Abstract
Background: National studies report patients with limited English proficiency (LEP) have difficulty finding bilingual physicians; however, it is unclear whether this situation is primarily a result of an inadequate supply of bilingual physicians or a lack of the insurance coverage necessary to gain access to bilingual physicians. In California, 12% of urban residents are Spanish-speaking with some limited proficiency in English. The majority of these residents (67%) are uninsured or on Medicaid.
Methods: In 2001, we performed a mailed survey of a probability sample of primary care and specialist physicians practicing in California. We received 1364 completed questionnaires from 2240 eligible physicians (61%). Physicians were asked about their demographics, practice characteristics, whether they were fluent in Spanish, and whether they had Medicaid or uninsured patients in their practice.
Results: Twenty-six percent of primary care and 22% of specialist physicians in the 13 urban study counties reported that they were fluent in Spanish. This represented 146 primary care and 66 specialist physicians who spoke Spanish for every 100,000 Spanish-speaking LEP residents. In contrast to the general population, there were only 48 Spanish-speaking primary care and 29 specialist physician equivalents available for every 100,000 Spanish-speaking LEP patients on Medicaid and even fewer (34 primary care and 4 specialist) Spanish-speaking physician equivalents for every 100,000 Spanish-speaking physician equivalents for uninsured Spanish-speaking LEP patients.
Conclusion: Although the supply of Spanish-speaking physicians in California is relatively high, the insurance status of LEP Spanish-speaking patients limits their access to the physicians. Addressing health insurance-related barriers to care for those on Medicaid and the uninsured is critical to improving health care for Spanish-speaking LEP patients.
Inadequate health insurance and language barriers are 2 major factors that influence access to care for Latino immigrants.1 Many Latino immigrants are either uninsured or have Medicaid insurance coverage, limiting their ability to find physicians who are willing to care for them. Many physicians are unwilling to accept Medicaid patients because of low payment rates and administrative hassles and are even less willing to provide charity care.2–4 In addition, immigrants with limited English-speaking proficiency often have communication problems with providers, thus contributing to lower utilization of services, lower rating of care, and less satisfaction with care.5–9
To reduce barriers to care for people with limited English proficiency, recent federal and state policies have directed providers to provide linguistic services for these patients.10–12 Services can range from language phone lines to bilingual staff. National studies report patients have difficulty finding bilingual physicians;13 however, it is unclear whether this situation is caused primarily by an inadequate supply of bilingual physicians or a lack of the insurance coverage necessary to gain access to bilingual physicians.
Latinos are the largest minority group in the United States. Although Latinos are geographically concentrated in states such as California, Texas, New York, and Florida, between 1990 and 2000, the Latino population grew in every state except Hawaii. Latinos now comprise 12.5% of the nation’s total population.14 In California, almost one third of the state’s population is Latino, and 12% of the urban population consists of Spanish-speaking persons with some limited proficiency in English.15 Two-thirds of these Spanish-speaking persons with limited English proficiency (LEP) are uninsured or Medicaid beneficiaries.16,17
No prior studies have systematically evaluated the Spanish language capability of physicians in California or other states. Prior research has documented the problems of access to physician services related to insurance coverage. In California, only 54% of practicing physicians participate in the Medicaid program.18 An even smaller percentage (43%) of practicing physicians in the state have any uninsured patients in their practice. It is not known whether physicians fluent in Spanish are more or less likely to care for Medicaid and uninsured patients and therefore would be more available to Spanish-speaking LEP patients who are concentrated in these uninsured and Medicaid populations.
We performed a study to measure the availability and distribution of Spanish-speaking physicians in California. To determine the relative contributions of patients’ health insurance status and the supply of Spanish-speaking physicians to the availability of bilingual physicians for Spanish-speaking patients, we compared the supply of Spanish-speaking physicians for California’s total LEP Spanish-speaking population with the number of Spanish-speaking physicians for LEP Spanish-speaking Medicaid and uninsured patients.
Methods
Study Design
As a part of an on-going study of physicians in California, we conducted in 2001 a mailed survey of primary care and specialist physicians practicing in the state’s 13 largest urban counties. These counties include 78% of the state’s population including 77% of the Medicaid population and 78% of the state’s practicing physicians. The survey methods have been previously published in detail.19 In brief, these physicians were identified from the American Medical Association’s Physician Masterfile, a database of US allopathic and osteopathic physicians. Only physicians providing direct patient care, not in training, and not employed by the federal government were eligible for the survey. Physicians were drawn using a probability sample stratified by county, specialty, and physician race/ethnicity with an oversampling of black and Latino physicians. Black and Latino physicians were oversampled to obtain a sufficient sample size of physicians from these racial and ethnic groups who could be compared with white physicians who constituted the overwhelming majority of all physicians. Completed questionnaires were obtained from 1364 of the 2240 eligible physicians (61%). Response rates did not differ by physician sex, by specialists versus primary care physicians, or by county of practice location. Response rates were significantly higher (P < .05) for white physicians (71%) and those who were board-certified (65%).
To estimate physician skills in Spanish, physicians were asked which communication methods they would use if a patient with limited English skills who spoke Spanish came to their office for care. Those physicians who checked that they speak Spanish were considered fluent for the purposes of the analysis. Physicians were also asked about their demographics, training characteristics, practice characteristics, practice location, and patient characteristics.
Data Analysis
Analyses examining the availability of Spanish-speaking physicians were weighted to be generalizable to the overall population of physicians in the sampled specialties in the 13 study counties. Estimates of the percentage of physicians fluent in Spanish were derived from our physician questionnaire and applied to a count of the overall number of physicians in surveyed specialties in the study counties obtained from the AMA Physician Masterfile. We created separate ratios of the supply of Spanish-speaking primary care and specialist physicians per the number of LEP Spanish-speaking persons in the 13 study counties reported in the 2000 US Census.20 We compared these ratios with the total number of physicians from the AMA Physician Masterfile per total population regardless of language.
To assess the distribution of Spanish-speaking physicians among LEP Spanish-speaking patients, we compared the mean percentage of LEP Spanish-speaking residents in communities where Spanish-speaking physicians practiced with the mean percentage of LEP Spanish-speaking residents where non-Spanish-speaking physicians practiced. To determine whether the percentage of Latino and LEP patients in a physician’s practice was merely a reflection of the proportion of such patients in the community, we compared the mean percentage of Latino and LEP patients in physicians’ practices for Spanish-speaking and non-Spanish-speaking physicians controlling for the mean percentage of LEP Spanish-speaking residents in the community. Communities used in the analysis were subcounty geographic areas defined by clusters of contiguous zip codes; they correspond to areas used by the state for health care workforce planning.21
We operationalized the supply of physicians available to Medicaid and uninsured patients as a function of the number of physicians caring for Medicaid and uninsured patients and the respective percentage of such patients in their practices. We calculated Medicaid Spanish-speaking physician equivalents by multiplying the mean percentage of Medicaid patients in the practices of Spanish-speaking physicians times the total supply of Spanish-speaking physicians in the study counties. For example, a physician who reported that 20% of his/her practice consisted of Medicaid patients would constitute 0.2 Medicaid physician equivalents. We divided our calculated supply of Spanish-speaking physician equivalents by 100,000 Spanish-speaking LEP Medicaid beneficiaries. We repeated these ratios using the estimates of physicians seeing uninsured patients and the number of Spanish-speaking LEP uninsured patients. Data on language spoken by Medicaid beneficiaries were obtained from the California Department of Health Services’ Medicaid eligibility file for January 2001.22 Data on language of uninsured residents were obtained from the California Health Interview Survey 2001.23 The California physician survey research protocol was reviewed and approved by the UCSF Committee on Human Research.
Results
Among all physicians in the study counties, 26% of primary care and 22% of specialist physicians reported that they were fluent in Spanish. Spanish-speaking physicians in the study sample differed from non-Spanish-speaking physicians on several sociodemographic and practice characteristics (Table 1). Although there were no significant differences by age and gender, race/ethnicity was highly associated with Spanish fluency. Latino physicians reported the highest rate of speaking Spanish (93%). International medical graduates were more likely to report fluency in Spanish compared with US graduates (36% vs 25%). Although physicians who were not board-certified were more likely to speak Spanish, physicians did not report differences in Spanish fluency by practice setting.
Characteristics of Spanish-Speaking Physicians in Study Sample
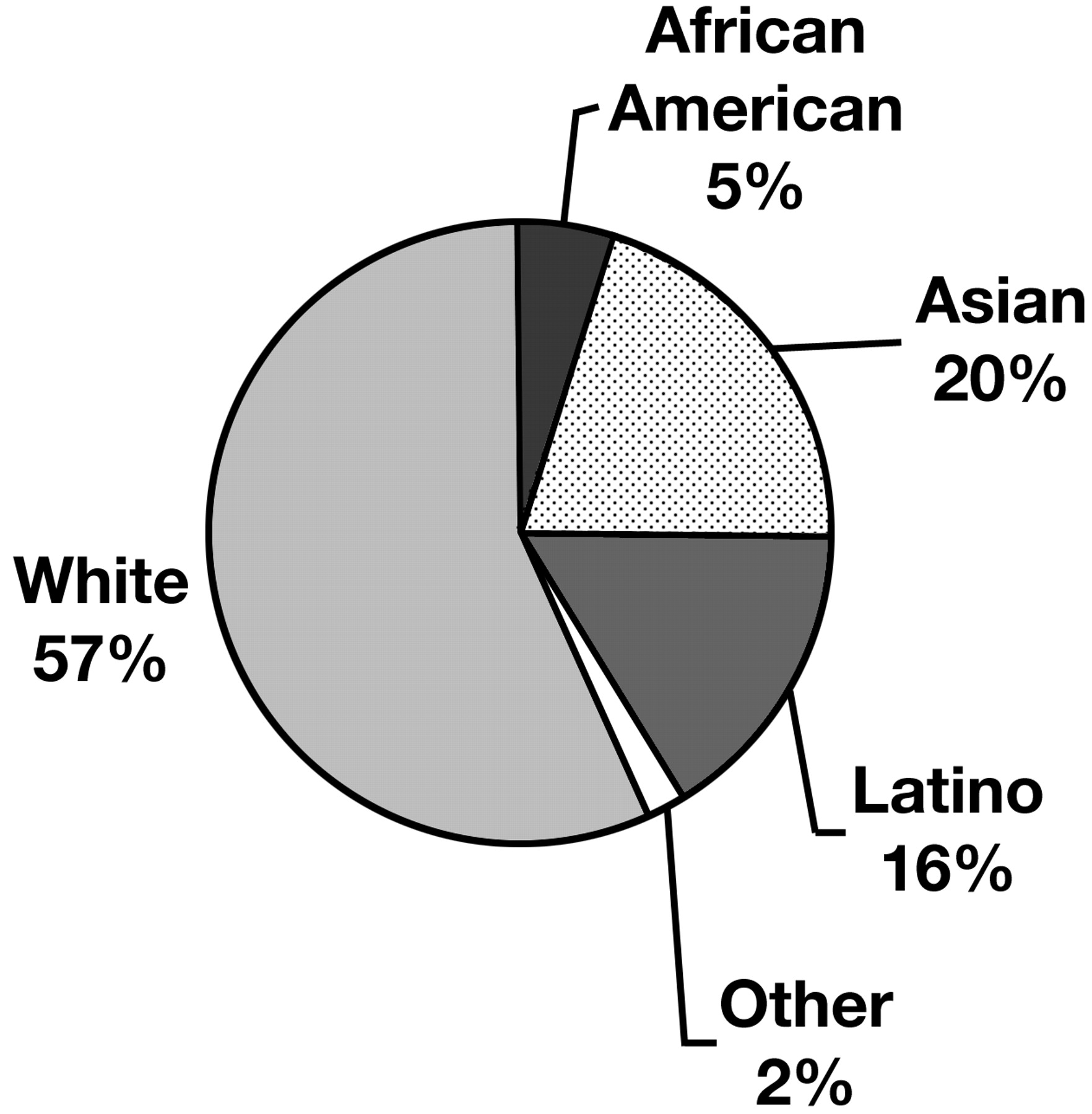
Weighting results to the total population of physicians in the study counties, we found that although almost all Latino physicians speak Spanish, Latino physicians comprise only 4% of the urban California workforce, and as a result only 16% of Spanish-speaking physicians are Latino (Figure 1). Likewise, international medical graduates make up 23% of the workforce and a slightly larger portion (28%) of Spanish-speaking physicians.

{kind=link}
Spanish-speaking physicians by race/ethnicity in 13 urban California counties, 2001.
In the 13 urban study counties, there were 146 primary care and 66 specialist physicians who spoke Spanish for every 100,000 Spanish-speaking LEP residents (Tables 2 and 3). The primary care physician ratio is substantially above a Council on Graduate Medical Education-defined standard of adequacy of 60 to 80 primary care physicians per 100,000 population.24 (No such standard exists for the subset of specialists included in the survey.)
Supply of Primary Care Physicians for All and Spanish-Speaking Patients in 13 Urban California Counties, 2001
Supply of Specialist Physicians for All and Spanish-Speaking Patients in 13 Urban California Counties, 2001
In communities in which Spanish-speaking primary care physicians practiced, on average, 15.3% of residents were LEP Spanish-speaking compared with 9.7% of residents where non-Spanish-speaking primary care physicians practiced (P < .05). Likewise, Spanish-speaking specialist physicians practiced in areas with more LEP Spanish-speaking residents than did non-Spanish-speaking specialist physicians (mean 12.9% vs. 9.2%; P < .05).
After controlling for the number of Spanish-speaking residents in the community, Spanish-speaking physicians were still found to have a disproportionately greater percentage of Latino and LEP patients in their practices. On average, physicians fluent in Spanish had 12% more Latino patients and 9% more LEP patients in their practice than other physicians after adjusting for the proportion of Spanish-speaking LEP residents in their community. Although Spanish-speaking physicians were slightly more likely to take Medicaid patients (60% vs 53%, P = .02), they were not more likely to take uninsured patients (47% vs 43%, P = .20).
Although Spanish-speaking physicians were more likely to care for Spanish-speaking patients, Medicaid coverage or lack of insurance seemed to impair access to these physicians for many Spanish-speaking LEP patients. In contrast to the general population, there were only 48 Spanish-speaking primary care and 29 specialist physician equivalents available for every 100,000 Spanish-speaking LEP patients on Medicaid. There were even fewer Spanish-speaking physician equivalents (34 primary care and 4 specialist) for every 100,000 uninsured Spanish-speaking LEP patients.
The supply of physicians fluent in Spanish for LEP Spanish-speaking Medicaid beneficiaries was substantially lower than the supply of Spanish-speaking physicians for Spanish-speaking LEP persons overall, because Spanish-speaking patients are over-represented in the Medicaid program, and many physicians either did not participate in Medicaid or did so at a low level. Spanish-speaking physicians, like all physicians, limit the number of their Medicaid patients: the mean percentage of Medicaid patients was 14% among all Spanish-speaking physicians’ practices. Physicians are even less likely to accept uninsured patients, and the mean percentage of uninsured patients for Spanish-speaking physicians was 3%. The restricted supply of Spanish-speaking physicians for Medicaid and uninsured patients speaking Spanish (48 and 34 primary care physicians per 100,000 patients, respectively) is similar to the supply of physicians for Medicaid and uninsured patients in the state regardless of language (46 and 15 primary care physicians per 100,000 patients, respectively).
Conclusion
A quarter of primary care physicians and a fifth of specialist physicians in urban areas of California report that they have the language skills to directly communicate with Spanish-speaking patients. Many non-Latino physicians report that they speak Spanish. These Spanish-speaking physicians practice in communities with a greater need for bilingual physicians, and they disproportionately serve many of the LEP and Latino patients in their communities. However, many Spanish-speaking physicians, like other physicians, accept few or no Medicaid and uninsured patients. Although the large number of Spanish-speaking physicians for the total population seems to be ample, the number of Spanish-speaking physicians for patients who are uninsured or on Medicaid is inadequate. As a result, it is the insurance status of LEP Spanish-speaking patients and not the supply of Spanish-speaking physicians, which limits their access to these physicians.
Study Limitations
Our study has several limitations. First, the results are based on self-rated language fluency of physicians. We did not validate the self-reports with formal testing of physicians’ medical Spanish skills, which might reveal a range of fluency in Spanish. However, some ability of physicians to speak Spanish with patients is likely to improve communication compared with physicians with no ability to speak Spanish.
Second, Spanish-speaking physician supply may not provide sufficiently detailed information on which to judge the availability of physicians with Spanish skills at the point of service for individual patients. Patients may experience barriers in access to Spanish-speaking physicians even when the supply of Spanish-speaking physicians is relatively high. Third, our study does not address the availability of bilingual providers for patients who speak neither English nor Spanish. The relatively high proportion of non-Latino physicians who are fluent in Spanish is not generalizable to other languages, such as Cantonese, Vietnamese, or Russian. Our findings should not be construed to indicate that language barriers are not a problem, especially for LEP patients with a primary language other than Spanish.
Finally, these data are limited to urban areas of California and the supply and skills of the physician workforce may not match the demand for linguistic services to the same degree in rural areas of California and other states. Nonetheless, we believe that our data are among the first to provide a population estimate of physicians’ Spanish skills; Spanish is the most prevalent language spoken by LEP patients in California.25 We believe our results also have implications for other states in that a national survey found that a higher proportion of Spanish-speaking patients who are uninsured compared with those who are insured did not have a regular doctor and experienced a language barrier with their physician.1
Implications
The high proportion of physicians who speak Spanish in California can potentially provide many LEP Spanish-speaking patients with access to health care that is not impeded by language barriers. Other studies have shown better communication, greater satisfaction, and improved outcomes for LEP patients who are treated by physicians speaking their native language.26,26a
Although almost all Latino physicians in California speak Spanish, Latino physicians comprise only 4% of all physicians and 16% of Spanish-speaking physicians in the state. This finding demonstrates the value of having a broad array of physicians, not simply those from any one particular ethnic group, educated to speak languages in addition to English. However, this finding does not mean that emphasizing bilingual capabilities for all physicians obviates the need to recruit more Latinos and other underrepresented minorities into the medical profession. Moreover, language fluency is only one element of cultural competence. Evidence suggests that Latino patients report greater satisfaction when treated by Latino physicians.27 Finally, other studies have shown that Latino physicians have a higher proportion of uninsured patients in their practices than non-Latino physicians, and minority physicians are more likely to practice in underserved areas and have minority patients28,29 contributing to better access to care for Medicaid and uninsured patients, irrespective of language proficiency.
IMG physicians are also more likely to speak Spanish, and previous reports show that they are more likely to participate in Medicaid and have a greater percentage of Medicaid patients in their practice.18 Recruiting physicians from Latin American countries may also help urban areas meet the demand for Spanish-speaking physicians.
Our findings are consistent with other studies, which have found that patients’ financial status is more influential than English proficiency in affecting access to physicians as measured by indicators such as having a usual source of care and the number of physician visits.30,31 Our results also suggest that type of insurance coverage, rather than limited English proficiency, is probably the single greatest barrier to physician services for Spanish-speaking LEP patients. Federal and state policies have recently been implemented to increase the availability of linguistic services for LEP patients and may help address one dimension of access to care for LEP patients. However, many LEP patients will continue to have difficulty accessing physicians as long as insurance barriers exist. States continue to struggle with low physician participation rates in Medicaid and growing numbers of the uninsured. Despite the push of Medicaid beneficiaries into managed care and increased Medicaid reimbursement rates in California, there has been no increase in physician participation rates in Medicaid in recent years.32 The national trend has also been toward declining physician participation in Medicaid.33 Latinos are the fastest growing minority group in the US and have the highest rates of uninsurance in the nation. Addressing health insurance related barriers to care for Medicaid beneficiaries and the uninsured is critical to improving health care for Spanish-speaking LEP patients.
Notes
Funding for the survey was provided by the California Health Care Foundation and the Health Resources and Services Administration’s Bureau of Health Professions.
Results of this study were presented at the Latino Coalition for a Healthy California Conference, August 2002.
- Received for publication November 13, 2003.
- Revision received November 13, 2003.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 26a.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.