Pneumothorax is defined clinically as an “accumulation of air or gas between the parietal and visceral pleurae,”1 and whereas it is often not a medical emergency, it can result in respiratory distress, tension pneumothorax, shock, circulatory collapse, and even death. Although there are many possible causes of dyspnea during a dental procedure, one rare complication is pneumothorax.
References in the dental literature frequently describe pneumomediastinum and subcutaneous emphysema as a complication of dental procedures,2–7 but little is to be found in either the dental or medical literature regarding passage of air causing pneumothoraces. A literature search using multiple medical search engines (MDConsult, Science Direct, Ovid, Expanded Academic ASAP, Wiley Interscience, EBSCO, Journals of the American Medical Association, and Academic Press Ideal) and the key words “pneumothorax or pneumomediastinum or subcutaneous emphysema and dental extraction” found 35 articles applicable to the case described. Only one cited pneumothorax as a complication.8 Most descriptions are in the dental literature. As a result, whereas physicians can be the first to assess a patient with acute onset of shortness of breath, they will most likely be unaware of this potential complication.
Dentists and physicians more often attribute the rapid onset of dyspnea in patients after a dental procedure to an anaphylactic reaction to the anesthesia used during the procedure. Although an anaphylactic reaction is often the case, it is important that physicians recognize the potential for a pneumothorax in a patient who has a patent airway and does not respond to treatment for anaphylaxis.
Case Report
A 21-year old man came to the emergency department complaining of pain on the left side of his face and radiating to the middle of his chest. Immediately before he arrived, the patient had undergone a lower molar extraction in which the dentist had used a high-speed air-turbine dental drill, along with positive pressure air, to aid in clearing the surgical field. Forty-five minutes after the procedure began, the patient complained to the dentist of some shortness of breath. The dentist discontinued the procedure and sent the patient to our emergency department. At the time of arrival, the dyspneic sensation had abated considerably. Despite no history of drug allergies, the patient was immediately given diphenhydramine (Benadryl) for a presumed anaphylactic reaction to lidocaine (Xylocaine) received at the dentist’s office. Epinephrine was not given at that time.
The patient’s blood pressure was 132/75 mm Hg, pulse 71 beats per minute, respirations 18/min, temperature 97.3°F, and oxygen saturation 99% on room air. When we examined him, we could visualize a patent airway and appropriate movement of the vocal cords. There was a slight fullness on the left side of the patient’s face but no erythema. We noted crepitation on the left side of the patient’s neck that extended bilaterally along the inferior aspect of the sternum and bilaterally on the superior submental and buccal areas of the jaw. The patient denied any tenderness with palpation of these areas. His lungs were clear to auscultation, and findings of the rest of the examination were unremarkable.
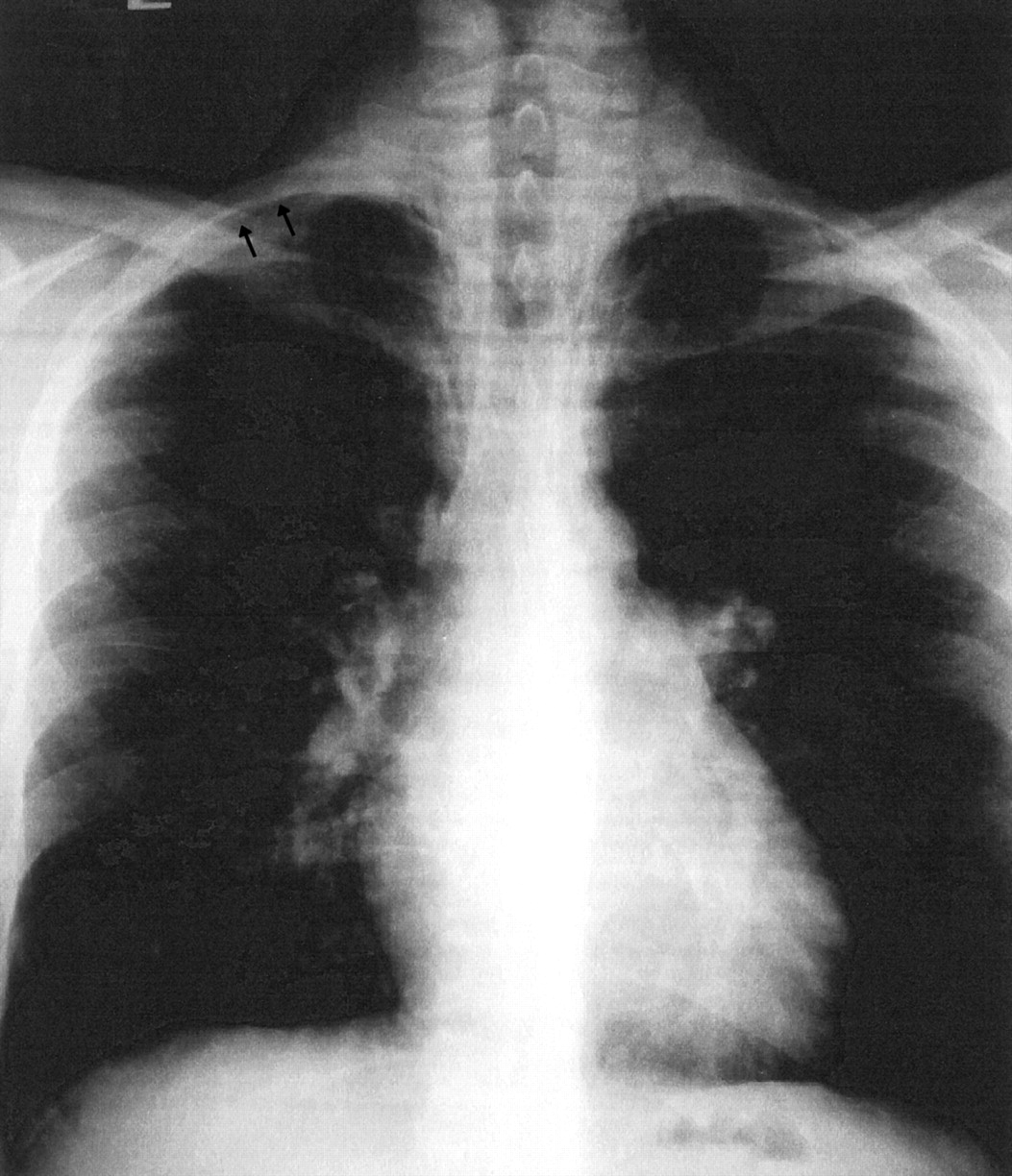
Radiographs of the neck and chest (Figure 1 and Figure 2) showed emphysema of the subcutaneous tissues of the face, retropharyngeal space, and mediastinum, as well as an apical pneumothorax on the right side.

Radiograph of patient’s neck. Note the prominent opacities in the subcutaneous tissue consistent with air filling the potential spaces of the fascial planes of the neck.

Radiograph of patient’s chest. The line noted with black arrows represents a pneumothorax induced by pressured air passing through the fascial planes of the neck into the thorax.
The patient was admitted to the hospital so he could be monitored for any progression of the pneumothorax and concomitant symptoms. Because of possible infection of the potential spaces, he began a course of 875/125 mg of amoxicillin-clavulanate (Augmentin) twice daily for 10 days. The patient remained afebrile and had a normal white cell count throughout his hospitalization. On hospital day 2, the patient noted some pain with deep inspiration, which resolved by day 3. His hospital course was otherwise unremarkable. Daily chest and neck films showed gradual resolution of the emphysema and pneumothorax. The patient was discharged on day 3 and completed the 10-day antibiotic course as an outpatient. A follow-up chest radiograph to assess the status of the pneumothorax 6 weeks later showed complete resolution of his emphysema and pneumothorax. Clinically he was asymptomatic at his follow-up examination.
Discussion
Subcutaneous emphysema, pneumomediastinum, pneumopericardium, and pneumothorax can occur as the result of several invasive dental procedures.9 Turnbull10 first described barotrauma associated with a dental procedure in the early 20th century. He referred to a case in which a bugler, shortly after a tooth extraction, developed subcutaneous emphysema of his face and head as a result of the Valsalva maneuver while playing his instrument.
Modern dentistry has incorporated tools that further the risk of barotrauma. High-speed air-driven drills have been in use for routine dental procedures since the 1960s. Ideally, a drill should be positioned so that the air is directed away from the surgical field; however, many dentists use drills that have an air-and-water-cooled burr. The resulting dispersion can direct some of the air and water directly into the wound and into the potential spaces of the neck.8,11,12
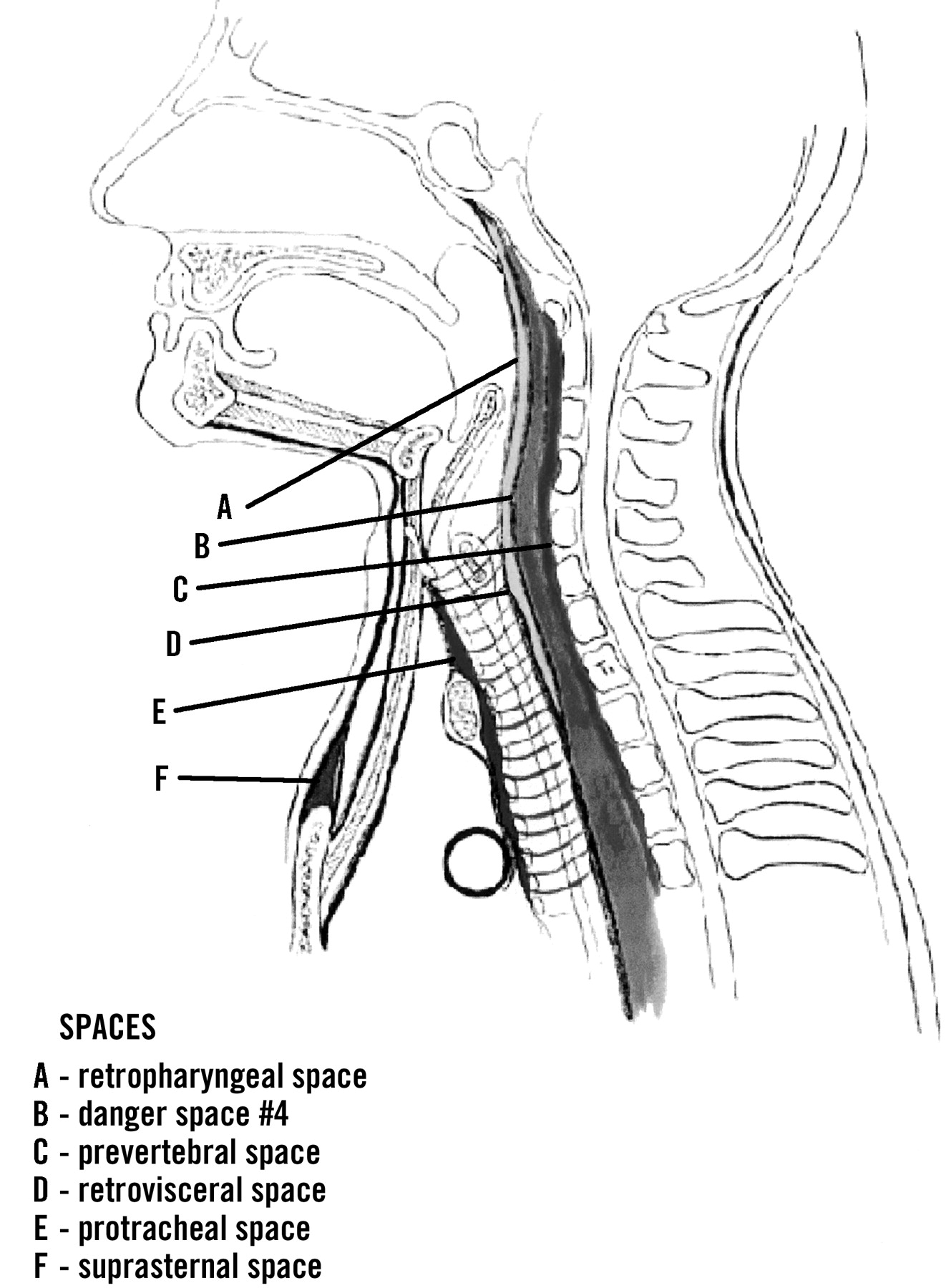
This flow into the subcutaneous tissue initiates the opening of potential spaces and can result in the aforementioned complications. An understanding of facial and neck anatomy is essential to recognize the pathway air takes when a pneumothorax occurs. The base of the first, second, and third molar roots communicates directly with the sublingual and submandibular spaces. These spaces communicate with the pterygomandibular, parapharyngeal and retropharyngeal spaces (Figure 3). It is through the retropharyngeal space that air can pass to the mediastinum and the pleural space. Air passing into the mediastinum and pleural space is most commonly associated with extraction of the third molar.13

{kind=link}
{kind=link}
{kind=link}
Illustration of spaces of head and neck. Reproduced with the permission of Dr. Walid El-Bermani, MD, PhD, of the Department of Clinical Anatomy, Tufts Medical School.
In the case described, air could have spread to the thoracic cavity in two ways. First, accumulation of air in the retropharyngeal space can come from the submaxillary space found under the mandible. This area directly communicates with the lateral pharyngeal space, which is contiguous with the retropharyngeal. Second, air can pass from the superficial deep investing fascia to superficial fascia, allowing direct spread to the third intercostal space, where it can pass into the pleural space. By either route, compromise of pulmonary function ensues.
In addition to pneumothorax, air passing through the potential spaces of the neck has been implicated in complications ranging from otalgia, eustachian tube dysfunction and temporary hearing loss,14 dysphagia and dysphonia,15 pneumoperitoneum and pneumopericardium9 to pneumoparotid16; even air emboli have been reported.17
Barotrauma has resulted from a number of other unusual events: use of hydrogen peroxide as an antiseptic in the oral area,18 cocaine or other drug use, status asthmaticus, arthroscopy, scuba diving, adenotonsillectomy, spirometry, gastrointestinal instrumentation, and even secondary to increased intrathoracic pressure, as with a Valsalva maneuver (eg, labor).19,20 Coughing spasms, sneezing, and vomiting have also been shown to cause ascending barotraumas associated with rupture of alveolar membranes21; the increased intraoral pressure in an person with exposed gingival spaces would be at similar risk for a descending interruption. Although no studies have clearly ascertained a relation between barotrauma and dental procedures, the disruption of normal anatomic barriers to the underlying fascial planes as a result of dental procedures can place patients at increased risk for barotrauma.
Infections can also arise when these fascial planes are exposed, so that evaluation for infection and treatment with antibiotics might be necessary.22 Ludwig’s angina is a particularly serious infectious complication that arises from bacterial spread through these fascial planes.23 Oxygen supplementation has been shown to hasten the resolution of the emphysema; it replaces air in the potential spaces and is more readily reabsorbed into the surrounding tissues.24 Otherwise, treatment is mainly supportive, and the condition is typically self-limiting.
Although dental and periodontal procedures seem routine in clinical practice today, they are not without their systemic complications. Air-powered drills or other pressurized appliances used during dental procedures can introduce air into the potential spaces of the neck and thorax. Communication of these spaces to the pleura can result in pneumothoraces, which can be life-threatening. Fortunately, in the case described, the patient developed no life-threatening complications. His case, however, illustrates anatomically how air or other materials, including pathogens, can pass relatively easily from the oral cavity, aided by the air pressure of a dental drill, into the fascial planes and into the thorax.
Diagnosis can be made by a thorough examination, focusing on overlying tissue and the pulmonary system, as well as radiographs to disclose the barotrauma. Management should focus initially on acute stabilization if the patient shows any signs of pulmonary compromise. Assessment for possible infection should be undertaken, and empiric antibiotic therapy for typical oral pathogens can decrease risk of life-threatening complications associated with infectious spread in the fascial planes. Finally, regular assessment for resolution of emphysematous findings, as well as clinical symptoms, can confirm successful treatment and reduce the risk of untoward complications. When assessing such a patient, physicians should be aware that dyspnea can be caused by an anaphylactic reaction, but they should also consider anatomic impairment of breathing as a result of mass effect. As in this case, when a patient has acute shortness of breath during or immediately after a dental procedure, primary care physicians should consider the potential for such barotraumas in addition to other possible conditions.
Notes
No outside sources were solicited or used for funding of this paper. The opinions and assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of the Army Medical Department or the Army Service at large.
- Received for publication November 1, 2002.
- Revision received November 1, 2002.