Abstract
Background: Thyroid disorders are among the most commonly treated conditions by the United States health care system. The number of patients reporting thyroid hormone use has increased in recent years, but it is unknown if there have been differential increases in the number of treated individuals within different demographic groups. Previous research has also not evaluated how expenditures for different thyroid hormone medications have changed in recent years.
Methods: Using data from the 1997 through 2016 Medical Expenditure Panel Survey, we calculated the proportion of adults reporting thyroid hormone prescriptions by 3 demographic variables (age, sex, and race) and determined expenditures from thyroid hormone prescriptions by medication type (overall, generic, Synthroid or Cytomel, and other brand).
Results: Between 1997 and 2016, the proportion of adults who reported thyroid hormone use increased from 4.1% (95% CI, 3.7–4.4) to 8.0% (95% CI, 7.5–8.5). Most of the growth in thyroid hormone use occurred among adults aged >65, and use was also more common among females and non-Hispanic whites. Expenditures from thyroid hormones increased from $1.1 billion (95% CI, 0.9–1.3) in 1997 to $3.2 billion dollars (95% CI, 2.9–3.6) in 2016. Generic thyroid hormone prescriptions comprised 18.1% of all thyroid hormone prescriptions in 2004 (95% CI, 15.8–20.4) and 80.8% of all thyroid hormone prescriptions (95% CI, 78.4–83.2) in 2016.
Conclusions: Thyroid hormone use nearly doubled over the last 20 years, and increased use was associated with being older, female, and non-Hispanic white. During the same time period, thyroid hormone expenditures almost tripled.
- Data Analysis
- Health Expenditures
- Health Services Research
- Hypothyroidism
- Thyroid Diseases
- Thyroid Hormones
Introduction
Thyroid hormones are among the most commonly used classes of medications in the United States.1 Although approved by the Food and Drug Administration for numerous conditions, including clinical hypothyroidism, thyroid hormones are also commonly used for unapproved conditions, such as subclinical hypothyroidism, depression, and weight reduction.2 Although the prevalence of overt hypothyroidism is thought to be between 0.2% and 2%, with a stable incidence, the proportion of the adult population who report using a thyroid hormone has increased in recent years.2 We, therefore, sought to characterize the proportion of adult individuals using thyroid hormones by age, sex, and race/ethnicity from 1997 through 2016. We also aimed to describe the costs associated with all thyroid hormone prescriptions between 1997 and 2016 and mean per user expenditures from different thyroid hormone types between 2004 and 2016.
Methods
The 1997 to 2016 Medical Expenditure Panel Survey (MEPS) was used for the analysis.3 The Agency of Health care Research and Quality sponsors the survey, which is nationally representative of the noninstitutionalized United States population. MEPS collects sociodemographic, medical condition, and prescription medication information from 2 overlapping cohorts over 2 years. Prescription drug information is reported by individuals and confirmed through pharmacies. Reporting of chronic medications by MEPS participants has been found to be reliable.4
Our sample included all adult (age, >17) MEPS participants. Thyroid hormones were identified by therapeutic subgroup (Multum therapeutic sub-class #1 [TC1S1] = 103) and confirmed with prescription drug names. We differentiated thyroid hormone medications by prescription drug name as Synthroid and Cytomel, other brand, or generic prescriptions starting in 2004, when generic levothyroxine was available.
Thyroid hormone expenditures included out-of-pocket and insurance payments. Expenditures were inflation adjusted to 2016 US dollars by using the Consumer Price Index.5
Adjusted Wald tests were used to determine if there were statistically significant differences in the proportion of medication users and medication expenditures at different time points. A multivariable logistic regression model that included age, age2, sex, and interaction terms between these 3 variables compared the proportion of thyroid hormone users by age and sex during 1997 to 1999 and 2014 to 2016. Another model that included these same variables but added race/ethnicity, year, and an interaction term between race/ethnicity and year investigated thyroid hormone use by race/ethnicity during 1997 to 2016. Each model was followed by postprediction average marginal effects.
The OhioHealth Institutional Review Board ruled this study exempt. Stata, version 15, with survey weights applied, was used for the analysis. Four outliers (>$2500/year) were excluded from expenditure estimates. P values less than .01 were considered statistically significant.
Results
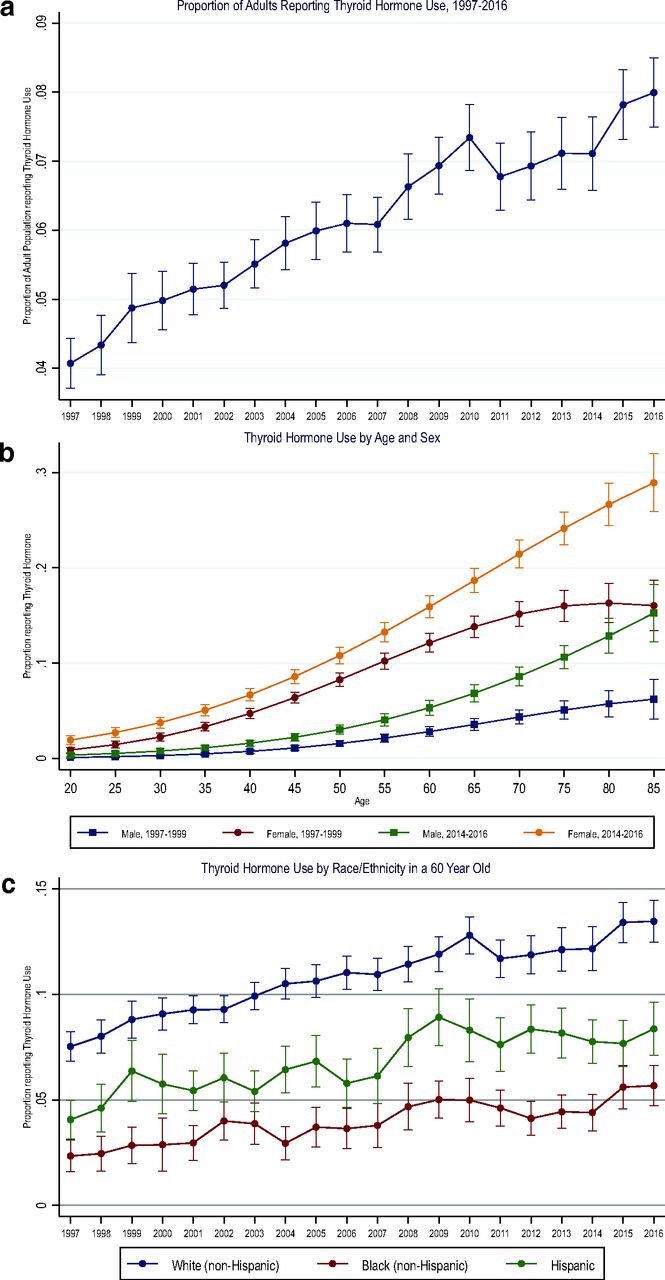
Based on the 470,067 adults in our sample, we found that the proportion of the US population who reported thyroid hormone use increased from 4.1% (95% CI, 3.7–4.4) in 1997 to 8.0% (95% CI, 7.5 to 8.5) in 2016 (P < .001) (Figure 1a). Use generally increased with increasing age, but the growth in utilization between 1997 to 1999 and 2014 to 2016 was predominantly among individuals older than 65 years of age. Use was also higher among women than men (Figure 1b) and higher among non-Hispanic whites (Figure 1c) than non-Hispanic blacks and Hispanics. However, the increase was not significantly different between non-Hispanic whites and non-Hispanic blacks (adjusted odds ratio [aOR] interaction term 1.01 [95% CI, 0.99–1.03], P = .29) or Hispanics (aOR interaction term 1.00 [95% CI, 0.99–1.02], P = .74).

Top (1a): The figure identifies the proportion of US adults who reported filling a thyroid hormone replacement prescription in a calendar year between 1997 and 2016. Center (1b): Estimated proportion of US adults from 1997 to 1999 and 2014 to 2016 who reported thyroid hormone replacement by age and sex. Estimates were calculated using postprediction average marginal effects after performing the multivariable logistic regression described in the Methods section. Bottom (1c): Predicted proportion of population between 1997 and 2016 that reported thyroid hormone replacement by race/ethnicity, adjusted for age and sex. Error bars represent 95% CIs. Abbreviation: CI, Confidence interval.
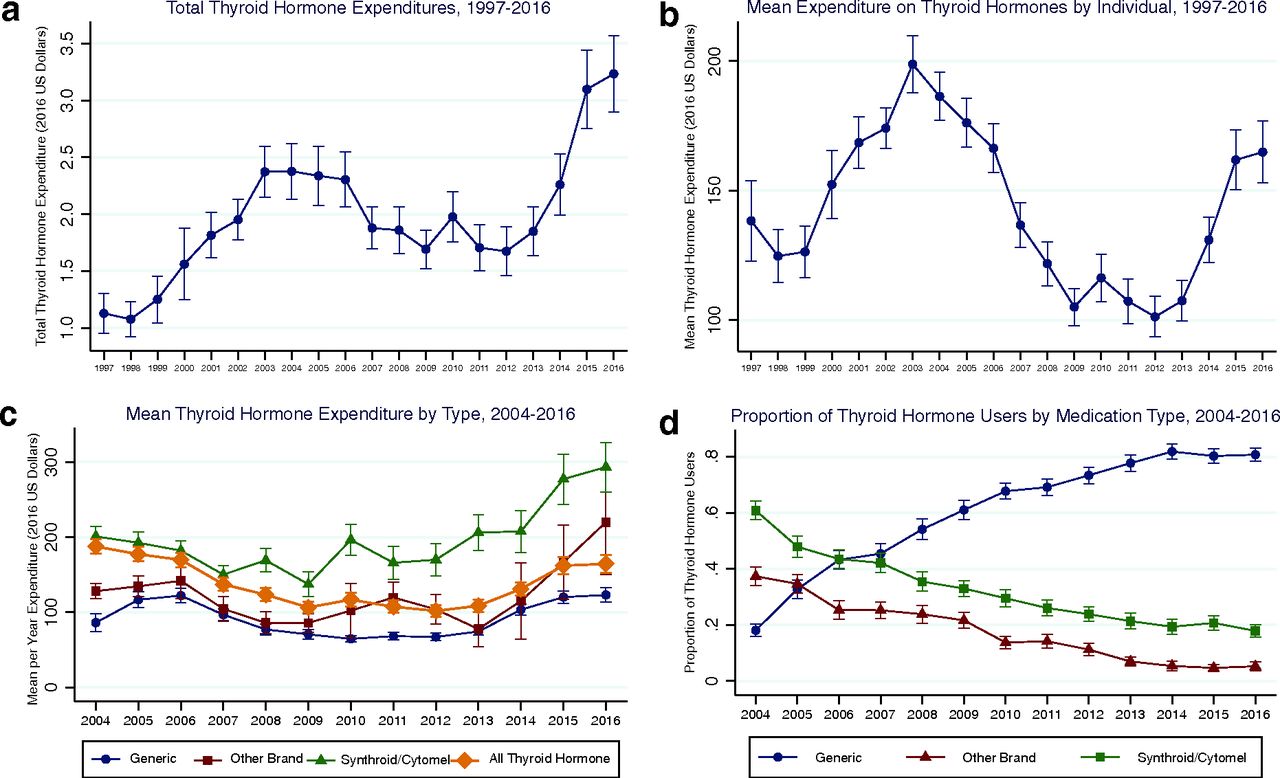
Thyroid hormone expenditure increased from $1.1 billion (95% CI, 0.9–1.3) in 1997 to $3.2 billion (95% CI, 2.9–3.6) in 2016 (Figure 2a). Mean annual per user expenditures followed a similar pattern as overall expenditures (Figure 2b). Mean user brand and generic thyroid hormone expenditures increased toward the end of the study, with generic thyroid hormone increasing from $64.6 per year (95% CI, 60.3–68.9) in 2010 to $123.0 per year (95% CI, 113.4–132.7) in 2016 (P < .001) (Figure 2b). The proportion of thyroid hormone users who reported using generic thyroid hormone increased to 80.8% (95% CI, 78.4–83.2) in 2016 from 18.1% (95% CI, 15.8–20.4) in 2004 (Figure 2c).
{kind=link}
{kind=link}
Top Left (2a): Total expenditure from thyroid hormone between 1997 and 2016. Top right (2b): Mean thyroid hormone expenditure per person/year between 1997 and 2016. Pharmaceutical rebates were not included in the calculations. Bottom left (2c): Mean expenditure per person/year by generic, Synthroid/Cytomel, and other brand thyroid hormone between 2004 and 2016. Pharmaceutical rebates were not included in the calculations. Bottom right (2d): Percentage of thyroid hormone users who reported generic, Synthroid/Cytomel, and other brand thyroid hormones between 2004 and 2016. Individuals can be included in multiple categories. All expenditures were adjusted to 2016 US dollars using the Consumer Price Index. Error bars represent 95% CIs. Abbreviation: CI, Confidence interval.
Discussion
This study found that between 1997 and 2016 thyroid hormone use increased among all US adults. Thyroid hormone use was associated with being non-Hispanic white, female, and elderly. During the same time interval, thyroid hormone expenditures almost tripled.
Because our data source did not include information on the specific indications for initiating thyroid hormone treatment, we were unable to determine why there was an increase over time in overall thyroid hormone use. However, previous research strongly implies that recent increases in thyroid hormone use are predominantly from a rise in the treatment of subclinical hypothyroidism rather than overt hypothyroidism. Subclinical hypothyroidism is notably more common than overt hypothyroidism and is unlikely that around 8% of the population has overt hypothyroidism. In addition, research using data from the National Health and Nutrition Examination Survey showed that thyroid-stimulating hormone (TSH) values are greater among females, increase with age, and are higher in non-Hispanic whites than Mexican Americans and African Americans.6 Higher TSH values among females, older individuals, and non-Hispanic whites combined with the trend toward initiating thyroid hormone treatment among individuals with lower median TSH levels, which was demonstrated in a study performed in the United Kingdom,7 may together explain why both overall thyroid hormone prescriptions and thyroid hormone prescriptions within certain demographic groups have increased over time.
If the increase in thyroid hormone use among US adults was truly from increases in the treatment of subclinical hypothyroidism, thyroid hormone use within the US adult population merits critical scrutiny because of the uncertain benefits from treating subclinical hypothyroidism and the substantial cost to our health care system from thyroid hormone prescriptions. There is no strong evidence to suggest that thyroid supplementation for patients with subclinical hypothyroidism results in improved cardiovascular or survival outcomes,8,9 quality of life, cognitive function, blood pressure, or body mass index.10,11 Moreover, despite increases in the proportion of generic thyroid hormone prescriptions over time, total expenditures on thyroid hormones increased steadily between 1997 and 2016. These increases were likely related to a greater number of individuals being prescribed a thyroid hormone and recent increases in per person expenditures from both brand name and generic thyroid hormone prescriptions.
This study’s limitations included the use of self-reported medications, lack of controlling for pharmaceutical rebates (which are not thought to flow back to the payer for most generic medications),12 and potential misclassification of brand versus generic levothyroxine. Moreover, because of the cross-sectional nature of MEPS and its lack of laboratory data, we were unable to determine if the differential increases in thyroid hormone was due to increases in treatment for overt or subclinical hypothyroidism. In addition, we were also not able to add information about whether some of the increase in treatment could be related to more individuals being screened for hypothyroidism.
In conclusion, total expenditures on thyroid hormones almost tripled between 1997 and 2016. A disproportionate increase in thyroid hormone use was associated with being female, identifying as non-Hispanic white, and being older.
Acknowledgments
Michael Johansen had full access to all the study data and takes responsibility for the integrity of the data and the accuracy of the data analysis. The authors have no conflicts of interest to report. No funding was used on this research.
Notes
This article was externally peer reviewed.
To see this article online, please go to: http://jabfm.org/content/33/2/284.full.
- Received for publication April 30, 2019.
- Revision received August 8, 2019.
- Accepted for publication August 9, 2019.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.