
Abstract
Introduction: Spondylolysis and isthmic spondylolisthesis are commonly implicated as organic causes of low back pain in this population. Many patients involved in sports that require repetitive hyperextension of the lumbar spine like diving, weightlifting, gymnastics and wrestling develop spondylolysis and isthmic spondylolisthesis. While patients are typically asymptomatic in mild forms, the hallmark of symptoms in more advanced disease include low back pain, radiculopathy, postural changes and rarely, neurologic deficits.
Methods: We conducted a narrative review of the literature on the clinical presentation, diagnosis, prognosis and management of spondylolysis and isthmic spondylolisthesis.
Results: A comprehensive physical exam and subsequent imaging including radiographs, CT and MRI play a role in the diagnosis of this disease process. While the majority of patients improve with conservative management, others require operative management due to persistent symptoms.
Conclusion: Due to the risk of disease progression, referral to a spine surgeon is recommended for any patient suspected of having these conditions. This review provides information and guidelines for practitioners to promote an actionable awareness of spondylolysis and isthmic spondylolisthesis.
Introduction
The prevalence of back pain in adolescents has steadily increased over the past decade, with an annual incidence ranging from 11.8% to 33%.1,2 Spondylolysis and isthmic spondylolisthesis are commonly implicated as organic causes of low back pain in adolescents and may go unrecognized until symptoms develop into adulthood.1,3 Spondylolysis is the term used to describe an anatomic defect of the pars interarticularis, which typically results from stress reaction and subsequent fracture as a result of repetitive loading of the lumbar spine in extension and rotation.4⇓⇓–7 In the setting of bilateral pars interarticularis defects, forward translation of 1 vertebra relative to the next caudal vertebral segment may occur, which is termed isthmic spondylolisthesis4⇓⇓⇓–8 Consequently, spondylolysis and isthmic spondylolisthesis may be considered a continuum of the same disease process.7,9 Estimates for the prevalence of spondylolysis (5% to 11.5%) and isthmic spondylolisthesis (4% to 8%) at adulthood are similar in range.1,3⇓⇓–6,10,11 And while the majority of patients improve with conservative therapy including activity restriction, physical therapy and bracing, others require operative intervention due to persistent symptoms.1,3 Appropriate clinical workup of these pathologies is imperative as it leads to earlier diagnosis and management. Physicians should remain informed regarding when to expect and how to appropriately manage these conditions in the pediatric or young adult patient presenting with back pain.
Classification
The etiologies of spondylolisthesis were initially described by Wiltse et al., and then later modified by Marchetti et al.11,12 The Wiltse-Newman classification categorizes spondylolisthesis under broad etiologies which include isthmic, dysplastic, degenerative, post-traumatic and pathologic.11 In contrast, the Marchetti-Bartolozzi classification distinguishes developmental, which includes dysplastic, from acquired etiologies, which includes isthmic, traumatic, degenerative and pathologic.11,12 The primary focus of this article is spondylolysis, as well as isthmic spondylolisthesis, as these pathologies are much more commonly implicated in the young adult population presenting with back pain to their primary care physician.
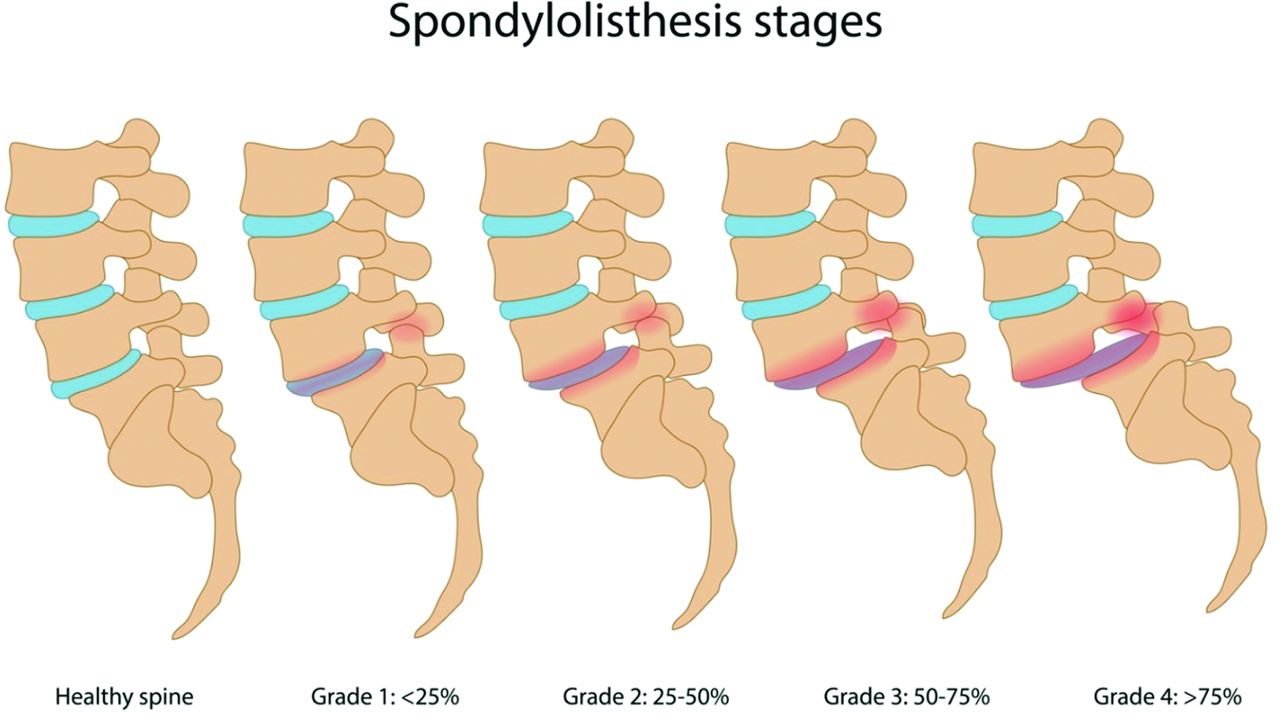
In addition, the Meyerding classification is frequently used to grade the severity of the “slip” or forward translation of the vertebra relative to the next caudal vertebral segment.13 The slip grade is particularly relevant as it provides prognostic information and can influence subsequent management in these patients (see Figure 1).13

The severity of spondylolisthesis according to the Meyerding classification system divides slip severity into 5 grades: 0% to 25% is Grade I, 25% to 50% is Grade II, 50% to 75% is Grade III, 75% to 100% is Grade IV, and greater than 100% is Grade V, which is referred to as spondyloptosis. Reproduced with permission from OrthoInfo. © American Academy of Orthopaedic Surgeons. https://www.orthoinfo.org/.
Pathophysiology and Natural History
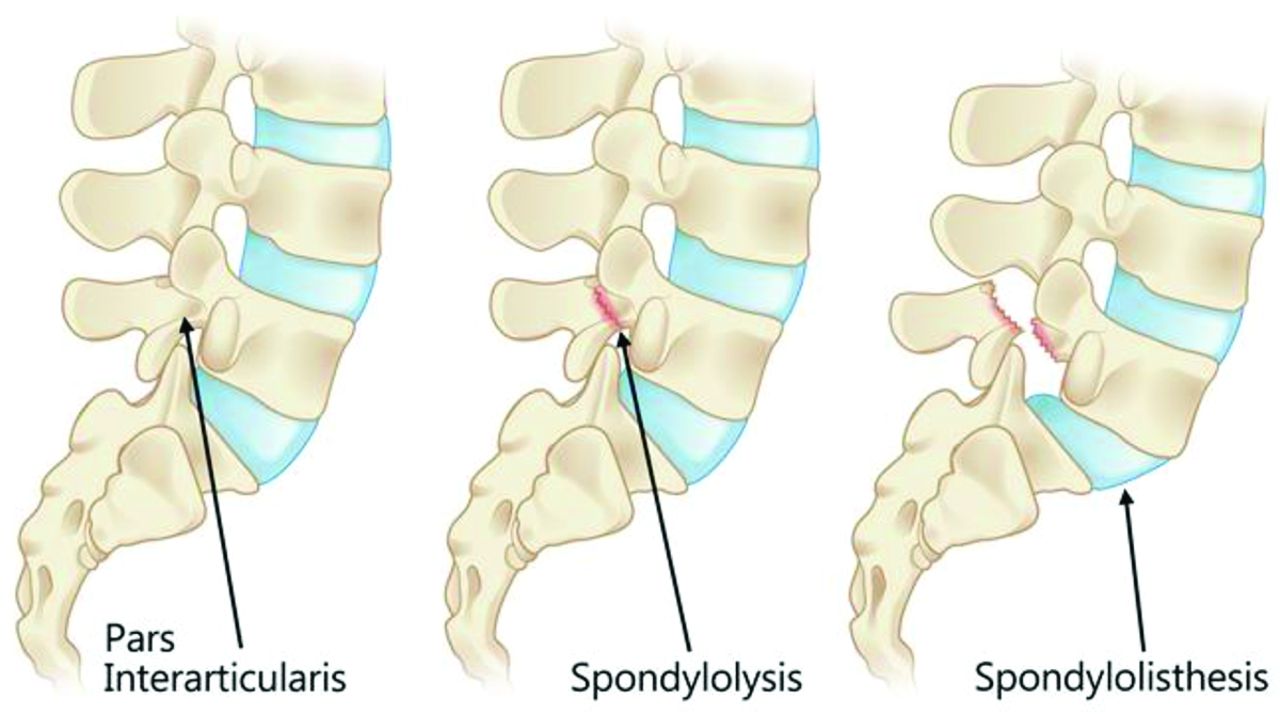
Spondylolysis is an anatomic defect of the pars interarticularis, which initially begins as a stress reaction.4⇓⇓–7 This stress reaction represents increased bony edema and microtrauma, resulting in an inflammatory, osseous healing response of the pars without a radiographically apparent fracture.14 However, following increased stress on the lumbosacral spine, spondylolysis may develop as a distinct fracture propagates through the pars.15,16 Morita et al. described this process in 3 distinct phases.16 In the early stage, there is a nondisplaced, acute fracture line. At the progressive stage, a bone gap may be evident as the fracture can become mildly displaced with some evidence of healing. Finally, at the terminal stage, there is evidence of pseudoarthrosis and sclerosis at the site of the defect.16 These distinct stages are important as they provide implications with healing potential.16,17 For instance, with conservative management, the healing rate of early-stage spondylolysis is 73 to 87%. This contrasts sharply with the progressive and terminal stages, which has healing rates of 38 to 60% and 0%, respectively.16⇓–18 Isthmic spondylolisthesis, where forward translation of 1 vertebra relative to the next caudal vertebral segment occurs, can be considered a progression from spondylolysis (see Figure 2).4⇓⇓⇓–8 As the pars fracture loses continuity, all structural support between the anterior and posterior spinal elements is lost and the vertebral body is able to subluxate anteriorly under normal physiologic loads.4⇓–6 This phenomenon only occurs in the setting of bilateral spondylolysis as the mechanical stability from a unilaterally intact pars prevents slippage.6 In a long-term study of 500 patients, Beutler et al. noted that 62.5% of patients with bilateral spondylolysis had some degree of spondylolisthesis on presentation. At 45-year follow-up, the incidence of spondylolisthesis increased to 81.2%. Whereas a younger age on presentation with spondylolysis was associated with increased risk of progression to spondylolisthesis, the incidence decreased with each passing decade: 7% in the first decade, 4% in the second and third decade, and 2% in the fourth decade.6

The pars interarticularis (left) refers to the small segment of bone that joins the facet joints in the spine. Spondylolysis (center) occurs via a stress fracture and subsequent fracture of the pars interarticularis. In the setting of bilateral pars defects, forward translation of the caudal vertebral segment may result, termed isthmic spondylolisthesis (right). Reproduced with permission from OrthoInfo. © American Academy of Orthopaedic Surgeons. https://www.orthoinfo.org/.
Several factors are thought to contribute to the development of spondylolysis and spondylolisthesis.19⇓–21 A genetic component is a significant factor that has been implicated in the pathogenesis of this disease. For instance, spondylolysis has been linked to particular familial distributions and also correlates with the occurrence of spina bifida, a condition that is also strongly linked to a genetic predisposition.19 Similarly, spondylolisthesis has a strong genetic link, as it is 5 times more likely in patients with first-degree relatives with the same condition.20,21
In addition, mechanical factors are perhaps the most apparent contributing factor. As this pathology has not been described in newborns or nonambulators, like patients with cerebral palsy, bipedial ambulation and upright posture likely play a significant role.11,19,22 To stand erect for bipedal ambulation, lumbar lordosis is inherently increased. This in turn increases the strain on the pars interarticularis in the lumbar spine and predisposes to fracture development as distraction forces are applied anteriorly and compressive forces posteriorly.20 As forces are applied anteriorly, fracture propagation in the pars interarticularis occurs in a predictable inferior to superior fashion. In contrast, as reactive compressive forces are applied posteriorly, cortical contact promotes healing in a characteristic superior to inferior pattern.18 As a result, spondylolysis is best described as a fatigue fracture of the pars interarticularis from chronic, repetitive stresses placed on the lumbar spine.19
The mechanical contribution of spondylolysis is best exemplified in athletes. High levels of physical activity have been strongly associated with this condition as the aforementioned forces are increased on the pars interarticularis during strenuous exercise.19,23 Higher rates of spondylolysis have been reported in young athletes (11%) compared with nonathletes (3%).24 Up to 47% of athletes aged 12 to 18 with atraumatic back pain presented with spondylolysis, with similar incidence rates of spondylolisthesis also reported (47.45%).25,26 Furthermore, the incidence of spondylolysis in athletes also seems to be sport specific as well, as higher rates of incidences have been reported in activities that require hyperextension of the lumbar spine including diving, weight-lifting, rowing, gymnastics, and wrestling (see Figure 3).19,23

A young gymnast performing a back-bend position requiring hyperextension of the lumbar spine. Such repetitive maneuvers place stress on the pars interarticularis and predispose patients to develop spondylolysis and subsequent isthimic spondylolisthesis. Reproduced from Sands WA, McNeal JR, Penitente Get al Stretching the Spines of Gymnasts: A Review. Sports Med. 2016;46(3):315 to 327.
Once spondylolisthesis has occurred, the risk of further slippage is multifactorial. Female gender and remaining growth potential are commonly reported risk factors.6⇓–8,17,27,28 As such, peak rate of progression of spondylolisthesis seems to closely align with peak growth velocity during puberty.19 However, pronounced lumbosacral kyphosis and the presence of a high-grade spondylolisthesis on initial radiographic evaluation are the most predictive factors for further progression.19,27,31,29,30
Signs, Symptoms, and Diagnosis
Not all patients with spondylolysis and isthmic spondylolisthesis will go on to develop symptoms, and though pars interarticularis defects may be discovered in the diagnostic work-up of back pain, it must not be assumed to be causative.6,10 The stage of spondylolysis or the grade of spondylolisthesis on presentation largely determines whether patients become symptomatic.10 For instance, early stage spondylolysis often remains asymptomatic and is considered an incidental radiographic finding.32 Similarly, low-grade spondylolisthesis (Grade I and II) does not typically manifest in severe symptoms.6,33⇓–35 However, in high-grade spondylolisthesis (Grade III and IV), patients report a marked increase in symptoms with 55% to 91% reporting back pain, 44 to 55% reporting radicular symptoms and 50% reporting restrictions in activity.33,36 Pain tends to be worse with extension, which loads the posterior spinal elements, especially the pars.1,35,37 In isthmic spondylolisthesis, symptoms may be precipitated by sagittal imbalance leading to muscle pain in the lower back.38 Radiculopathy in spondylolysis and isthmic spondylolisthesis can be attributed to instability or disk pathology, which may lead to L5/S1 foraminal stenosis leading to compression of the exiting L5 nerve root or tension of the traversing S1 nerve root.36,39,40
When assessing a patient with a pars interarticularis defect, a thorough physical and neurological examination are essential to rule out concomitant pathology.1 Spondylolysis and isthmic spondylolisthesis rarely cause neurological deficits at initial presentation. Low-grade disease can present with lumbar tenderness to palpation along with limited and painful lumbar extension.36 High-grade disease can present with a palpable step-off and alterations in posture due to the anterior and inferior translation of the torso, including hamstring tightness and a crouch gait.1,4 The 1-legged hyperextension or “stork test,” is a described examination maneuver where the patient is asked to stand on 1 leg while the clinician passively hyperextends the spine, reproducing the patient’s pain.41–42 However, recent studies have questioned the diagnostic utility of this test in spondylolysis and isthmic spondylolisthesis, noting low sensitivities (50% to 73%) and specificities (17% to 32%).41–42
As back pain is becoming an increasingly common reason for visits to musculoskeletal care providers, a comprehensive initial differential diagnosis should be kept in mind.1 Other organic pathologies including Scheuermann kyphosis, overuse syndromes, disk herniations, spondylodiscitis or neoplasm should also be considered, and missing or delaying such diagnoses has its own implications.1,10 Spondylodiscitis typically presents with fevers, pain with motion and elevated serum inflammatory markers.1 Neoplasm classically presents with pain at night and constitutional symptoms such as weight loss, night sweats or fatigue. In the setting of acute radiculopathy, lumbar disk herniation should be considered, especially following a trauma.1
Radiographic Evaluation
Plain radiographs and advanced imaging have a role in the diagnosis and management of spondylolysis and isthmic spondylolisthesis. However, plain radiographs are the first and most important step in the evaluation of any patient with low back pain. Standing AP and lateral radiographs of the entire spine are indicated in the setting of localized pain, a clinical deformity or red flag symptoms (night pain, fevers, unintentional weight loss or neurologic deficits).1 In addition, radiographs are indicated in the setting of persistent low back pain for greater than 4 weeks in children/adolescents and 6 weeks in adults.1
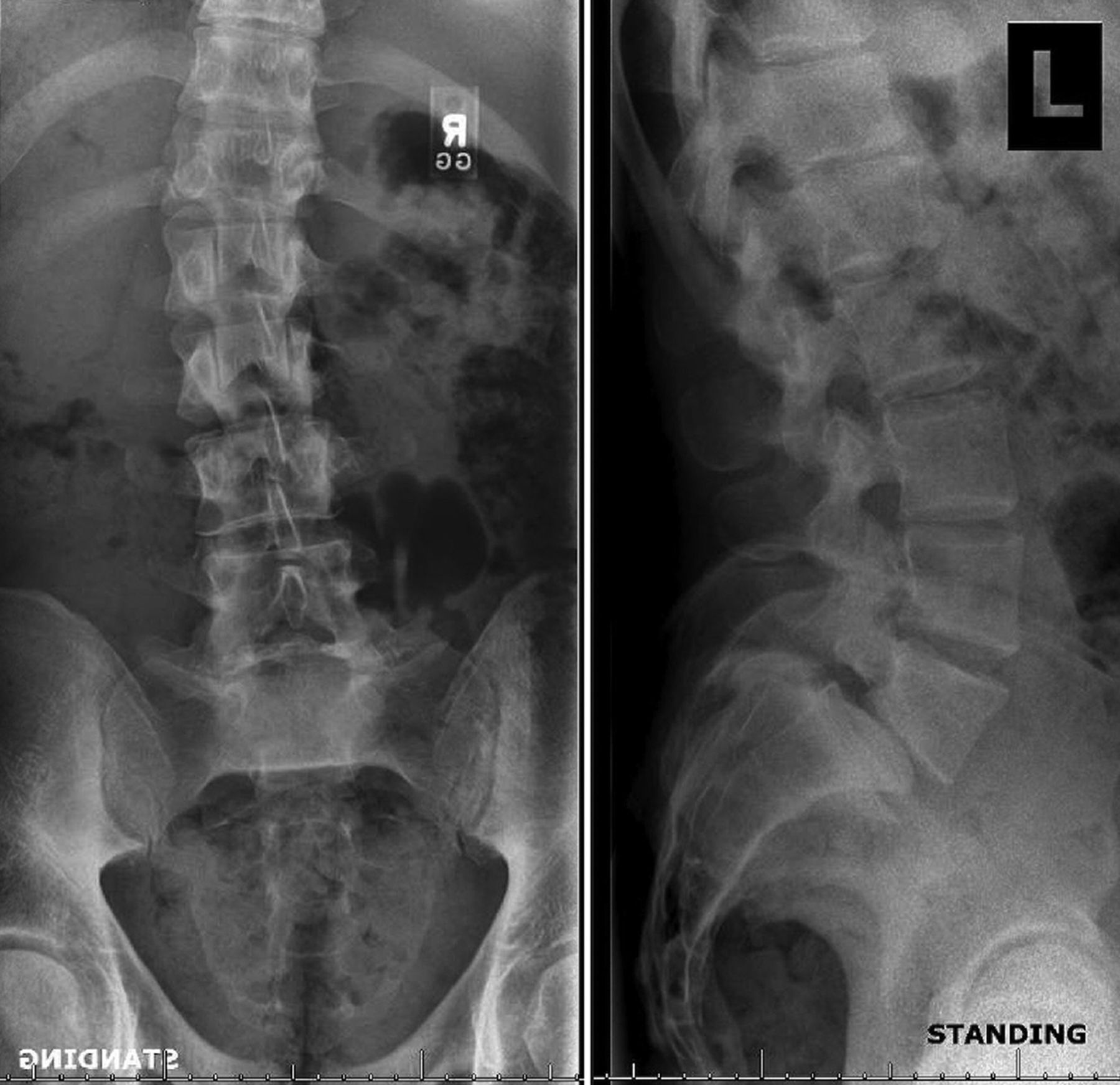
In spondylolysis and isthmic spondylolisthesis, standing AP and lateral radiographs of the lumbosacral spine are likely to reveal cortical defects at the L5 pars interarticularis (see Figure 4), with or without anterolisthesis. Oblique radiographs have historically been touted as more sensitive than AP and lateral radiographs; however, more recent data suggest that the inclusion of oblique views increases cost and radiation without affecting diagnostic sensitivity or specificity.43–44 During preoperative planning, the L5/S1 level can be assessed with a Ferguson view, which directs the beam parallel to the L5/S1 joint space, approximately 30 to 35 degrees cephalad to the vertical.45

AP and Lateral standing radiographs of a skeletally mature young athlete demonstrating L5-S1 Meyerding Grade II isthmic spondylolisthesis. Significant disk space collapse corresponds with long-standing low back pain; this patient also presented with L5 radiculopathy due to resultant foraminal stenosis. In addition present on the AP film is a minor thoracolumbar scoliosis which is likely incidental and unrelated to the aforementioned pathology.
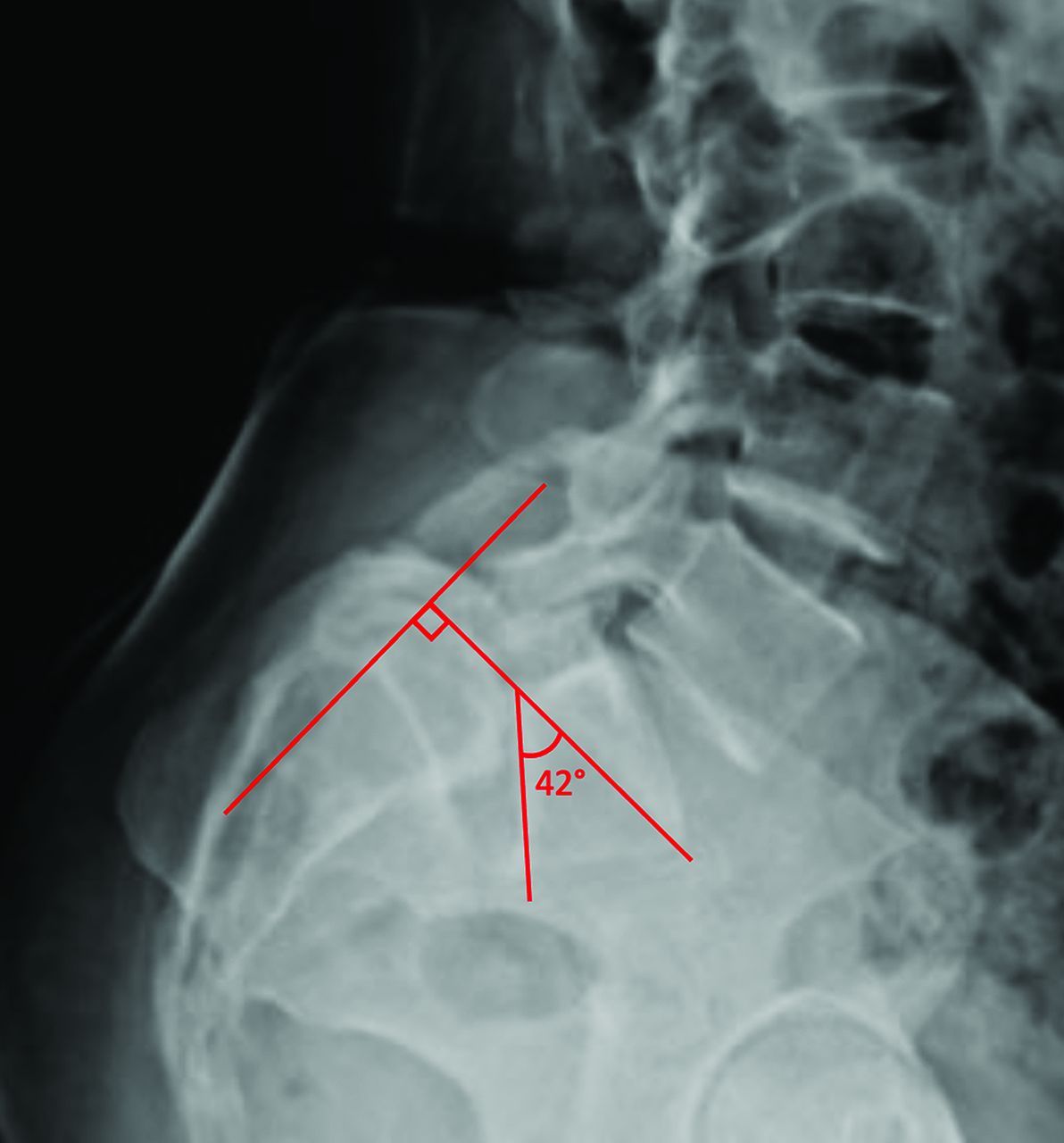
There are several measurements that can be made based on plain radiography that have variable predictive and prognostic value. The slip angle is the angle between the superior endplate of the S1 vertebral body and the inferior endplate of the L5 vertebral body. If the superior endplate of S1 is deformed due to sacral doming, which is seen in this pathology due to mechanical stress on the anterior sacrum, the angle can be measured between a line perpendicular to the posterior sacrum and a line along the inferior endplate of L1 (see Figure 5).45 A slip angle of greater than 50 degrees is predictive of further slip progression.7,46 The lumbosacral angle is the angle between the posterior sacrum and the superior endplate of the L1 vertebral body.29 A lumbosacral angle less than 100 degrees is associated with an increased risk of cosmetic and functional disability. In addition, lumbosacral angle is the most reliable method for determining the degree of lumbosacral kyphosis.29
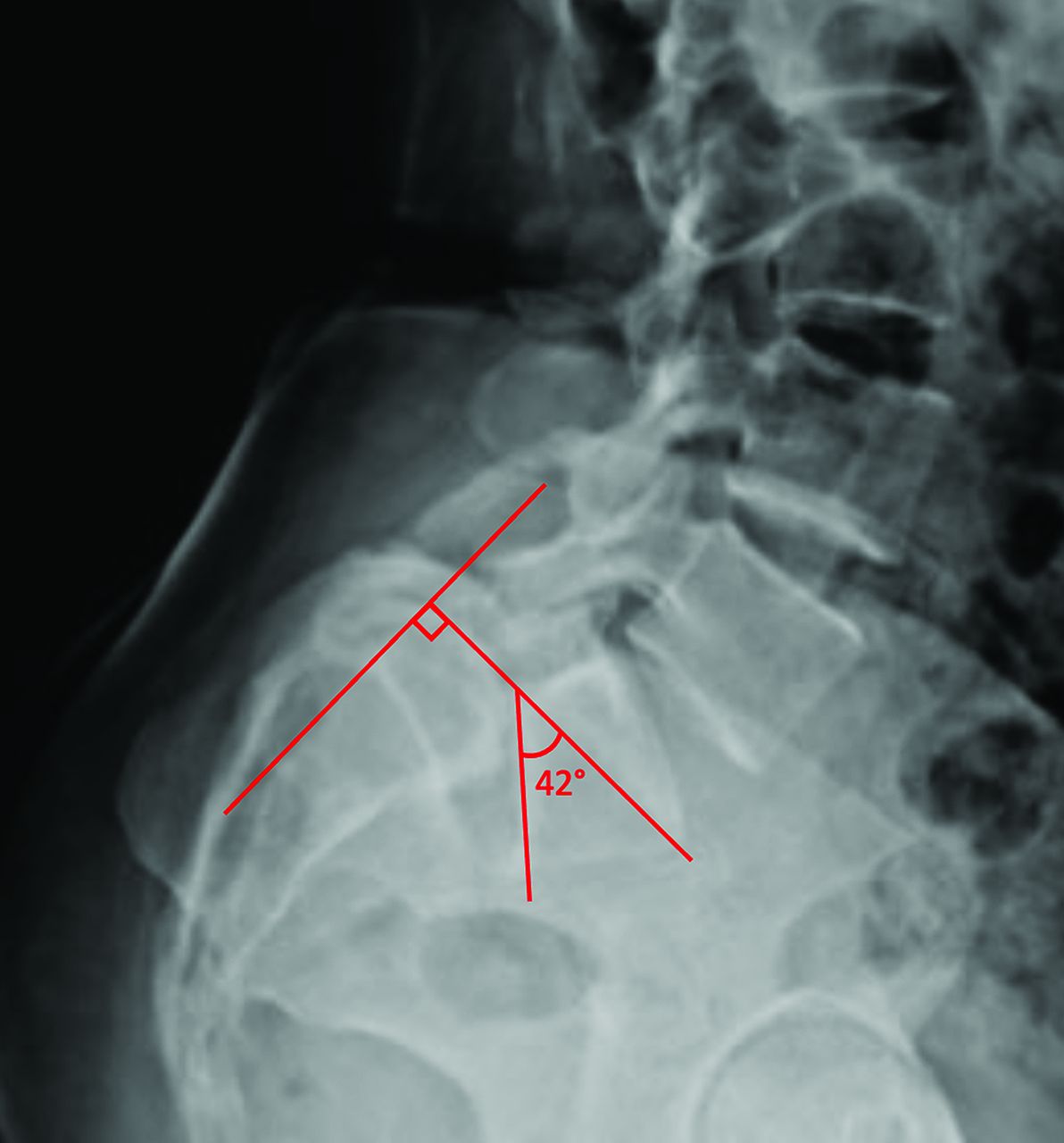
Lateral radiograph evaluating the slip angle of a patient with high-grade spondylolisthesis. A slip angle greater than 50 degrees is predictive of further slip progression
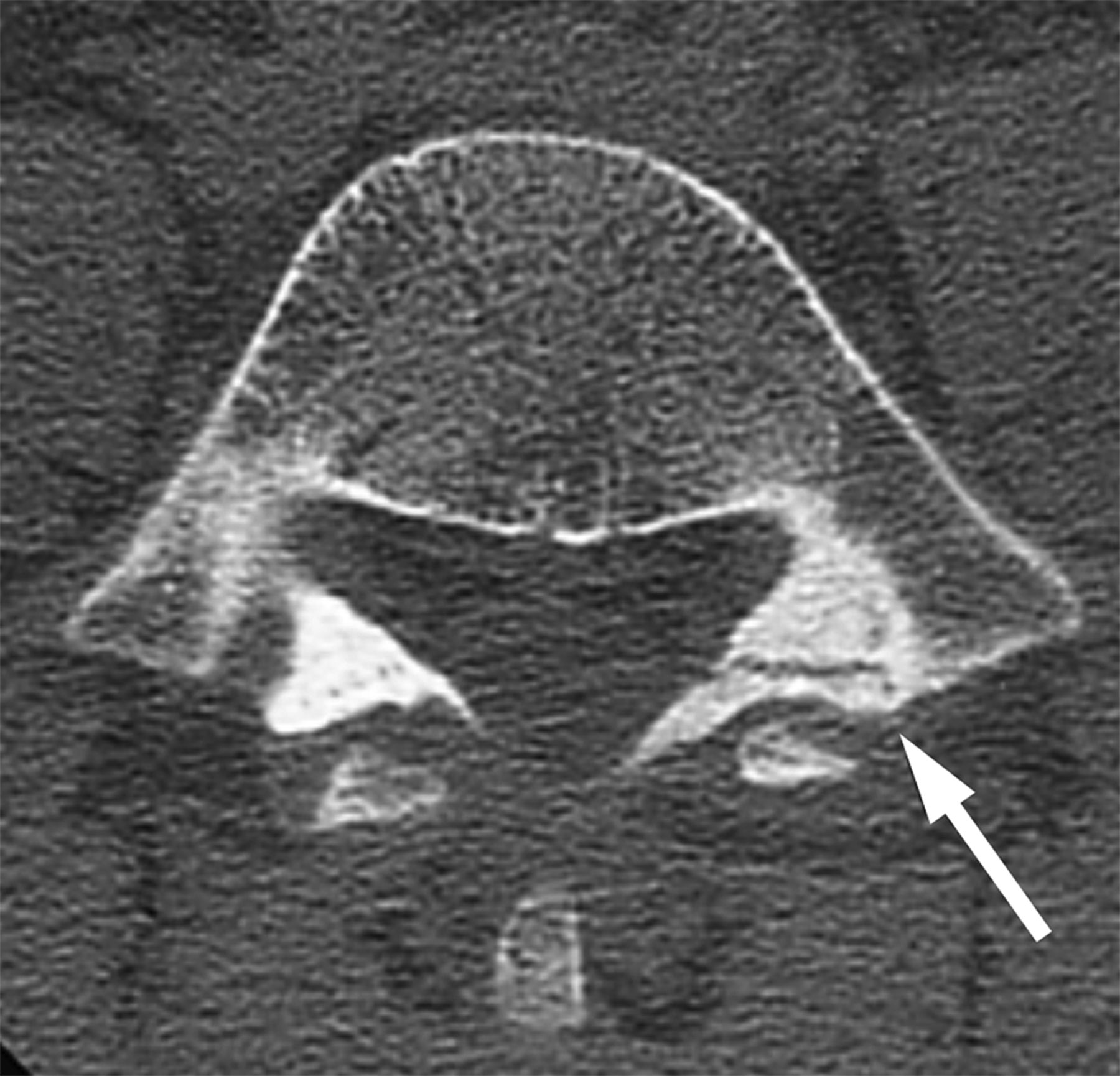
Single-photon emission CT (SPECT) of the lumbosacral spine is the most effective method for detecting spondylolysis when plain radiographs are normal. As increased uptake in the pars is indicative of a stress reaction, decreased uptake on serial SPECT scans has been correlated with improved clinical symptoms.4 Thin-section CT scans are the best modality at defining bony anatomy in spondylolysis and isthmic spondylolisthesis (see Figure 6).47⇓–49 Similarly to SPECT scans, thin-section CT can help confirm progressive healing of pars defects by delineating the degree of cortical disruption, lysis and sclerosis.4,47⇓–49 Improved 3-dimensional CT reconstructions of the lumbosacral spine in the setting of isthmic spondylolisthesis is also useful in preoperative planning.4

An axial CT scan image demonstrating spondylolysis. The image highlights the cortical disruption and surrounding sclerosis at the area of the pars defect.
While T2-weighted MRI may reveal edema of the pars bone marrow on pars stress reactions, there is generally no role for MRI in diagnosing spondylolysis and isthmic spondylolisthesis.50 The exception where MRIs may be a useful adjunct is in the rare setting of neurologic signs or symptoms. However, unlike degenerative spondylolisthesis where central stenosis leading to neurogenic claudication is a common finding, isthmic spondylolisthesis characteristically leads to an abnormal increase in canal diameter (“wide canal sign”).51 Radiculopathy, when present, typically involves the L5 nerve root due to lumbar instability or disk pathology causing L5/S1 foraminal stenosis.36,39,40 Spinal cord anomalies, infection and neoplasm are other sources of low back pain that are best assessed with MRI.4
Management
If the diagnosis of spondylolysis or spondylolisthesis is unclear, or once a diagnosis is made, referral to an experienced spine care provider is advisable. Management decisions are often guided by multiple factors. Both pathologies are generally considered nonsurgical diseases, as young adults with spondylolysis and low-grade spondylolisthesis are able to return to pain-free, unrestricted activities approximately 85% of the time.3,5 However, to date, there have been no high-level studies comparing long-term outcomes in operative versus nonoperative management in either disease.
Nonoperative
Conservative management options in spondylolysis and low-grade spondylolisthesis are intended to alleviate pain, promote osseous healing of the pars defect, if possible, and prevent progression of the slip, if present.4,5,16,52 As the healing potential is significantly greater in unilateral than bilateral lesions, prompt treatment from an early diagnosis of spondylolysis may improve the overall clinical outcome.4,52 Furthermore, other causes of pain must always be considered as many radiographic pars lesions are asymptomatic, and require no intervention or activity restrictions.53
While there are limited direct comparison studies between various nonoperative treatment modalities, for symptomatic cases, management for both spondylolysis and low-grade spondylolisthesis typically begins with a period of strict avoidance of aggravating activities and lumbar flexion-based physical therapy.4,5,52,53
This typically demands abstinence from sport in a young athlete, particularly those involved in extension-based activities including gymnastics, football, soccer and others.54 Physical therapy emphasizes spine stabilization through stretching of the hip flexors, hamstrings and strengthening of the deep abdominal muscles and lumbar multifidus over a pain-free range of motion arc.4,55 Lastly, bracing immobilization via a thoracic lumbar sacral orthosis (TLSO) is often used as an adjunct to reduce pain and limit spine mobilization.4,19,55⇓–57 Despite widespread current use, Klein et al. performed a meta-analysis of observational studies assessing nonoperative management modalities and found no statistically significant difference in success rates between those treated with a brace (89.0% in 334 patients) and those without (86% in 137 patients).5 The authors’ protocol typically reserves a short period of bracing for 6 to 8 weeks in patients who do not initially respond to rest and physical therapy. Other modalities including heat, traction, massage therapy, acupuncture and chiropractic manipulation may have therapeutic effect though have not demonstrated efficacy supported by high-quality literature.58,59
Optimal management for high-grade spondylolisthesis, including the precise role of nonoperative management, remains controversial. While others have advocated for routine surgery in high-grade cases, Lundine et al. performed a recent retrospective review of 53 patients with high-grade spondylolisthesis and noted that in asymptomatic patients, observation alone did not lead to significant problems at follow-up.60 In addition, delayed surgical intervention did not result in worse clinical outcomes. While patients with a more kyphotic slip angle tend to have a poorer prognosis, no clear radiographic threshold exists to dictate management.60,61 Similarly to spondylolysis and low-grade spondylolisthesis, nonoperative management includes activity restriction, physical therapy and bracing.60⇓⇓–63 The authors treatment decisions in high-grade spondylolisthesis are principally guided by patient symptomatology with an initial trial of conservative modalities before considering surgery in most cases.
Operative
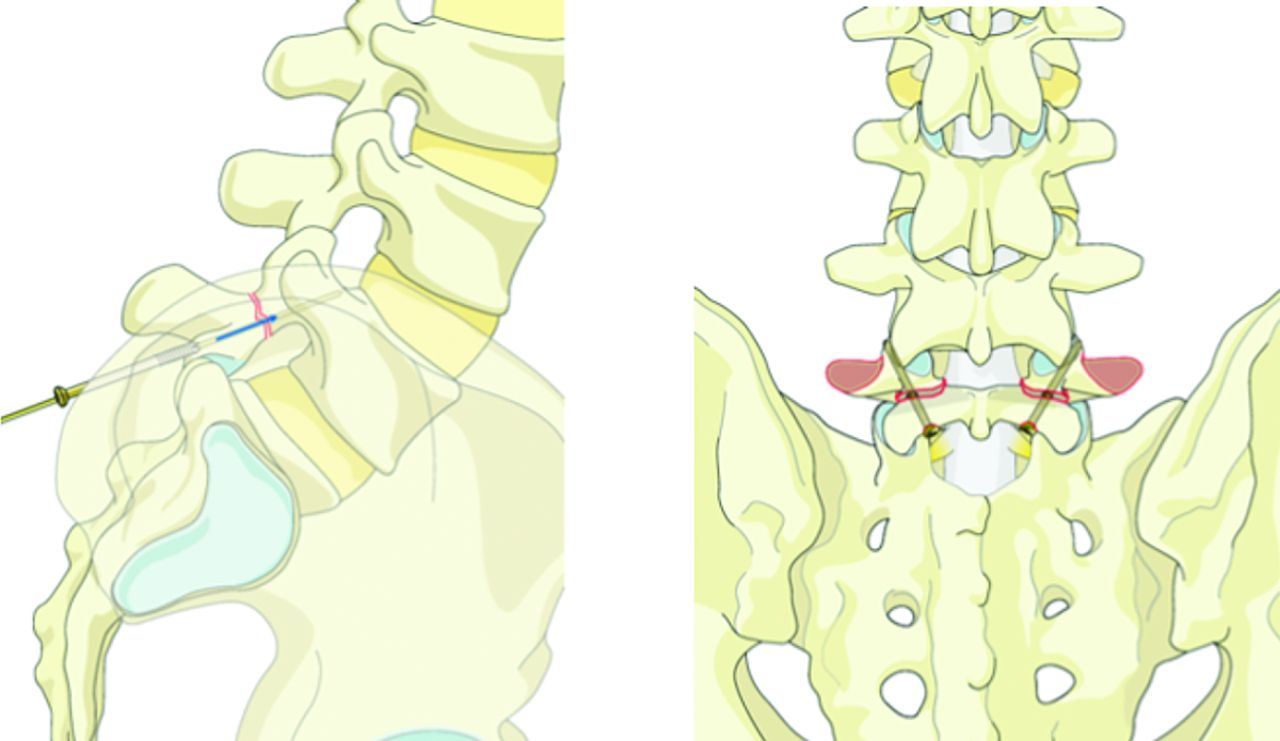
Surgical management is indicated in patients with persistent pain from a nonhealing spondylolytic defect or spondylolisthesis despite a minimum of 6 months of nonsurgical management.4 In high-grade cases with severe symptoms, a shorter trial of nonoperative therapy may be most appropriate. In cases of spondylolysis, direct repair of the pars defect is recommended as opposed to fusion as it spares motion of adjacent spinal segments.64 Several surgical techniques, all with excellent results, have been described to achieve healing of the pars defect including direct screw fixation, wiring technique or pedicle screw-sublaminar hook technique (see Figure 7).64⇓⇓–67 In low-grade spondylolisthesis for an L5 isthmic defect, surgical treatment involves L5-S1 in situ posterolateral fusion and results show excellent clinic outcomes.64
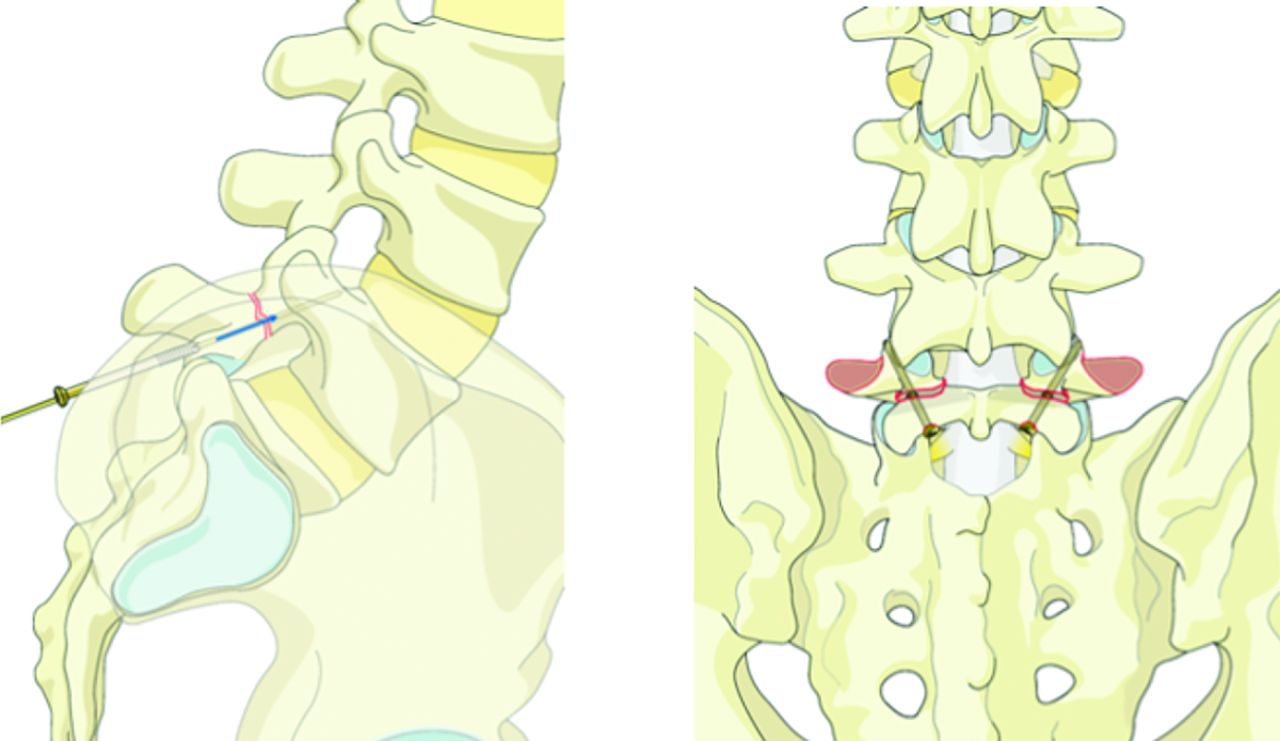
Lateral and posterior views demonstrating direct screw fixation technique for bilateral pars defect repairs. Reproduced with permission from AO Surgery Reference. © by AOSpine International, Switzerland. http://www.aosurgery.org/.
In high-grade spondylolisthesis, the precise surgical procedure remains controversial. While some argue for in situ posterolateral fusion from L4 to S1 (see Figure 8), others argue that spinal fusion with reduction should be performed (see Figure 9).64,68⇓–70 Advantages include restoration of sagittal balance which minimizes lumbosacral shear force and improves fusion rates.64,68 However, instrumented fusions with reductions are more technically demanding, require longer surgical times and lead to increased blood loss compared with in situ fusion.64,69 In addition, iatrogenic neurologic injury, including a traction L5 radiculopathy, occurs at a higher rate and correlates with the degree of reduction achieved.64,71⇓⇓–74 As no high-quality evidence comparing both techniques exist, the authors advocate for a case-specific approach where partial reductions are considered in patients with high-grade slips and high slip angles. Direct decompression in the setting of neurologic deficit should also be considered.

AP and lateral radiographs demonstrating L4-S1 in situ instrumented fusion with fibula allograft for augmentation.
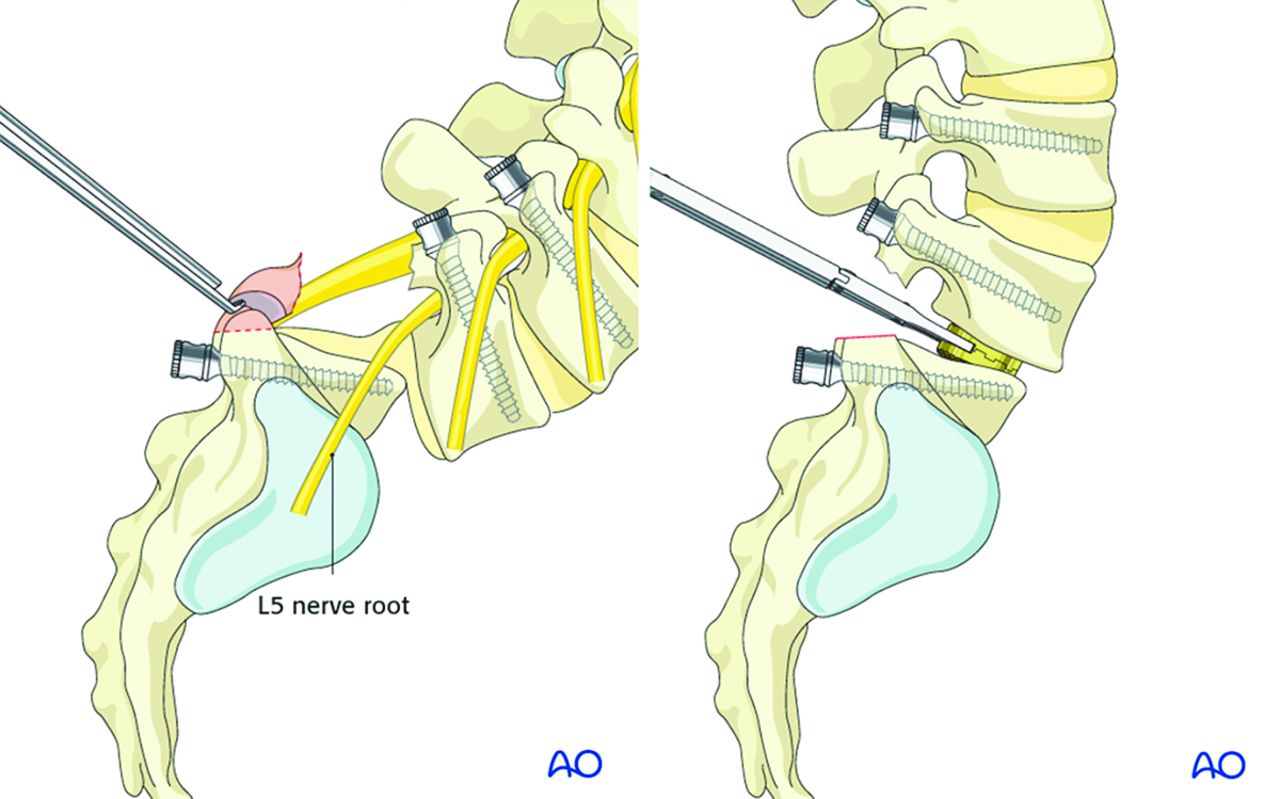
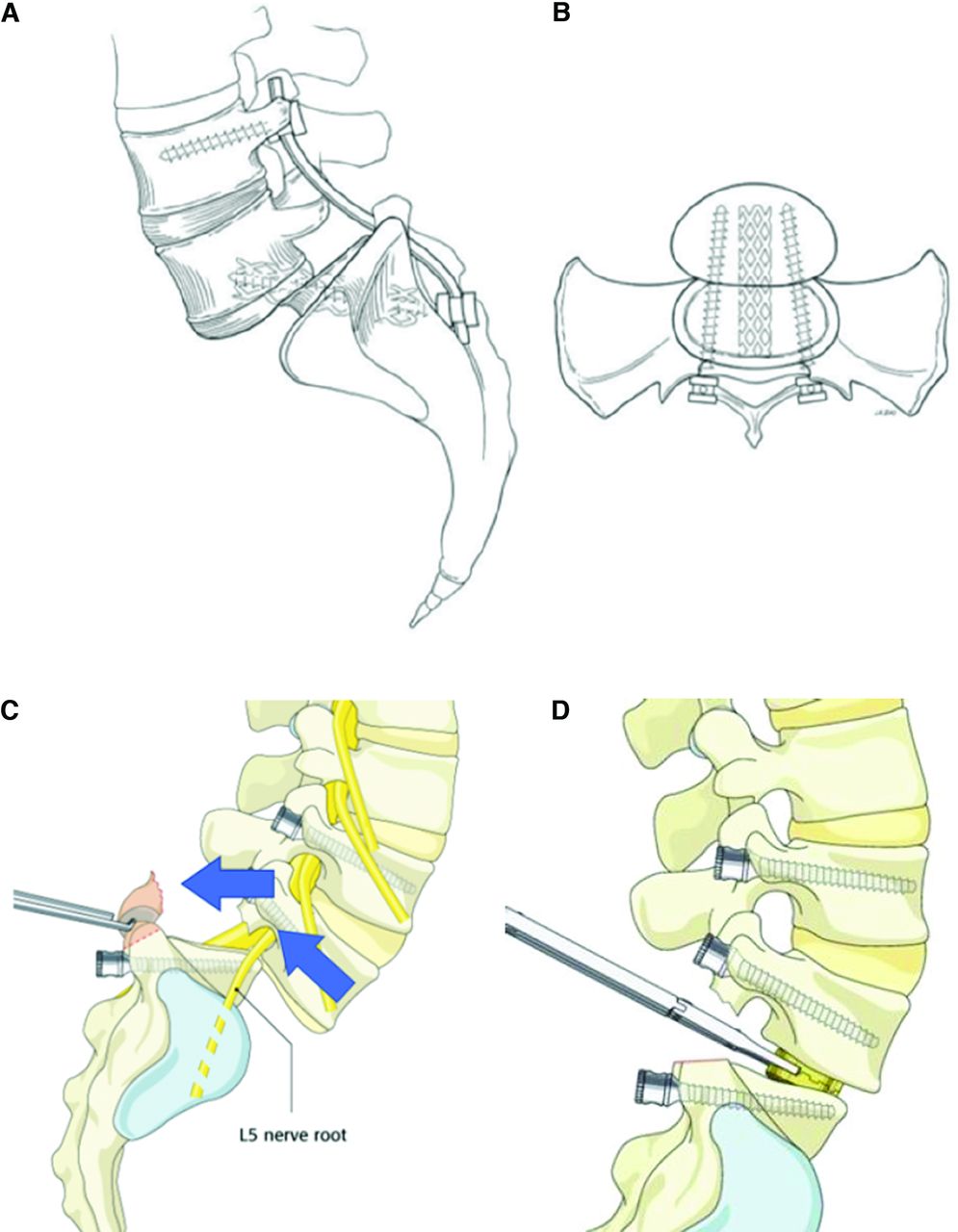
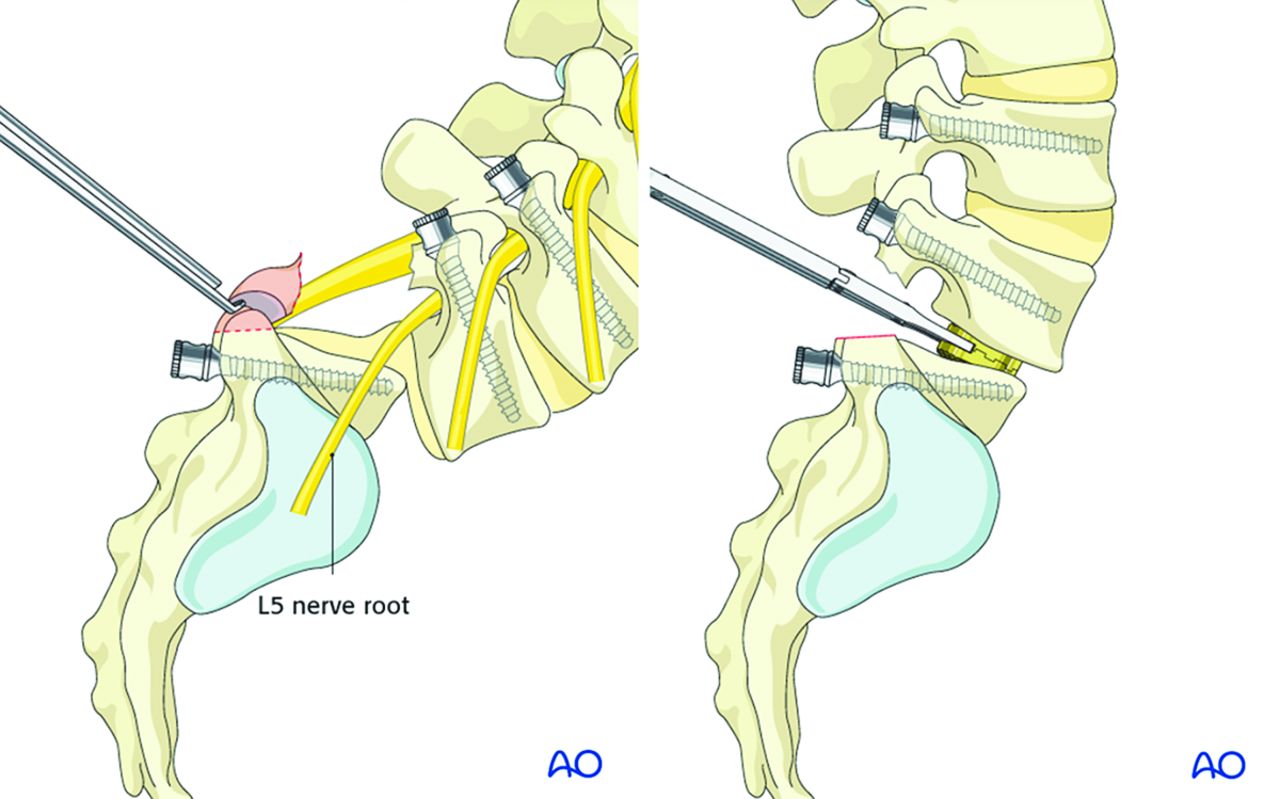
Lateral (left) view demonstrating facet removal for a wide decompression and to gain access to the L5-S1 disk space. Following disk removal, an interbody cage is placed at the L5-S1 disk space (right). Care must be taken during reduction due to the proximity of the L5 nerve root. Reproduced with permission from AO Surgery Reference. © by AOSpine International, Switzerland. http://www.aosurgery.org/.
When to Refer to a Specialist
As spondylolysis and isthmic spondylolisthesis are commonly implicated as organic causes of low back pain in adolescents and young adults, primary care physicians are essential to early detection and initiation of appropriate treatment pathways. In spondylolysis, osseous healing more likely occurs when diagnosed within 1 month of symptom onset, further highlighting the importance of early detection.52,75 In addition to a detailed history and physical examination, standing antero-posterior (AP) and lateral views of the lumbosacral spine as well as flexion/extension views for spondylolisthesis to evaluate instability are indicated to confirm the suspected diagnosis.45,76
While the mainstay treatment of spondylolysis and isthmic spondylolisthesis is nonoperative management, the authors recommend an early referral to an orthopedic specialist in the setting of suspicions of either pathology. Nielsen et al. conducted a retrospective review of 46 patients with symptomatic spondylolysis/isthmic spondylolisthesis and noted that time from initial presentation to diagnosis was 1 week for orthopedic surgeons compared with 25 weeks for orthopedic providers.75 While there are many contributing factors to delayed diagnoses, including insurance authorization for imaging studies, an early referral can allow for a comprehensive discussion about all potential management options and possibly avoid the negative impact on quality of life, social functioning and psychologic health with initiation of early treatment.
Conclusion
Spondylolysis and isthmic spondylolisthesis represent a continuum of a disease process that remains common among the active, adolescent and young adult population.7,9 The hallmark signs include lower back pain with limited lumbar motion and hamstring tightness.77,78 Due to the improved clinical outcomes with early intervention, typically by conservative modalities including activity restrictions and physical therapy, the authors recommend an early orthopedic referral. Nevertheless, primary care physicians play an essential role in the early recognition of these pathologies and should remain informed on risk factors, symptoms and initial work-up.4,52 This review of the pathophysiology, natural history, diagnosis and management of spondylolysis and isthmic spondylolisthesis may serve as a guidance for any physician in the evaluation and triage of patients suspected to be affected by these conditions.
Notes
This article was externally peer reviewed.
This is the Ahead of Print version of the article.
Funding: None.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/6/000.full.
- Received for publication March 28, 2022.
- Revision received June 2, 2022.
- Accepted for publication June 22, 2022.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}