50 mg of oral tramadol.35
Valsalva maneuver can be used instead of a tenaculum during IUD insertion to reduce pain and anxiety. One study compared the efficacy of IUD insertion with Valsalva maneuver versus tenaculum use and found that both methods were equally successful. In addition, the Valsalva maneuver was associated with less anxiety, less pain, and less bleeding with IUD insertion.38 This study determined that immobilization of the cervix was the most important factor for passing an IUD through the cervical canal, and this could be achieved with Valsalva, which immobilizes the cervix and uterus by increasing intra-abdominal pressure. There were no cases of uterine perforation with use of Valsalva during IUD insertion. Another study compared the use of Valsalva vs tenaculum to pass a Pipelle device into the uterus for an endometrial biopsy; both methods were equally successful.39 These recommendations are summarized in Table 2.
Nonpharmacologic Methods for Reducing Pain or Anxiety with Gynecologic Procedures
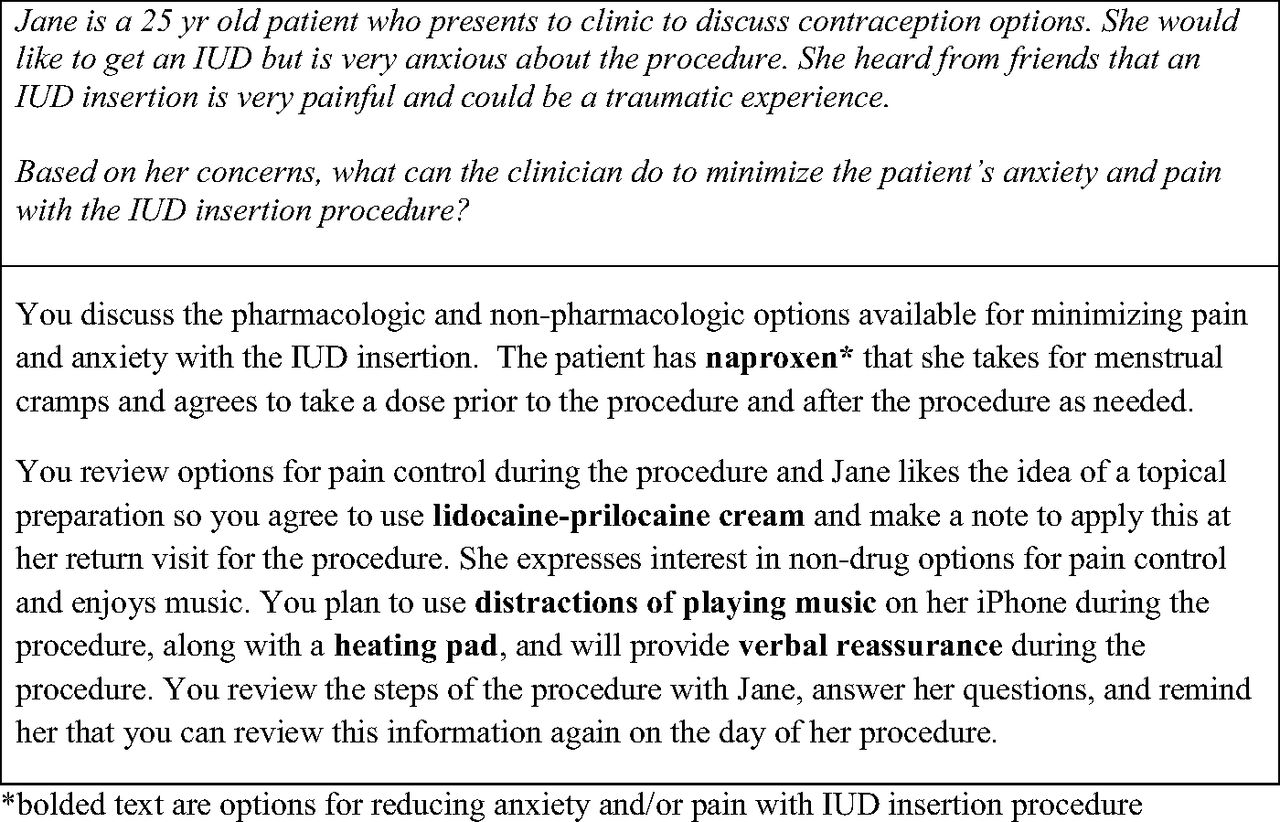
Evidence-based recommendations for choosing one pain-relieving measure over another do not exist. Shared decision making with the patient is an important alternative to help patients understand options and trade-offs for the different pain relief methods that the clinician has available in their setting. For instance, it is important for patients to know that lidocaine paracervical blocks can reduce pain with tenaculum placement and IUD insertion but may cause pain when injected into the cervix.20 It is also helpful to offer more pain relief options to patients who are at higher risk for experiencing discomfort with IUD insertion, such as patients who are nulliparous, have a history of cervical stenosis, dysmenorrhea, or have significant preprocedure anxiety.7,9,40 Please refer to Figure 1 for a case study that shows how to use pharmacologic and nonpharmacologic methods to reduce pain and anxiety with IUD insertion.

{kind=link}
Case study.
Conclusion
Moderately effective pharmacologic and nonpharmacologic methods exist for reducing pain and anxiety with IUD insertion. These treatment methods should be offered to create a more comfortable experience for patients. Additional research is needed to determine the comparative efficacy of these methods.
Acknowledgments
Mindy Smith, MD, MS provided editing assistance.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/37/6/1150.full.
- Received for publication February 21, 2024.
- Revision received May 17, 2024.
- Accepted for publication May 28, 2024.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.