Abstract
Background: Discharge communication between hospitalists and primary care clinicians is essential to improve care coordination, minimize adverse events, and decrease unplanned health services use. Health-related social needs are key drivers of health, and hospitalists and primary care clinicians value communicating social needs at discharge.
Objective: To 1) characterize the current state of discharge communications between an academic medical center hospital and primary care clinicians at associated clinics; 2) seek feedback about the potential usefulness of discharge readiness information to primary care clinicians.
Design: Exploratory, convergent mixed methods.
Participants: Primary care clinicians from Family Medicine and General Internal Medicine of an academic medical center in the US Intermountain West.
Approach: Literature-informed REDCap survey. Semistructured interview guide developed with key informants, grounded in current literature. Survey data were descriptively summarized; interview data were deductively and inductively coded, organized by topics.
Results: Two key topics emerged: 1) discharge communication, with interrelated topics of transitional care management and follow-up appointment challenges, and recommendations for improving discharge communication; and 2) usefulness of the discharge readiness information, included interrelated topics related to lack of shared understanding about roles and responsibilities across settings and ethical concerns related to identifying problems that may not have solutions.
Conclusions: While reiterating perennial discharge communication and transitional care management challenges, this study reveals new evidence about how these issues are interrelated with assessing and responding to patients’ lack of readiness for discharge and unmet social needs during care transitions. Primary care clinicians had mixed views on the usefulness of discharge readiness information. We offer recommendations for improving discharge communication and transitional care management (TCM) processes, which may be applicable in other care settings.
- Communication
- Discharge Planning
- Patient Safety
- Primary Health Care
- Transitional Care
Introduction
Communication between hospitalists and primary care (PC) clinicians (including physicians, nurse practitioners, and physician assistants) is essential after hospital discharge to improve care coordination, minimize adverse events, and decrease costs.1 Review of discharge information is a core component of transitional care management (TCM), which is required by the Centers for Medicare and Medicaid to support patients’ transitions from inpatient care back to home.2,3 High quality discharge communication should include complete and timely information about primary diagnosis, diagnostic test results, treatment or hospital course, discharge medications, pending studies, patient and family counseling, and follow-up plans.4 Despite increasing access to inpatient hospital data through shared electronic health records (EHRs), PC clinicians do not always have access to complete and timely hospital discharge summaries.5⇓⇓–8 Further, hospitalists and PC clinicians note the importance of including social information in discharge communication,9 which is now reinforced by recent US federal policy encouraging inpatient screening for health-related social needs.10
In our ongoing research on improving discharge processes, we asked that the Readiness for Hospital Discharge Scale (RHDS)11⇓–13 be completed by discharging patients, inpatient registered nurses (RN), and, when possible, family caregivers on the day of discharge. The RHDS assesses perceptions of discharge readiness across 4 domains: Personal Status (how the patient feels on day of discharge), Knowledge (about self-care at home); Perceived Coping Ability; and Expected Support (how much social or caregiving support the patient will have). The RHDS is a validated measure which has demonstrated a positive predictive value of identifying patients at risk for adverse postdischarge outcomes, such as readmission.11,12 (Appendix 1 has additional details about the RHDS.)
The original purpose of this study was to: 1) characterize the current state of discharge communication between an academic medical center hospital and PC clinicians at associated clinics, and 2) seek feedback about the potential usefulness of discharge readiness information to PC clinicians. Additional aims of this manuscript include describing unexpected inductive, but strongly interrelated, topics that emerged from the data, including PC clinician views on: a) inadequate TCM processes and hospital follow-up appointments, b) concerns about lack of shared understanding between hospital and PC teams and ethical concerns related to lack of available resources, and c) specific recommendations for improving discharge communications.
Methods
Study Design
We used an exploratory, convergent mixed methods design, using an investigator-developed survey and semistructured interviews with the purpose of using interviews to clarify and expand our understanding of survey data. This study was approved by the University of Utah Institutional Review Board (IRB# 00154704). Recruitment and research participation was completed June-July, 2022.
Sample
The study team recruited Family Medicine (FM) and General Internal Medicine (GIM) PC clinicians at an academic medical center of the intermountain United States. The study team invited participation during faculty meetings, then emailed the survey to all faculty in each division (FM n = 36; GIM n = 20; Total = 56). A second invitation was emailed approximately 1 week later. Survey respondents indicated willingness to participate in an interview.
Survey
The 94-item electronic REDCap13,14 survey (Appendix 2) was informed by a literature review.15⇓–17 This manuscript reports survey responses in these domains: individual and practice characteristics (items 3 to 9); discharge communication received directly from a hospital care team member versus communication sent automatically through the EHR (items 18 to 28); and specific feedback on the RHDS (items 62 to 84). To ensure anonymity, participant contact information was unlinked to survey responses.
Interviews
The interview guide was developed with input of key informants from the health system and current literature review.15,17⇓–19 The interview guide domains align closely with survey domains; domains and subdomains with definitions are provided in Appendix 3. The interview guide was iterated based on an ongoing review of survey responses and team debriefing after interviews. Probing questions were used to elicit more information about topics raised by participants not included in the original interview guide, particularly related to feelings about receipt and integration of social information. Interviews were conducted by phone or video conferencing, and were audio recorded, professionally transcribed, verified, and deidentified.
Data Analysis
Descriptive statistics were summarized using Stata/S.E. 17.0.20 Qualitative data from open-ended survey responses and interview transcripts were analyzed using content and thematic analysis.21,22 Initial deductive codes were derived from the original version of the interview guide. The first 2 interviews were coded in Microsoft Word simultaneously by 2 coders (CEE and ME), then discussed with a third (AAB). The remaining interviews were coded individually, then verified by a second coder. Inductive codes were iteratively added and discussed until agreed on. The team reached consensus as codes were grouped into topics using Microsoft Excel. Interview guide domains, subdomains with definitions, and codes are found in Appendix 3.
Data Integration and Rigor
Quantitative and qualitative data were compared and triangulated.23 Peer debriefing was used to explore topics, interpretations, and biases. Member-checking occurred within and between interviews, and by sharing deidentified, preliminary results with FM and GIM divisions. The team agreed there was data saturation,24 meaning no new topics emerged in the final interviews. Taken together, these considerations increase rigor, credibility, and trustworthiness of the data and interpretation.23,25
Results
Twenty-five surveys (44.6% participation rate) were completed. From these, 12 of the 25 respondents completed interviews. 3 surveys were started but not completed and were excluded from the analysis. Surveys took ∼15 minutes; interviews lasted ∼30 minutes.
Sample Characteristics
Participants were mostly physicians (84%), while the remaining were Nurse Practitioners or Physician Assistants. Of survey respondents (n = 25), 40% (n = 10) had been in their role for 1 to 5 years. Interview participants (n = 12) had practiced for a mean of 10 years (standard deviation [S.D.]=9.9; range 3 to 36 years). Interview respondents reported a mean panel size of 1187 patients (S.D. = 832, range 50 to 1700). Specific division information was only collected in interviews, where respondents were divided evenly between FM and GIM (50% each), representing 4 clinics, 2 from each division. Table 1 displays sample characteristics.
Participant Characteristics
Key Topics
Two main topics emerged from quantitative and qualitative data integration representing the key experiences shared by participants and are presented below. Survey responses are summarized in Tables 2 and 3; interview topics and excerpts are found in Table 4.
Primary Care Clinician Survey Responses Related to Current Discharge Communication Received
Survey Respondent Perspectives About Receiving the Readiness for Hospital Discharge Scale (RHDS)
Qualitative Topics and Excerpts from Interviews (n = 12)
Topic 1: Discharge Communication
The first topic includes findings related to a) views of current discharge communication between inpatient and PC settings, b) TCM and follow-up appointment challenges, and c) recommendations for improving discharge communication.
Overall, feelings about hospital discharge communication between inpatient and PC settings were mixed. Few respondents (8%, n = 2) state that they regularly (>50% of the time) receive direct discharge communication (Table 2). 16% (n = 4) reported never having received direct discharge communication. 48% (n = 12) of respondents said direct communication most often comes from the inpatient attending physician versus inpatient Case Manager (16%, n = 4) or other team member. Direct communication is most often received in an EHR in-basket message (per 20 of 21 [95%] of those who report receiving direct communication) versus phone call. Satisfaction with current discharge communication was low to neutral, with 32% (n = 8) dissatisfied/very dissatisfied and 56% (n = 14) responding neutrally (Table 2).
Most (68%, n = 17) survey respondents reported receiving automatic discharge notifications most (75 to 100%) of the time (Table 2). However, 20% (n = 5) reported that notifications are frequently missing. Almost one-third (28%, n = 7) state they commonly (25 to 75% of the time) receive notifications for patients they do not know.
When notified of a hospital discharge, participants said they respond in various ways ranging from deleting the message with no additional action, to contacting the hospital care team and/or patient, and coordinating postdischarge care with the clinic Care Manager. While survey respondents generally felt discharge notifications are Helpful (42%, n = 10) or Very Helpful (25%, n = 6), interviews revealed a range of positive and negative experiences (Table 4). Importantly, there was overwhelming consistency that discharge summaries are not completed/signed in a timely manner, resulting in having to search the EHR. Interviewees also noted variations in communication from hospitals within the region. Interoperability (ie, the Epic-specific ‘Care Everywhere’ function26) of regional hospital EHRs was mentioned positively (Table 4). One specific outside hospital was noted as having clear, brief discharge summaries and clinicians who make direct contact.
An unexpected finding emerged from the interviews centered around current TCM process, including hospital follow-up appointments. PC clinicians knew of an existing process to support transitions from hospital to PC. However, they could not describe what this involved, which patient population(s) it reaches, or which department was “in charge” (Table 4).
In addition, PC clinicians described 2 important challenges related to hospital follow-up appointments (Table 4). First, patients leave the hospital with no follow-up scheduled. Second, clinics lack dedicated TCM appointments reserved for hospital follow-up. PC clinicians also recognize important challenges with some patients who need optimal continuity of care, including those who are frequently hospitalized.
PC clinicians had specific recommendations for improving discharge communications, saying discharge summaries should be timely and brief, and include a) reason for admission; b) implications for outpatient care, particularly rationales for changing medications; and c) an actionable to-do list. Finally, PC clinicians recognized that direct messages from the inpatient team would be ideal, but not always realistic (Table 4).
Topic 2: Usefulness of the RHDS in the Outpatient Setting
The second topic focused on the usefulness of the RHDS in PC settings. Participants highlighted concerns regarding a lack of shared understanding about roles and responsibilities across settings and ethical concerns related to identifying problems that may not have readily available solutions. In surveys, 52% (n = 13) said they wanted to receive the RHDS from at least 1 perspective (that is, patient, inpatient RN, or family caregiver) (Table 3). Almost half said that they would like to receive the patient’s RHDS (46%), and inpatient RN’s RHDS (44%) (Table 3). Of those, most wanted it in the discharge summary (Table 4).
When asked to share thoughts on why they did not want to receive this information (Table 3), respondents were concerned that issues identified by the RHDS should be addressed before the patient is discharged; that the information would not affect their clinical decision making; that they lacked adequate resources to address identified issues; and that they already felt overloaded with “too much information” (Survey Participant [SP] 5).
Still, many PC clinicians saw the value in completing the RHDS before discharge. Moreover, respondents said that if the RHDS score indicated the patient was at “high-risk” for unplanned readmissions, it could trigger specific action (Tables 3 and 4). For example, if the inpatient RN had concerns, the PC clinician would “expedite follow-up and potentially set up services prior to follow-up” (SP 1).
In addition, PC clinicians expressed concerns of a lack of shared understanding about roles and responsibilities across settings, and their sense that they are left to handle social circumstances for which they have no resources (Table 4). PC clinicians also raised ethical concerns stemming from assessing problems that may not have readily available solutions either inside the health care system, or through community resources, particularly if a patient’s lack of discharge readiness is related to unmet social needs (eg, transportation, food, housing). In particular, this lack of resources includes understaffing in key interdisciplinary roles which are essential during transitions of care, including Case Managers, Clinical Pharmacists, and Social Workers. Respondents felt inpatient clinicians “kick the can” without recognizing that PC clinicians have limited resources (eg, revenue, staffing) to handle social circumstances.
Discussion
In seeking to assess the potential usefulness of the RHDS during care transitions, we uncovered both expected and unexpected concerns about the current quality of discharge communication, gaps in the current TCM processes, and ethical concerns related to screening patients for discharge readiness, particularly when a lack of readiness is related to unmet social needs which cannot be addressed by available resources. These results echo previously cited concerns about absent, incomplete, or difficult to read discharge summaries,5⇓–7 lack of standardized processes, inadequate compensation for care coordination, the need for more training around care transitions,27,28 and lack of resources available to meet patients’ social needs.29⇓–31
Half of PC clinicians said they find value in patient discharge readiness assessment information gained from the RHDS. Summarized RHDS information would be welcomed if directed to appropriate members of the PC team, including RN Care Managers, Clinical Pharmacists, and Social Workers. Indeed, other studies have found that TCM that includes Clinical Pharmacists32 and RNs33,34 is highly effective in reducing unplanned health care utilization.
That said, PC clinicians had ethical concerns about using the RHDS in the inpatient setting if a lack of readiness and/or unmet needs are not partially or fully addressed before discharge. Though hospitalists may feel pressure to discharge patients as soon as they are medically stable, PC clinicians expressed strong dislike of feeling like hospitalists are “kicking the can” to them without at least beginning to address patients’ unmet needs.
Still, PC clinicians expressed that if unmet needs information is communicated in a clear and timely manner, the PC team could act by referring patients to resources, or bringing patients in for follow-up sooner, particularly if the RHDS score indicated patients were at risk for readmissions or poor outcomes. Our study suggests that a summary of key RHDS findings should be communicated to outpatient providers, who can continue interventions that are initiated in the hospital, if resources are available. Strengthening federal and state policies to enhance community-level resources may ultimately help assuage clinicians’ ethical concerns about social needs screening in the context of insufficient resources.
In this study, PC clinicians preferred brief, actionable discharge summaries containing the reason for admission, clear rationales for medication changes, and specific implications for outpatient care. Importantly, though inpatient clinicians may be reticent to dictate to another clinician how to practice, PC clinicians in this sample nevertheless expressed the clear desire to know what specific actions the discharge team would recommend for them as the patient’s PC clinician (eg, draw repeat CBC on June 1). While some PC clinicians noted that direct peer-to-peer calls or messages would personalize communications and better catch their attention, which is consistent with findings from other studies,9,15 they also expressed understanding this is not always feasible or realistic for either inpatient or outpatient clinicians. Finally, PC clinicians clearly stated that discharge communications should be timely – completed as soon as possible after discharge— and before the patient is seen in outpatient care.
In this study, participants noted a wide variation in responses to receiving discharge communications. Our sense from the qualitative findings is that this has to do with the fact that discharge summaries are reported to be inconsistent, untimely, long, and do not specify recommended action. This suggests that systems-level improvement in the consistency, timeliness, brevity, and actionable usefulness of discharge summaries may offer a clear pathway forward toward improved transitions. For example, After Visit Summaries meet patients’ communication needs by using clear visual displays, appropriate literacy levels, and by specifying self-management recommendations to the patient.35,36 Our findings suggest that discharge summaries should be designed using similar user-centered methods, including specifying recommended action items for the patient’s continuity clinician. This aligns with Unnewehr et al.’s systematic review on optimizing the quality of discharge summaries: while health systems may customize discharge communications as needed, they should adhere to best practices including using concise language, and a consistently clear structure and layout.28
While the health system in this study has a TCM process, PC clinicians were unclear on its details; this may be a cautionary tale for health systems currently implementing TCM or struggling with TCM quality. This suggests that efforts to implement or reinforce TCM within a health system should engage both the inpatient discharge team and outpatient interdisciplinary team members in all ambulatory settings, particularly within PC. Furthermore, situating TCM processes within PC allows for a fiscal benefit to PC by using billing codes to generate revenue to fund additional interdisciplinary staff dedicated to this critical time for patients.37
A TCM core component is a face-to-face visit with a clinician within 7 to 14 days depending on complexity.2,3 Based on these study data and observations from other unpublished academic health system TCM processes, this health system should consider reserving outpatient hospital follow-up appointments in advance, prioritizing timeliness (ie, within 7 to 14 days), adequate duration (eg, 40 minutes), continuity of care (ie, patients see clinicians they know), regular interprofessional team meetings (ie, to discuss patients at higher risk of readmission or poor outcomes), and open lines of communication across inpatient-outpatient settings. Member checking for this study also revealed that hospital follow-up appointment scheduling should be streamlined to reduce time-burden for inpatient staff, for example, by having a dedicated phone line to reach outpatient scheduling. This would address PC clinicians’ concerns that appointments be made, in consultation with the patient, before the patient goes home.
Limitations
This study had limitations. Survey data are subject to social desirability and recall biases. Sampling from 1 academic health system limits generalizability, as does the low response rate. However, we attempted to mitigate this by using a rigorous mixed methods design, which included triangulation of quantitative survey data with qualitative responses in the surveys and interviews, iterating the interview guide to clarify emergent topics, continuing interviews until data saturation was reached, and member checking preliminary data interpretations with both FM and GIM divisions. Respondents were largely young, White, Non-Hispanic, and had been in their role for <10 years. This study only included PC clinicians, so findings may apply differently in specialty outpatient care settings.
Conclusion
This study reiterates perennial – yet still unsolved – challenges with hospital discharge communication and TCM during patients’ return to PC settings. Our findings also convey new evidence related to how discharge communication and TCM processes are seen as being interrelated with assessing and responding to patients’ lack of readiness for discharge and unmet social needs during care transitions. PC clinicians’ views are mixed about whether the RHDS would be a useful tool for communicating patients’ readiness for discharge. Some suggested that the RHDS would be helpful in identifying deficiencies in social needs and/or support, prompting actionable interventions by the PC team immediately following hospital discharge, while others stressed that interventions should begin while the patient is still in the hospital and be incorporated with clearer, timely, and directive discharge communication. We offer recommendations for improving discharge communication and TCM processes, which may be applicable in other care settings. Finally, PC clinicians raise concerns about how a lack of sufficient resources – both internal hospital system-based and external community-based – limits their individual agency to address patients’ social needs, again reinforcing the importance of buttressing assessment mandates with systemic- and policy-based resources and solutions.
Acknowledgments
We appreciated the opportunity to present and seek feedback on preliminary findings with the study site’s Family Medicine outpatient primary care clinicians, and General Internal Medicine inpatient hospitalists and Advanced Practice Clinicians, and General Internal Medicine outpatient primary care clinicians. Their feedback and perspectives were valuable in shaping our discussion of the study’s findings.
Appendix
Appendix 1. Additional Details About the Readiness for Hospital Discharge Scale
Additional details about the Readiness for Hospital Discharge Scale (RHDS) can be found on the Marquette University webpage.25 Different versions of the RHDS – for patients (e.g., adults, children, and post-partum mothers), caregivers, registered nurses (RN), and physicians – vary primarily in the phrasing of the questions with the central focus remaining always on the patient. For example, the patient version of question 1 reads “How physically ready are you to go home?” whereas the RN version reads “How physically ready is your patient to go home?” Scoring is done by adding item scores and dividing by the number of items, which calculates a mean score on a 0 to 10 scale. Subscale scoring is also possible. The Marquette University webpage includes a database of approved translations of the RHDS in various languages and a bibliography of references related to instrument development. Note that the study authors had permission to use the scale, but are not the original creators of the scale.
Appendix
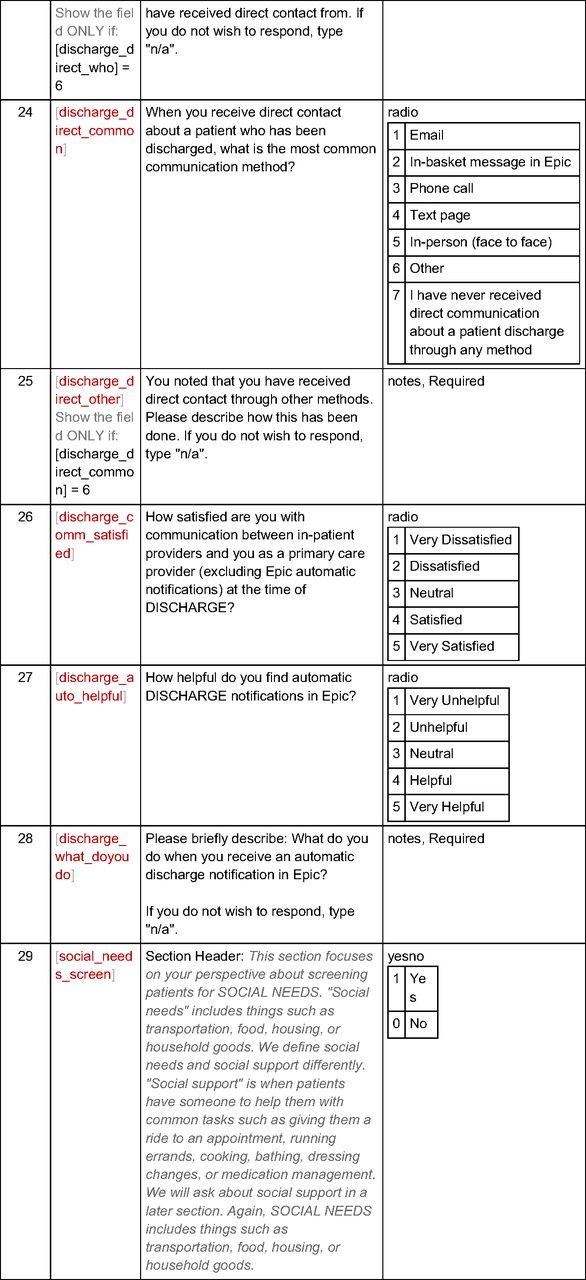
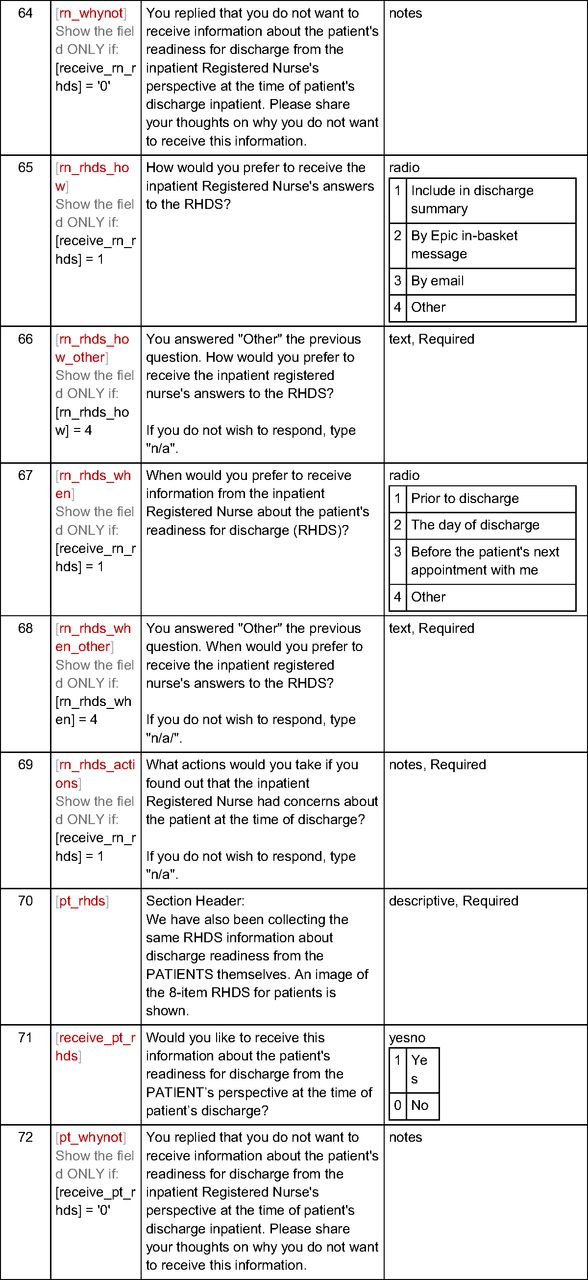
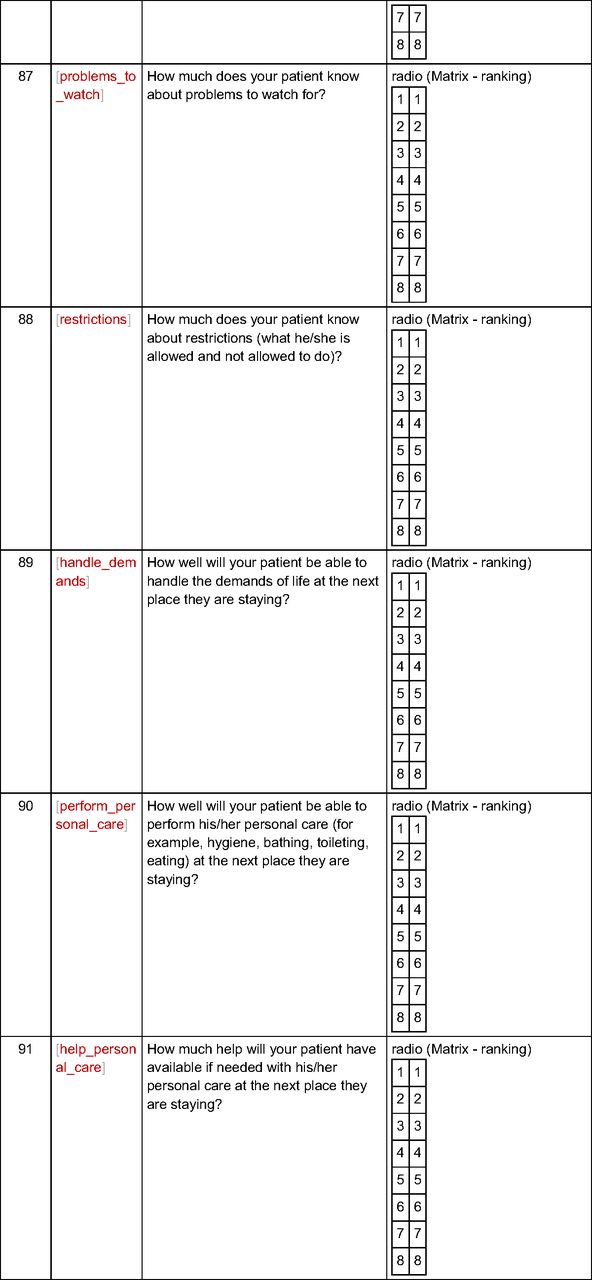
Appendix 2. Ninety-Four-Item Electronic REDCap Survey














Notes.
Items 3, 13-18, 20, 21 and 26 were adapted from Sheu L, Fung K, Mourad M, Ranji S, Wu E. We need to talk: Primary care provider communication at discharge in the era of a shared electronic medical record. J Hosp Med. 2015;10(5):307-310. doi:10.1002/jhm.2336
Items 29-42 inquiring about social needs and the corresponding questions (45-56) related to social support were adapted from Boch S, Keedy H, Chavez L, Dolce M, Chisolm D. An integrative review of social determinants of health screenings used in primary care settings. J Health Care Poor Underserved. 2020;31(2):603-622. doi:10.1353/hpu.2020.0048
Results from items 85-94 were used as preliminary data for a different study.
Appendix
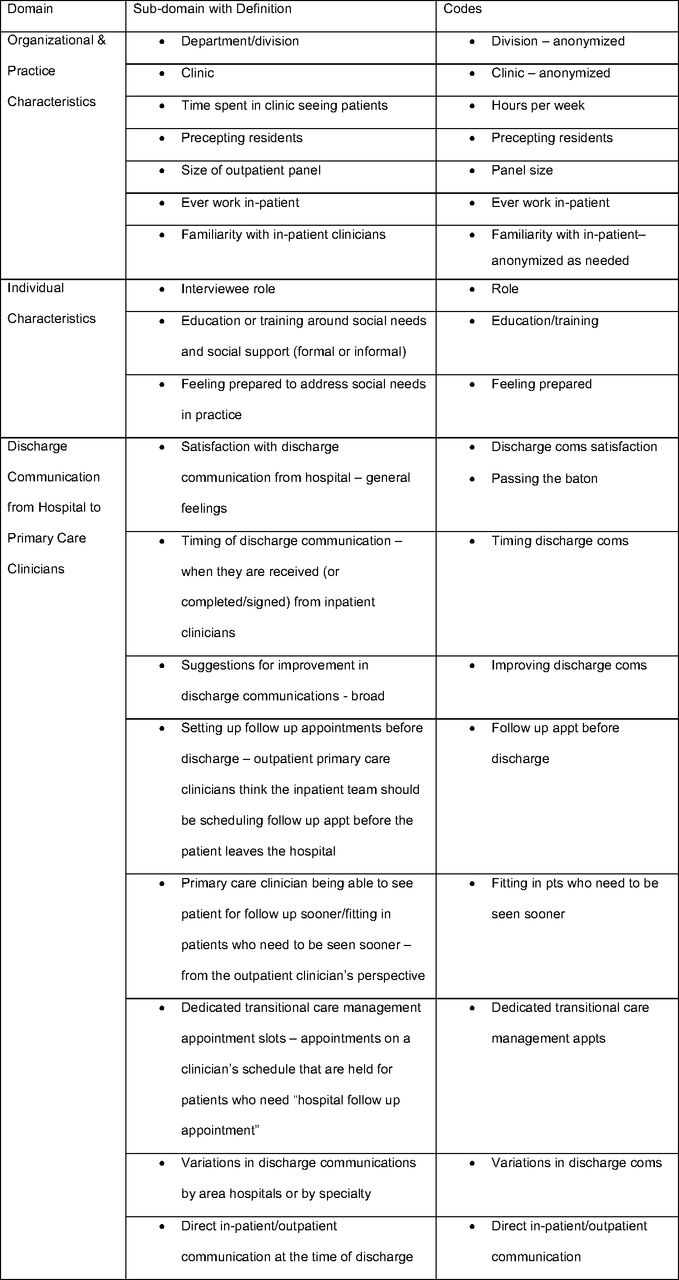
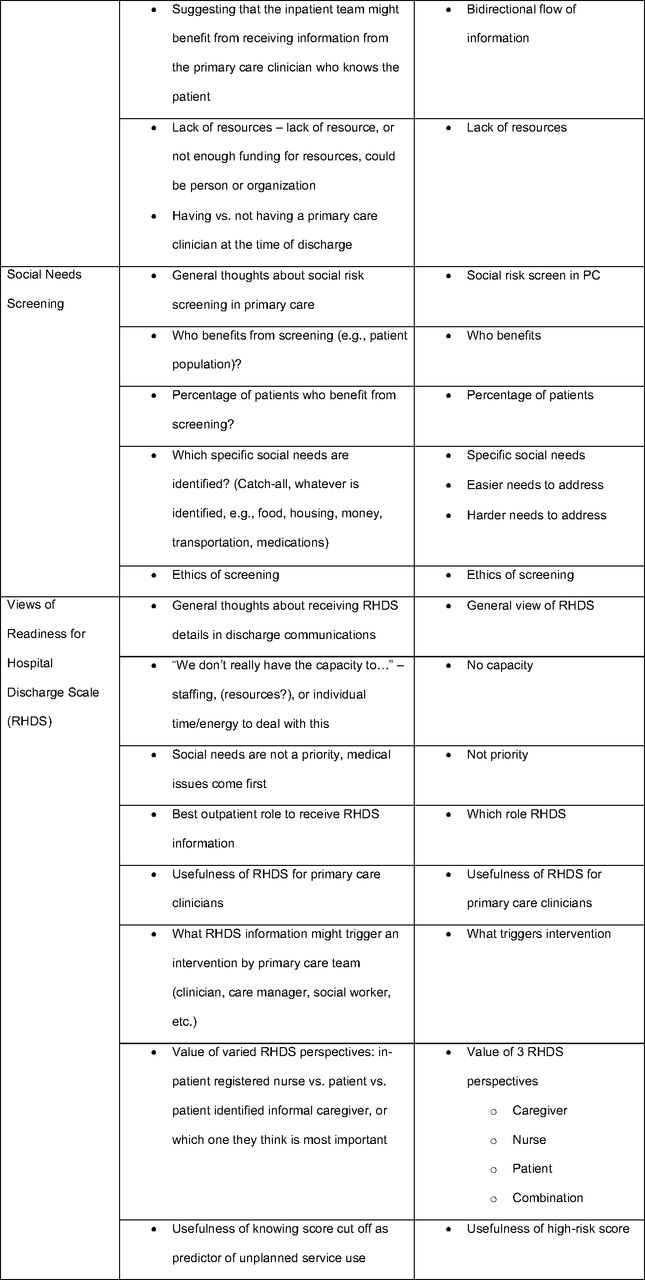
Appendix 3. Interview Guide Domains, Sub-domains with Definitions and Codes: Discharge Communication, Social Needs Screening, and Readiness for Hospital Discharge Scale



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Notes
This article was externally peer reviewed.
Funding: Dr. Elmore was supported by the National Institute of Nursing Research of the National Institutes of Health (NIH) under Award Number T32NR013456. The ongoing research referred to in this paper is The NEEDS Study (PI: Wallace), which is supported by the Agency for Healthcare Research and Quality (AHRQ) under Award Number R01HS026248. The use of REDCap at the University of Utah is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002538 for period 4/1/18-2/28/23. The content is solely the responsibility of the authors and does not necessarily represent the official view of the NIH or AHRQ.
Conflict of interest: Dr. Wallace discloses consulting fees paid by American Association of Medical Colleges, payment/honoraria paid by Northwell Health, and meeting/travel support for NIH and PCORI Study Sections. The other authors have no conflicts of interest to report.
We used the COREQ checklist for reporting the qualitative elements of this mixed methods study.The deidentified data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
To see this article online, please go to: http://jabfm.org/content/37/4/706.full.
- Received for publication May 2, 2023.
- Revision received June 2, 2023.
- Revision received August 28, 2023.
- Revision received January 25, 2024.
- Accepted for publication February 19, 2024.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.