Abstract
Introduction: Symptom diagnoses are diagnoses used in primary care when the relevant diagnostic criteria of a disease are not fulfilled. Although symptom diagnoses often get resolved spontaneously without a clearly defined illness nor treatment, up to 38% of these symptoms persist more than 1 year. It is largely unknown how often symptom diagnoses occur, which symptoms persist, and how general practitioners (GPs) manage them.
Aim: Explore morbidity rates, characteristics and management of patients with nonpersistent (≤1 year) and persistent (>1 year) symptom diagnoses.
Methods: A retrospective cohort study was performed in a Dutch practice-based research network including 28,590 registered patients. We selected symptom diagnosis episodes with at least 1 contact in 2018. We performed descriptive statistics, Student’s T and χ2 tests to summarize and compare patients’ characteristics and GP management strategies in the nonpersistent and persistent groups.
Results: The incidence rate of symptom diagnoses was 767 episodes per 1000 patient-years. The prevalence rate was 485 patients per 1000 patient-years. Out of the patients who had a contact with their GPs, 58% had at least 1 symptom diagnosis, from which 16% were persistent (>1 year). In the persistent group, we found significantly more females (64% vs 57%), older patients (mean: 49 vs 36 years of age), patients with more comorbidities (71% vs 49%), psychological (17% vs 12%) and social (8% vs 5%) problems. Prescriptions (62% vs 23%) and referral (62.7% vs 30.6%) rates were significantly higher in persistent symptom episodes.
Conclusion: Symptom diagnoses are highly prevalent (58%) of which a considerable part (16%) persists more than a year.
- Epidemiology
- Family Medicine
- Morbidity
- Retrospective Studies
- Signs and Symptoms
Introduction
Making a diagnosis is a complex aspect of general practice.1,2 The task of the GP to make the correct diagnosis is complicated by the combination of dealing with symptoms at an early stage of development, the presence of multiple symptoms and the dynamic nature of symptoms.3 When the relevant diagnostic criteria of a disease are not fulfilled and symptoms cannot be attributed to a pathophysiological disease or syndrome, a “disease diagnosis label” is not appropriate.3,4 In this case, symptoms are used as diagnostic labels (ie, symptom diagnosis).3 Symptom diagnoses constitute an important part of the workload in general practice. Surprisingly, despite their clinical relevance in general practice, only limited attention is paid to symptom diagnoses as specific symptom labels in research, education and practice.5,6 Previous epidemiologic studies have shown that symptoms such as cough, back pain, and fatigue are among the leading diagnoses in GP settings.7,8 Of all diagnoses made in general practice, symptoms that cannot be attributed to a pathophysiological disease or syndrome ranged between 25% and 64%.6,8⇓⇓–11 Even though most of these studies report high symptom frequencies in general practice, a large variation in symptom frequencies has been noted. One of the explanations for this variation might be the differences in research methods as most of these studies rely on self-report measures, small samples, short follow-ups or unstructured assessments.10 However, these methods might be prone to a lack of specific diagnoses, recall or missing data biases. Notably, none of the studies had access to a structured, large general practice data registry where all information pertaining to 1 health problem is systematically organized and stored in medical records. Therefore, morbidity rates of symptom diagnoses remain unclear.
Symptom diagnoses often involve short-term episodes, which get resolved spontaneously without a clearly defined illness nor treatment.12 However, persistent symptoms are found to be a major health concern in general practice.13,14
Longitudinal studies reveal that up to 40% of the symptoms presented in general practice evolve into persistent symptoms.6,10,15⇓⇓⇓–19 However, the stipulated duration for a symptom to be defined as a persistent symptom is not consistent in existing literature. This duration is seen to range from a few weeks to 1 year.6,10,15,16 Previous studies have found that the female sex, a high number of comorbidities and a low level of education are predictors for the persistence of symptoms.20,21 In addition, studies investigating the GP management strategies among patients with persistent symptoms have found a greater number of inappropriate referrals, unnecessary investigations, and medical prescriptions.3,22,23 Even though factors related to patients’ characteristics and GP management strategies have been previously studied, all relevant factors found at present in routinely collected primary care data, have not been studied together.
Because symptom diagnoses are common in general practice, a considerable part of such diagnoses develop into persistent symptoms and because of the problems that GPs experience in the care for patients with persistent symptoms, a better understanding of morbidity rates and an early identification of patients who are at risk of developing persistent symptom diagnosis are needed. This might guide decisions about treatment and prevention. Hence, this study aims to explore the wide spectrum of symptom diagnoses in general practice including morbidity rates of symptom diagnosis, and to compare patient characteristics and management strategies for patients with nonpersistent and persistent symptom diagnoses.
Methods
The current study has been preregistered on Open Science Framework (Registration DOI: https://doi.org/10.17605/OSF.IO/JWGM5). The current study is part of the innovative training network ETUDE (Encompassing Training in fUnctional Disorders across Europe; https://etude-itn.eu/), a network that aims to improve the understanding of mechanisms, diagnosis, treatment, and stigmatization of functional disorders.24
Study Design and Settings
We performed a retrospective cohort study in which we analyzed data from the Family Medicine Network (FaMe-Net), a Practice Based Research Network in the Netherlands (https://www.famenet.nl). The FaMe-net dataset includes electronic medical records in general practice covering 308,000 patient-years and more than 2.2 million encounters from 2005 until 2019.25 The validity of data registration is high as regular meetings are held among GPs from the FaMe-Net to discuss the coding system and biannually online ‘uniformity’ surveys are conducted for creating coding uniformity through training.26 The FaMe-Net GPs code all doctor-patient contacts, within an Episode of Care (EoC) structure. An EoC is defined as “a health problem in a person from the first until the last encounter.”25 An EoC includes (1) the reason for encounter (the literal expression of the reason(s) why a person enters the consultation room),27 (2) the diagnoses, (3) the interventions (diagnostic interventions, treatment, and referrals), and (4) all encounters (visits) within this EoC.25 The EoC diagnosis may be modified during the encounters.25 For example, the diagnosis could change from ‘fatigue’ to ‘anemia’, when the laboratory results are revealed.25 This registration allows the GPs to review the evolution of the EoC.28 However, only 1 diagnosis could be attributed to 1 EoC at 1 specific point of time. The EoC interventions includes prescriptions for medication (treatment). Prescriptions for medication consist of electronic prescriptions written by GPs and delivered immediately by pharmacies.
Ethical Approval
The Radboudumc Medical Ethics Review Committee in Nijmegen in the Netherlands has approved the use of the FaMe-Net data for scientific research (CMO declaration number: 2020 to 6871). All patients were informed and gave consent for their participation in the FaMe-Net with the option to opt-out. The extraction of the FaMe-Net data are pseudonymized.
Data Collection and Measurements
All morbidity in the FaMe-Net dataset is coded according to the second edition of the International Classification of Primary Care (ICPC-2).29 ICPC is the only coding system available in primary care data registries in the Netherlands. ICPC-2 includes 15 chapters referring to organ/system problems, 1 chapter referring to psychological problems and 1 chapter referring to social problems. In addition, ICPC-2 includes 7 main components: symptom codes (component 1), process codes (components 2 to 6), and specific disease codes (component 7) which are identical across all the chapters.
ICPC-2 resembles the International Classification of diseases (ICD) with regard to the specific diseases part. Indeed, ICD has been designed to promote international comparability in the collection, processing, classification, and presentation of mortality statistics.28 However, ICD lacks codes for several symptoms and nondisease conditions encountered in primary care.28 ICPC-2 provides an extensive list of specific codes for a wide range of symptoms presented by patients in general practice.28
Symptom Diagnosis
Symptom diagnosis is a specific diagnosis after ICPC-2.28 Symptom diagnosis is a concept which prevents the harm caused by nonspecific disease diagnosis.3 It is modeled on the patient’s request for care, and reflects a primary care approach dealing with high levels of uncertainty.3
We selected all EoC with a symptom diagnosis (component 1) with at least 1 contact in 2018 (index year) for all enlisted patients over a study period from 1978 to 2020.
We selected all encounters with a symptom diagnosis, including face-to-face encounters, encounters during out-of-service hours, telephonic consultations, and e-consultations. To set a threshold for persistent symptoms, we first explored the distribution of symptom durations across our data, and discussed the results with expert GPs in the field of symptom research and clinical practice. Consequently, an EoC duration of 1 year was set as the threshold dividing the nonpersistent symptom diagnosis and the persistent symptom diagnosis groups.
An overview of all studied ICPC symptom diagnoses is summarized in Appendix 1.
Patients’ Characteristics
Based on data gathered from electronic medical records, we collected patients’ characteristics in 2018 (eg, age, sex, level of education, marital status, employment, and experience of physical, psychological, or sexual abuse). In addition, we collected chronic comorbidities before the first contact in 2018 (Appendix 2), psychological symptoms (EoC with at least 1 contact in 2018 for an ICPC-2: P01-P29 over a study period from 1978 to 2020) and social problems (EoC with at least 1 contact in 2018 for an ICPC-2: Z01-Z29 over a study period from 1978 to 2020). All characteristics variables of the patients were studied from the level of the patient.
GP Management Strategies
We identified the coded GP management strategies within the EoC including the number of EoC with at least 1 prescription for medication, the numbers and types of diagnostic interventions, therapeutic interventions, and referrals. All GP management strategies were studied from the level of the EoC. The name of all interventions or management strategies as well as ICPC-2 related codes are summarized in Appendix 3.
Statistical Analysis
The incidence rate of symptom diagnosis in 2018 (in EoC per 1000 patient-years) was defined as follows: the number of new EoC divided by the number of patient-years of the population per 1000 patient-years.30 The prevalence rate of symptom diagnosis in 2018 (in patients per 1000 patient-years) was defined as follows: the number of patients with a new or already existing EoC with a symptom diagnosis in 2018 divided by the number of patient-years of the population per 1000 patient-years.30 Patient-years refers to the total average number of patients registered with the GP practice during the predetermined time period of the year 2018.
Descriptive statistics were reported to summarize patients’ characteristics, GP management strategies and the duration of symptom diagnosis in the form of mean (Standard Deviation [S.D.]), median (interquartile [IQR]) or frequencies (%) as appropriate. To compare patients with persistent and nonpersistent symptoms, Student’s t test (for continuous variables) and a Pearson’s Chi-square test (for categorical variables) were performed as appropriate.
Data were analyzed using Statistical Package for Social Science (SPSS) version 25.0 for Windows. A p-value of < 0.05 was considered to be statistically significant.
Results
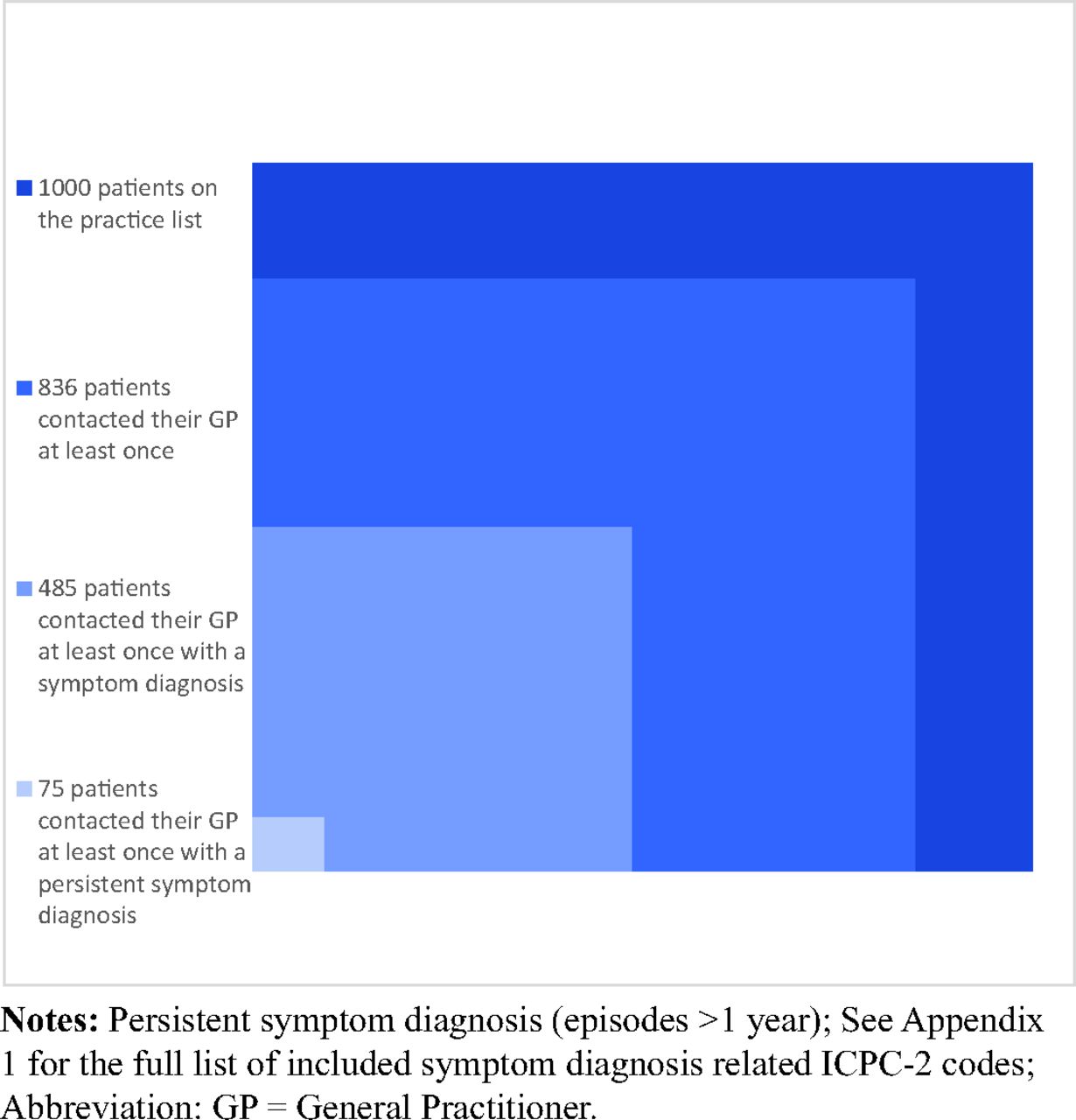
A total of 28,590 patients were registered on the general practice lists in 2018. The total number of patients who had at least 1 symptom diagnosis was 13,868, representing 48.5% of the enlisted patients and 57.9% of the patients who had contact with their GPs at least once in 2018. Among the 13,868 patients with a symptom diagnosis, 2172 (15.7%) had at least 1 persistent symptom diagnosis (Figure 1). The total number of symptom diagnoses episodes was 25,375, of which 2494 (9.8%) were persistent symptom diagnoses.

Proportion of patients with (persistent) symptom diagnosis in primary care (per 1000 patients, n = 28,590, contact year: 2018, study period: 1978 to 2020).
During the year 2018, the incidence rate of symptom diagnosis was 767 EoC per 1000 patient-years and the prevalence rate of symptom diagnosis was 485 patients per 1000 patient-years.
Cough (4.4%), weakness (4.3%), and abdominal pain (3.4%) were among the top 3 leading nonpersistent symptom diagnoses (Figure 2). Weakness (5.5%), constipation and low back pain (3.5%) were among the 3 most frequently persistent symptom diagnoses.

{kind=link}
{kind=link}
Frequencies of the top 10 symptom diagnoses in general practice (contact year: 2018, study period: 1978 to 2020).
Patients’ Characteristics
Out of the 13,868 patients with a symptom diagnosis, 5811 patients (41.9%) were males. The mean age was 38 years (S.D. = 23 years) and 7265 (52.4%) patients had 5 or more comorbidities.
The persistent symptom group included significantly more females (63.8% females vs 57.0% males, P < .001), older patients (a mean age of 49 years vs 36 years), and patients with more comorbidities (70.9% vs 48.9%, P < .001) compared with the nonpersistent group (Table 1). In addition, patients with persistent symptoms reported more previous psychological, physical and/or sexual abuse (16.4% vs 13.1%, P < .001) and had more psychological symptoms (17.4% vs 11.5%, P < .001). The patients with 1 or more symptom diagnosis that persisted for more than a year were less likely to be employed (64.5% vs 74.6%, P < .001), had a lower level of education (no formal education or less than 8 years of formal education: 5.6% vs 3.5%, P < .001), and more social problems (7.9% vs 4.8%, P < .001) compared with patients with nonpersistent symptom diagnoses.
Patient Characteristics of Non-Persistent and Persistent Groups Symptom Diagnosis (Contact Year: 2018, Study Period: 1978 to 2020)
GP Management Strategies
The overall median duration of symptoms was 0 days (IQR: 0–20) (nonpersistent group: 0 days [IQR: 0–7], persistent group: 1240 days [IQR: 665–2303]). A median duration of 0 days stands for only 1 consultation with the GP.
The median number of contacts with the GP for the overall group was 1 (IQR: 1–2). This median number was lower in the nonpersistent group (1 [IQR: 1–2]) when compared with the persistent group (4 [IQR: 2–7]).
The number of symptom episodes, with at least 1 written prescription, was 6824. As summarized in Table 2, episodes with at least 1 prescription were significantly higher in the persistent symptom diagnosis group (61.7% vs 23.1%, P < .001) compared with the nonpersistent group. Episodes with at least 1 referral were significantly higher in the persistent symptom diagnosis group compared with the nonpersistent group (62.7% vs 30.6%, P < .001).
Episodes Characteristics and the GP’s Management Strategies for Non-Persistent and Persistent Symptom Diagnosis (Contact Year: 2018, Study Period: 1978 to 2020)
Discussion
Summary of Main Findings
We found that symptom diagnoses in organ/system chapters are highly common in general practice. In 1 year, almost half of the registered patients and more than half of the patients who contacted their GPs at least once had a symptom diagnosis. Approximately 1 in 6 patients with a symptom diagnosis had at least 1 symptom diagnosis persistent more than a year. Persistent symptoms were significantly more prevalent in females, older people, patients with more comorbidities, and psychological and social problems. Prescriptions and referral rates were significantly higher in persistent symptom episodes when compared with nonpersistent episodes.
Comparison to Literature
To the best of our knowledge, this is the first study to explore the incidence and prevalence rates of symptom diagnosis. The incidence rate of symptom diagnosis of 767 EoC per 1000 patient-years was found to be higher than the prevalence rate of 485 patients per 1000 patient-years. These findings indicate that symptom diagnoses are more frequent and less persistent.31
Studies focusing on specific symptom labels such as Medically Unexplained Symptoms (MUS) or persistent somatic symptoms tended to find lower symptoms frequencies ranging between 3% and 30%.32⇓–34 These findings reflect that symptom diagnoses include a broader range of symptoms beyond these labels. As such, Rosendal et al. (2016) using the same classification (ICPC-2) as in our study to define symptom diagnosis, found a higher frequency of symptoms (36%) when compared with studies using other labels.11 However, Rosendal et al. (2016) claimed that the symptom frequencies in their study could be underestimated.11 This is because only 1 diagnosis label was given to each patient for the purpose of the research study, although the patient could report several health problems.11 Our findings (57.9%) were in congruence with other studies that explored a broad range of symptoms in general practice (ranging between 38% and 64%), even though these studies looked only at the most common symptoms in general practice.6,8,10
In our study, we found that 15.7% patients had at least 1 persistent symptom diagnosis. Studies on symptoms with a follow-up period of 1 year shared a higher prevalence of persistence symptoms between 20% to 38% of the cases.10,18,19 This difference could be explained by using different methodologies.
In fact, we calculated the prevalence retrospectively based on a GP data registry. In 1-year follow up studies on symptoms in general practice, the prevalence of persistent symptoms was calculated prospectively in the course of 2 interviews that occurred at the beginning and the end of these studies.10,18,19 This prospective method may not reflect the dynamic of GP practices. For instance, a quarter of participants who still experienced symptoms did not visit their GP on their own initiative during the 12-months follow up period.10,19
In this study, cough, weakness, and abdominal pain were among the most common symptom diagnoses. These symptoms were also reported as the most commonly presenting symptoms in general practices in the Netherlands, Canada, United States and Norway.7,11,34,35 This could suggest that the presentation of health care problems in Western countries, more specifically symptom diagnoses in general practice, might be similar to each other.
Our findings that persistent symptoms were more prevalent in females, older patients, patients with more comorbidities, patients who experienced abuse and with coexisting psychological symptoms correspond to other studies.14,15,21,32,34⇓⇓–37 In addition, in line with previous studies, patients with persistent symptoms had a lower socioeconomic status including lower rates of employment,14,32 more coexisting social problems,37 and a lower level of education.21,32,37
In line with previous literature, we found that GPs prescribed medical prescriptions and referrals significantly more often when the symptoms were persistent.23,34 Even though this might be explained by a longer duration of care and therefore more opportunities for prescriptions and referrals, high referral rates among patients with persistent symptoms may point toward GPs uncertainty and insecurity when handling persistent symptom diagnoses.
Strengths and Limitations
This study has several strengths. A major strength is the use of FaMe-Net data set that includes a large number of patients, contacts, and an episode-oriented structure. FaMe-Net is the only existing dataset, where GPs register the health problem within an EoC structure and are trained to recode episodes when symptoms evolve into diseases.26 It has been demonstrated to be a valid, long-lasting, detailed, structured and accurate general practice data registry.26 In addition, the outcome symptom diagnosis was a diagnosis as documented by GPs in daily routine practice.
Our study also has a number of limitations. Despite the high validity of the FaMe-Net dataset, the absence of information on billing requirements and information on data from other health care providers in the General Practice might have an impact on morbidity levels of symptom diagnosis. For a better description of symptoms, it is important to study the severity levels of symptoms and the level of burden.38 However, our definition of symptom diagnosis did not include these levels due to the absence of a structurally coded severity and burden levels in our GP data registry. We distinguished patients with nonpersistent and persistent symptoms based on the duration of their symptoms. Furthermore, even though the GPs are equipped to diagnose diseases and syndromes and trained to code the diagnosis at the highest level of certainty at that specific moment, it is still possible that some symptoms are undiagnosed diseases, and therefore, the morbidity rates of symptom diagnoses might be overestimated. Nevertheless, our findings are a reflection of general practice, where the GPs encounter challenges in making relevant diagnoses.
Future Research and Clinical Implications
Symptom research is in line with the philosophy of general practice as it empowers patients request of care and follows the person-centered approach.3,39 We provide a reliable estimation of morbidity rates of symptoms diagnosis including incidence and prevalence rates. Indeed, the gatekeeper role of the GP and the mandatory registration of all residents in the Netherlands to a GP practice40 are expected to increase the reliability of our findings on morbidity rates. As a considerable part of GPs’ daily practice consists of managing symptoms rather than diseases, our findings justify more emphasis on symptom diagnosis research, education, and training in general practice. More research and guidelines on management strategies to deal with symptoms is necessary. As such, future research may focus on what factors predict the evolution from short to persistent symptoms. A better understanding of why unfavorable medical and socio-economic factors are more prevalent in persistent symptoms diagnoses is urgently needed to reduce health care inequalities.
Summary
Symptom diagnoses are highly prevalent in general practice. Almost half of the registered patients have at least 1 symptom diagnosis. More than half of the patients contact their GPs at least once a year for 1 or more symptom diagnoses. Approximately 1 in every 6 patients with symptom diagnosis have at least 1 persistent symptom diagnosis. The group of patients with persistent symptom diagnoses consists of more females, older people, patients who have more comorbidities, psychological and social problems. During persistent symptom diagnosis episodes, significantly more referrals and prescriptions are observed. This might suggest that we need to provide GPs with effective tools to guide their management strategies. Therefore, research to predict and prevent an unfavorable course to reduce health inequality is needed.
Acknowledgments
Authors thank Georg Grewer and Martin Liebau for their help in this study. Authors also would like to thank all General Practitioners from the Family-Medicine Network for their participation in collecting data for this study.
Appendices.
Appendix 1. Overview of All Studied Symptom Diagnoses from the International Classification of Primary Care, Second Edition (ICPC-2)

Appendix 2. List of Comorbidities


Appendix 3. List of Interventions Related Codes in the 2nd Version of the International Classification of Primary Care (ICPC-2)

Appendix 4. List of Referrals Related Codes the 2nd Version of the International Classification of Primary Care (ICPC-2)

Appendix 5. Number of Comorbidities Stratified by Age Categories in the Persistent and Non-Persistent Groups

Notes
This article was externally peer reviewed.
Funding: This project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 956673 and is part of the Training Network Encompassing Training in fUnctional Disorders across Europe (ETUDE). The funding source had no role in study design, the collection, analysis and interpretation of data, in the writing of the report and in the decision to submit the article for publication.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/36/3/477.full.
- Received for publication September 27, 2022.
- Revision received January 23, 2023.
- Accepted for publication January 27, 2023.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.