Abstract
Background: The United States is facing a widespread opioid epidemic that disproportionately affects the working-age population. In the clinical setting, new low back pain is one of the most common reasons for opioid prescriptions, despite national recommendations advising against their use until nonopioid treatments have been trialed. In this study, we aimed to examine national opioid prescribing practices among primary care physicians after the evaluation of low back pain in working-age patients.
Method: This study used a national claims database's billing codes to identify patients in the outpatient setting with a new encounter for isolated low back pain following a 1-year look-back period. The primary outcome was whether an opioid prescription was filled within 30 days after the encounter. Patients with a daily morphine milligram equivalence (MME/day) known to be associated with a higher risk of overdose were also analyzed.
Results: A total of 418,565 patients between January 1, 2011 and November 30, 2016 were included. The proportion of patients with filled opioid prescriptions declined significantly between 2011 and 2016 (P < .01; 28.5% in 2011, 27.6% in 2012, 26.3% in 2013, 25.5% in 2014, 23.5% in 2015, and 20.4% in 2016). Nationally, the proportion of patients with a filled opioid prescription varied significantly between states (P < .01), ranging from 12.9% in Hawaii to 33.6% in Arkansas.
Discussion: We found that the overall frequency of opioid prescriptions for low back pain is decreasing nationally, which speaks favorably for future initiatives to change physician prescribing patterns. However, we identified that there is large variation in prescribing patterns among physicians in different states.
- Low Back Pain
- Opioids
- Outpatients
- Physician's Practice Patterns
- Prescriptions
- Primary Care Physicians
- Primary Health Care
- Quality of Health Care
The United States is facing a widespread opioid epidemic that disproportionately affects the working-age population. In fact, 1 in 5 deaths in young adults between 25 and 34 years of age are related to opioid use.1 In the clinical setting, new low back pain is one of the most common reasons for opioid prescriptions, despite national recommendations advising against their use until nonopioid treatments have been trialed.2,3 There is a lack of demonstrable long-term benefit of opioids and randomized clinical trials have shown their use to be associated with worse or similar long-term pain outcomes, as well as a dose-dependent risk of harm, compared with nonopioid medication.4,5
In light of the current nationwide focus on opioid-related health-care policy and future directives, we aim to examine opioid prescribing practices among primary care physicians after the evaluation of new low back pain in working-age patients.
Methods
This study used the IBM Health MarketScan® Commercial Claims and Encounters Database, which contains health information on private-payer insurance beneficiaries across the United States. ICD-9 724.2 or ICD-10 M54.4 billing codes were used to identify patients in the outpatient setting with a new encounter for isolated low back pain following a 1-year look-back period. Patients with any concurrent encounter ICD code and, therefore, also of any concurrent spinal pathology diagnosis, were excluded. In addition, excluded were patients who within the prior 12 months had an encounter billed in the database for a visit with a subspecialist physician, for example, an orthopedic surgeon or chronic pain specialist; patients who had filled opioid prescriptions within 90-days before their encounter of interest for low back pain; and patients who were captured in the database to have required forms indicative of chronic use.
The primary outcome was whether an opioid prescription of ≥20 daily morphine milligram equivalence (MME) was filled within 30 days after the encounter. This dose was selected, as opioid doses of greater than 20 MME/day have been shown to be associated with a higher risk of unintentional overdose compared with 0 to 20 MME/day.3,5 Proportions were imputed with IBM Health MarketScan trends and sampling weights. The Cochran-Armitage trends test was used for trends analysis. State variation was analyzed using χ2 test.
Results
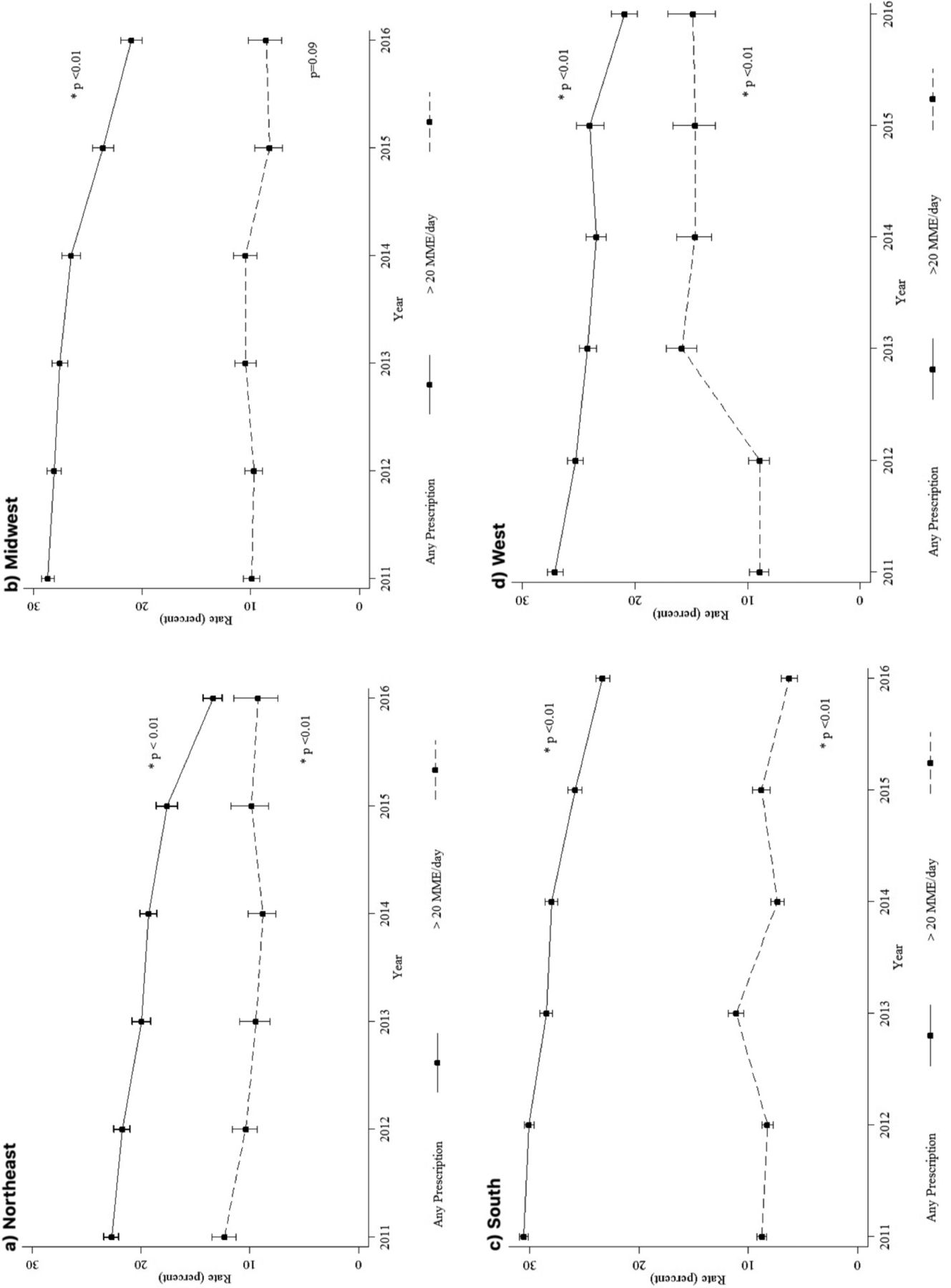
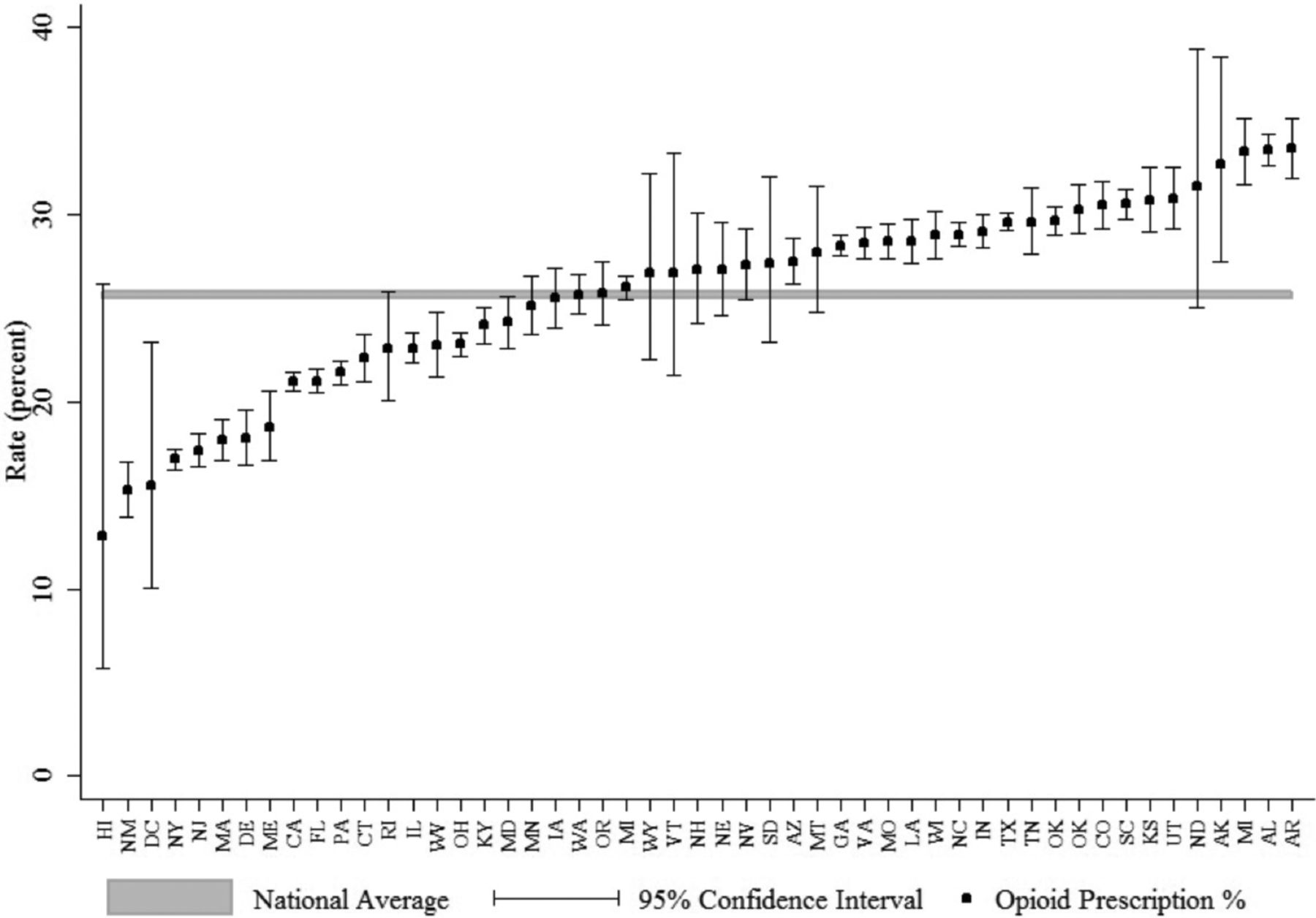
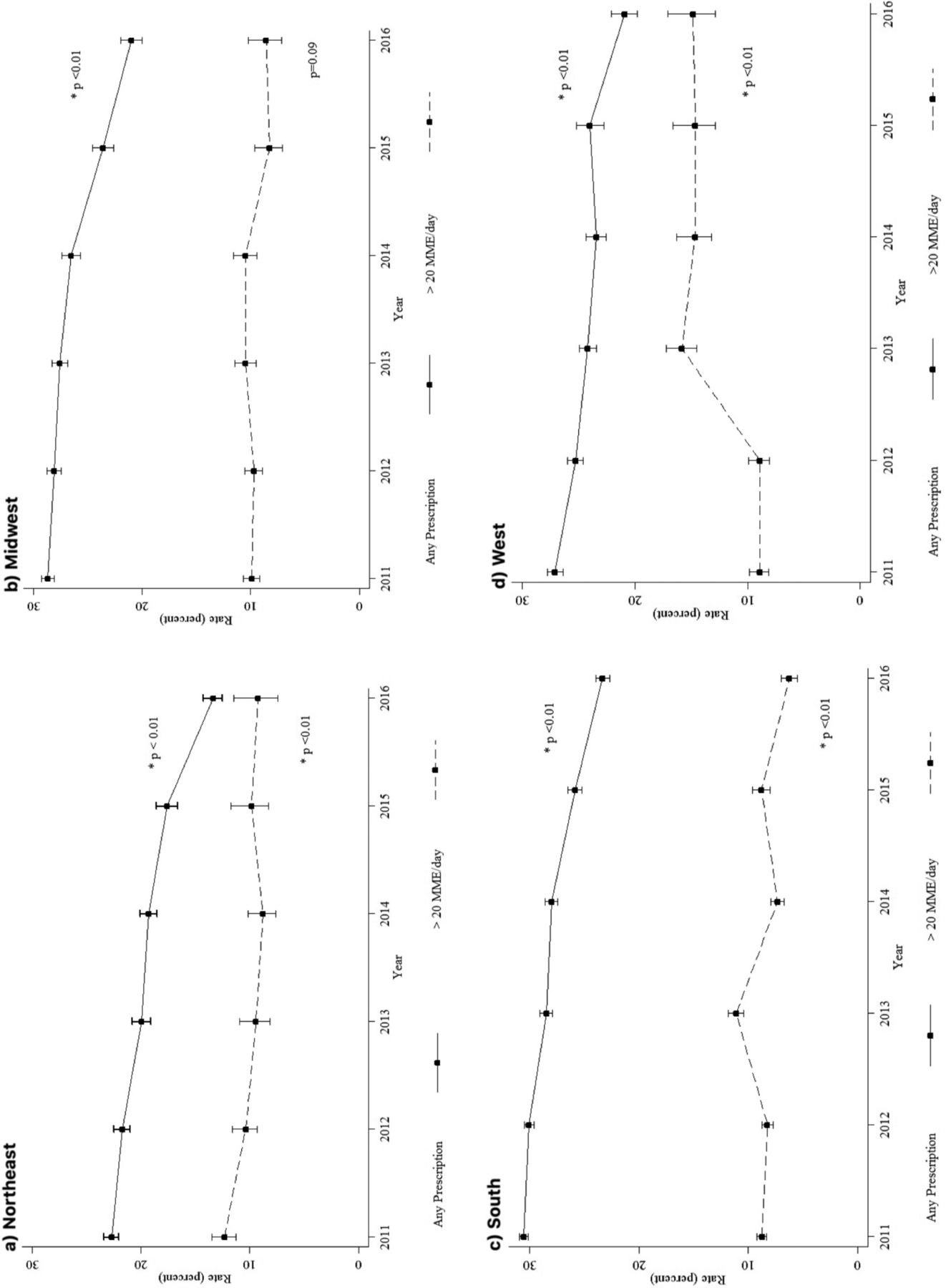
A total of 418,565 patients between January 1, 2011 and November 30, 2016 were included. Study population characteristics are displayed in Table 1. In our study population, 25.7% [95% CI: 25.6–25.9] of patients had a filled opioid prescription 30-days postencounter. Nationally, the proportion of patients with a filled opioid prescription varied significantly between the various states (P < .01), ranging from 12.9% in Hawaii to 33.6% in Arkansas (Figure 1). The proportion of patients with filled opioid prescriptions declined significantly between 2011 and 2016 (P < .01; 28.5% in 2011, 27.6% in 2012, 26.3% in 2013, 25.5% in 2014, 23.5% in 2015, and 20.4% in 2016). This decline was evident across the Northeast, Midwest, South, and West (Figure 2). Of those with a filled opioid prescription, the proportion with >20 MME/day did not significantly change over time (P = .16).
Characteristics of the Study Population
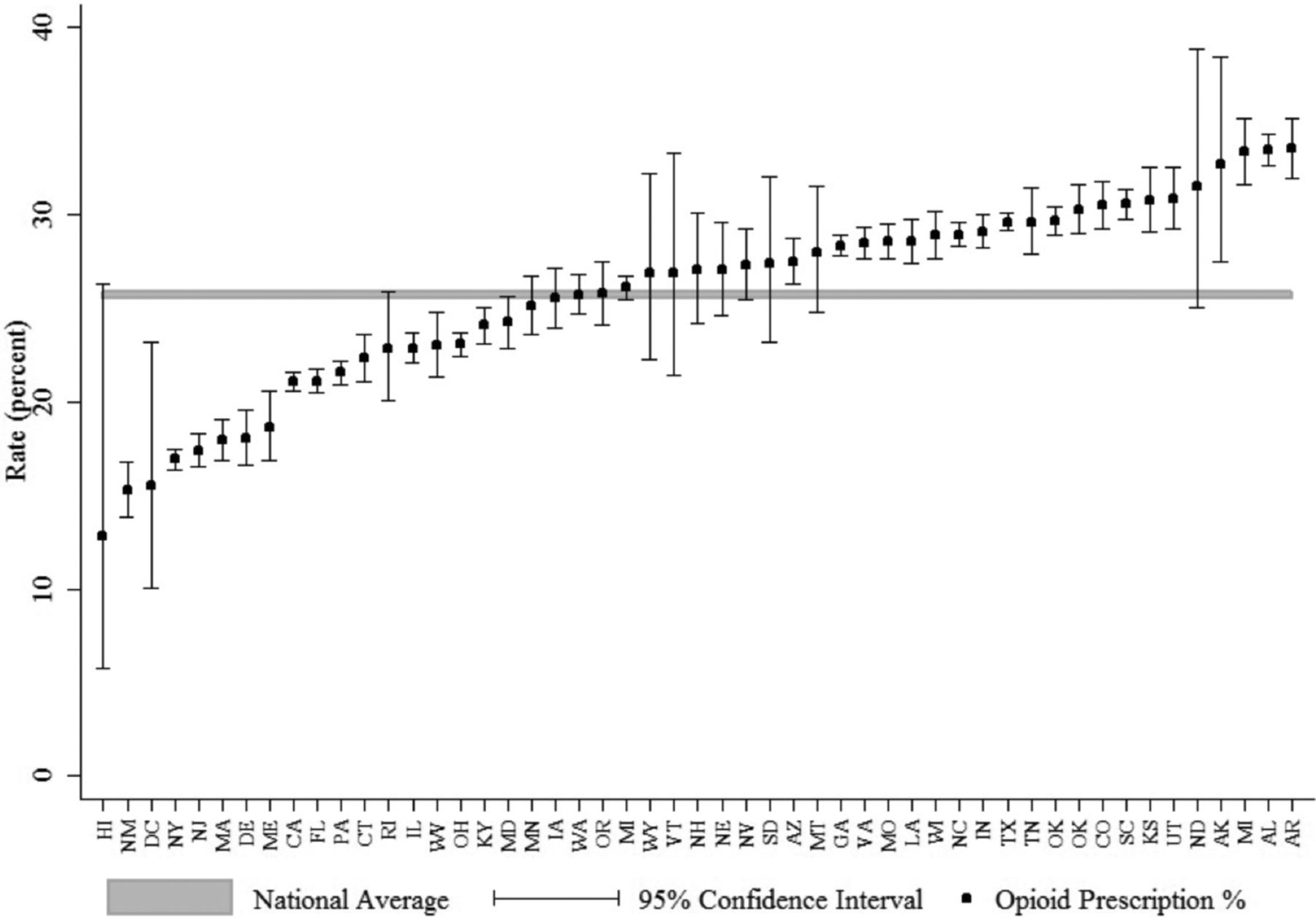
A caterpillar plot of the proportion of patients with a filled opioid prescription and the associated 95% logit confidence interval by state.
{kind=link}
{kind=link}
Regional scatter plots of the annual proportions of patients with any filled opioid prescription as well as the proportion of those with a filled prescription receiving more than 20 MME/day and their associated 95% logit confidence intervals. a: Northeast. b: Midwest. c: South. d: West.
Discussion
Encouragingly, the overall frequency of opioid prescriptions for new back pain encounters is decreasing nationally, which speaks favorably for future initiatives to change physician prescribing patterns. The underlying reasons for the reduction in opioid prescribing is unclear but almost certainly multifactorial. Such factors likely include an increased awareness for the current opioid epidemic in the United States and increased focus in national educational campaigns. For example, the American Board of Internal Medicine foundation's Choosing Wisely campaign has disseminated recommendations against the use of opioids for back pain before the trial of alternatives.6 These recommendations are supported by the American Association of Family Physicians. Other strategies may include increased use of state-wide prescription drug monitoring programs and “Harm Reduction” strategies. The latter strategy aims to decrease death from overdose through a combination of opioid substitutions, opioid education, concurrent supply of an opioid antagonist, and access to behavioral health services.7,8,9
However, although the overall trend is favorable, we further found that there is large geographic variation in prescribing patterns among physicians in different states. These findings add evidence to a current knowledge base that there is large variation in opioid prescribing among ordering providers and low back pain is no exception.10,11,12 Addressing geographic variation and discrepancies through local health policies and education efforts will continue to be needed to address the epidemic further. In addition, opioid prescriptions written at doses of ≥20 MME remained relatively stable in our study. In addition to current strategies, there may, therefore, be a need for clear unified guidelines not only for appropriate indications but also for dosing.
In addition to the role played by physicians in combating opioid overuse, there is also an opportunity for third-party payers in guiding high-value care, and recent evidence has demonstrated their utilization management requirements to be highly variable.13 Private insurers can restrict the reimbursement of inappropriate prescribing, for example, through prior authorization and visit requirements. Ultimately, opioid prescribing for low back pain continues to provide multiple challenges that will be best addressed by a multifaceted approach encompassing payers, physicians, and patients.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/33/1/138.full.
- Received for publication July 17, 2019.
- Revision received October 22, 2019.
- Accepted for publication October 23, 2019.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.