
Abstract
Background: Rates of individuals with a psychotherapy visit has not been well studied, and recent reports lack granularity by age.
Methods: The 2017–2019 Medical Expenditure Panel Survey (MEPS) was used to investigate rates and associations of psychotherapy and psychiatry visits by age/sex and antidepressant/antipsychotic use.
Results: The study included all 90,853 individuals, of which 5.2% (95% CI, 4.9–5.4) reported any psychotherapy (excluding psychiatry visits) visit during a year, while 3.6% (95% CI, 3.4–3.8) reported a visit with a psychiatrist. Females were more likely to have a psychotherapy visit than males after 15 years of age. The highest rates of females with a psychotherapy visit were between 15 and 30 years of age, while rates among males were highest between 10 to 25 years of age. For psychiatry visits, males had higher rates than females during preteen years, similar rates through teen years, lower rates though adulthood, and similar rates after 60 years of age. Rates of a psychiatry visit did not vary as much by age as a psychotherapy visit. Among antidepressant or antipsychotic medication users, the rate of either a psychotherapy visit or a psychiatry visit during a year was markedly higher at younger ages and decreased as age advanced.
Conclusion: Psychotherapy and psychiatry utilization have differences in population level patterns with use being highest among females between 15 to 30 years of age and higher among younger (compared with older) individuals who reported antidepressants or antipsychotics.
- Cross-Sectional Studies
- Health Services Research
- Medical Expenditure Panel Survey (MEPS)
- Mental Health
- Primary Health Care
- Psychiatry
- Psychotherapy
Introduction
Mental Health diagnoses are common in the United States and accounted for the primary diagnosis in over 55 million physician visits in 2018.1 Treatment for these conditions can include some combination of psychotropic medications and/or psychotherapy. Hundreds of randomized controlled trials have been conducted that test psychotherapy for an array of mental health conditions such as major depression, panic disorder, specific phobias, obsessive-compulsive disorder, bulimia nervosa, post-traumatic stress disorder, and bipolar disorder.2⇓⇓⇓⇓–7 While treatment of mental health conditions has increased over the past 30 years, most of the increase has been attributed to increased rates of pharmacotherapy.8
Previous studies have shown generally stable rates of utilization of psychotherapy, while diagnosis and pharmacologic treatment of mental health conditions increased, especially in younger populations.8 However, these studies used data from more than a decade ago and often relied on the Medical Expenditure Panel Survey, which has recently improved methodology to better capture nonphysician aspects of medical care.9 Research into psychotherapy utilization has not been robust likely because this visit type has historically been poorly reimbursed by insurance and not well captured in many data sources. Given this, we investigated the proportion of individuals engaged in any psychotherapy visit or any psychiatry visit during a year and analyzed these rates by age and sex.
Methods
The 2017–2019 Medical Expenditure Panel Survey (MEPS) was used for this repeated cross-sectional study.9 The MEPS is nationally representative of noninstitutionalized population of the United States and is sponsored by the Agency of Health care Research and Quality (AHRQ). This household-based survey collects information of socioeconomic, demographic, prescription medication, and medical care utilization. Each household is included in the survey for 2 years, while each year of the survey includes 2 overlapping cohorts. Importantly, the survey has improved methods for collecting information and includes methods for verifying information, including outreaching to medical providers.9
All individuals in the survey were included in the study. The office-based and outpatient visit files were used to determine psychotherapy visits and psychiatry visits. The primary outcomes of the study were any psychotherapy visit and/or psychiatry visit during a calendar year. Psychotherapy visits were defined as visits with a psychologist or a visit for psychotherapy or mental health counseling that did not occur during a physician visit. There was no report of psychotherapy or mental health counseling in 12% of individuals with a psychologist visit. A psychiatry visit was defined as a visit with a psychiatrist.
Race/ethnicity was categorized as White (non-Hispanic), Black (non-Hispanic), Hispanic, Asian (non-Hispanic), and other race/ethnicities. Antidepressants and antipsychotics were defined by a mix of medication category and prescribed medication name. Serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, trazodone, nefazodone, vilazodone, bupropion, and mirtazapine were classified as antidepressants.
Multivariable logistic regressions were used with the outcome variable being psychotherapy visit during a year and/or a psychiatry visit during a year. Separate regression models were used for each sex and antidepressant/antipsychotic utilization. Restricted cubic splines with 5 knots were used to model age in all regressions. In the regression models by sex, the entire sample was included, and knots were placed at 5, 15, 25, 50, and 70 years of age. For regression models by antidepressant/antipsychotic, only individuals >9 years of age were included, and knots were placed at 15, 30, 45, 60, and 75 years of age. The adjustrcspline command was then utilized to construct postregression estimates. Complex survey weighting and STATA version 17 (STATA Corporation) were used for all analyses. The Ohio Health Institutional Review Board ruled the study exempt.
Results
The study included 90,853 individuals from the 2017–2019 MEPS. Overall, 7.3% (95% CI, 7.0–7.6) of individuals had a psychiatry or a psychotherapy visit during a year. In total, 5.2% (95% CI, 4.9–5.4) of the population reported any psychotherapy visit, while 3.6% (95% CI, 3.4–3.8) reported any psychiatrist visit. Of the individuals with either visit type, 50.8% (95% CI, 48.9–52.9) had only psychotherapy visits, 29.1% (95% CI, 27.3–30.9) had only psychiatry visits, and 20.2% (95% CI, 18.7–21.4%) had both a psychiatry and a psychotherapy visits. Numerous differences were seen in people reporting antidepressant/antipsychotic medications, psychotherapy visits, and psychiatry visits. People who had a psychotherapy visit (compared with a psychiatrist visit) were less likely to be on an antidepressant/antipsychotic (Table 1).
Demographic and Socioeconomic Characteristics of Individuals Reporting Psychotherapy Visit, Psychiatry Visit, and Antidepressant/Antipsychotic Medication
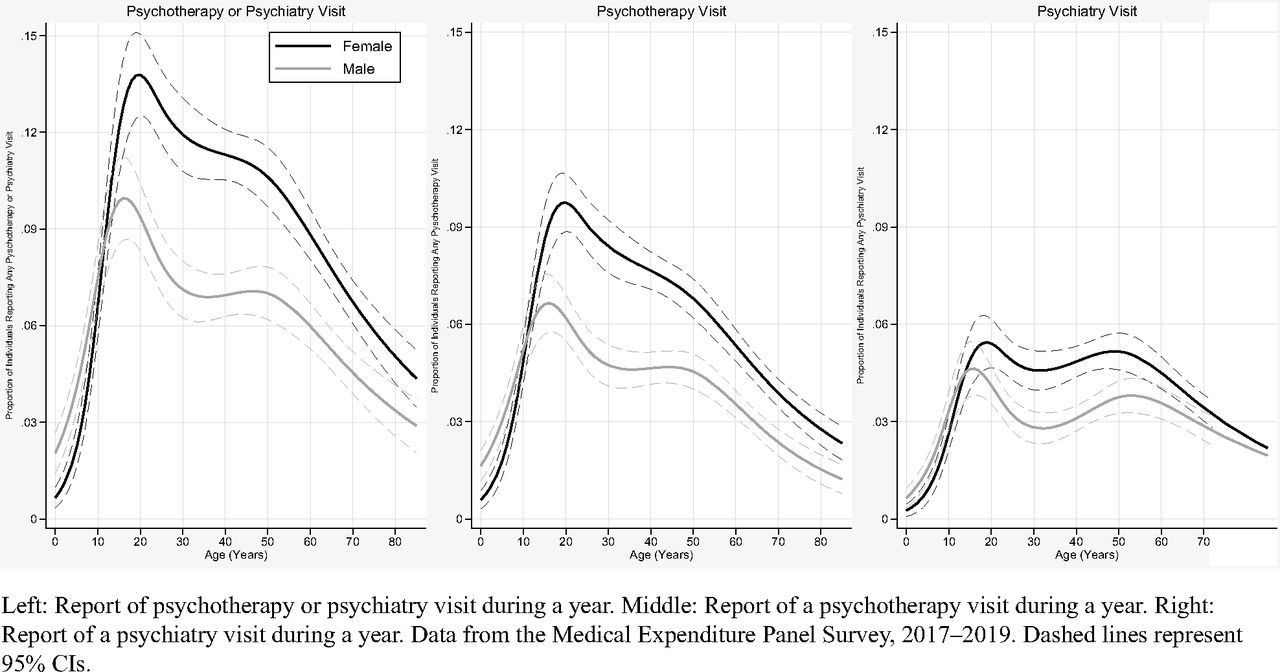
Females between 15 and 85 years of age were more likely to report a psychotherapy or psychiatry visit during a year than males. The highest rates of any psychotherapy or psychiatry visit for females were between 15 and 30 years of age, while the highest rates for males were between 10 and 25 years of age. For psychotherapy visits, females were more likely to have a visit than males after 15 years of age. The highest rates of a psychotherapy visit for females were between 15 and 30 years of age, while males were highest between 10 to 25 years of age. Following these peaks, there was a decline with increasing age for both males and females (Figure 1).
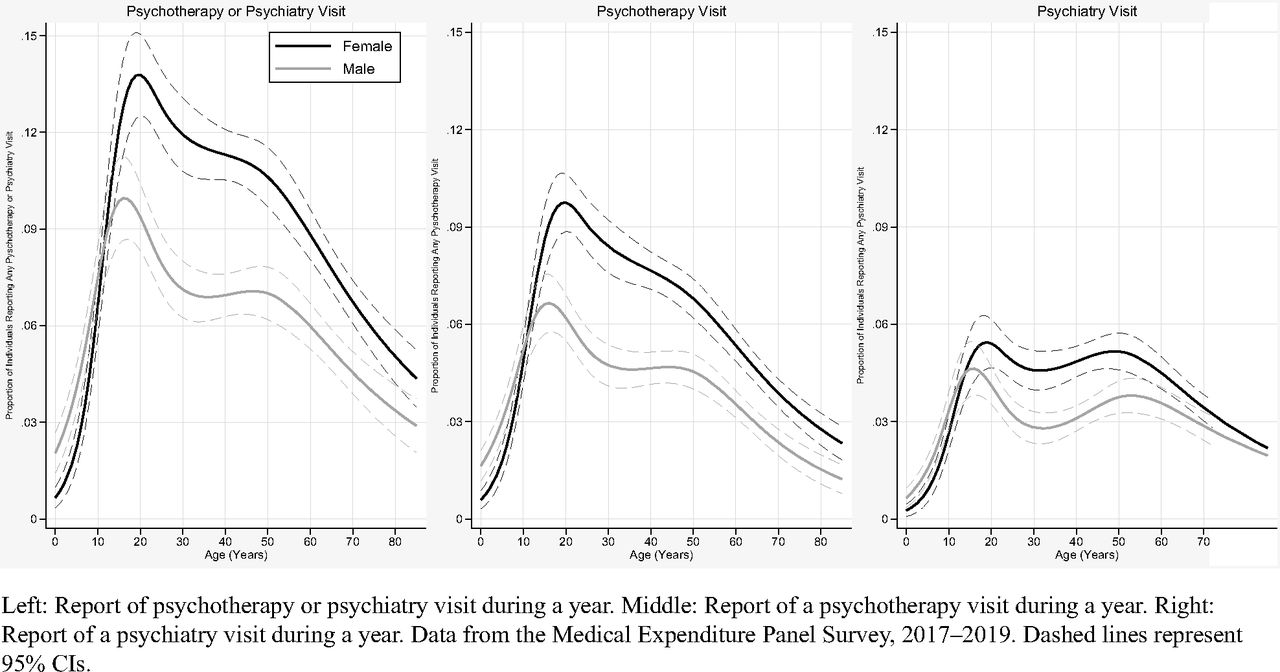
Proportion of population reporting psychotherapy and/or psychiatry visit during a year by age and sex, 2017–2019.
Males were more likely than females to have a psychiatry visit during preteen years and less likely than female through adulthood. There were similar rates between males and females through teen years and after 60 years of age. The rates of psychiatry visits initially peaked in middle teen years for males and late teens for females. Following these peaks, rates declined during the 30s for males and plateaued for females until 60 years of age. After age 60, psychiatry visit rates declined for males and females (Figure 1).
Among individuals who reported an antidepressant/antipsychotic medication during a year, rates of a psychotherapy visit or a psychiatry visit were much higher in younger individuals. Among individuals with no antidepressant or antipsychotic during a year, the proportion of individuals reporting any visit type of the 3 categories was also higher at younger ages (Figure 2).
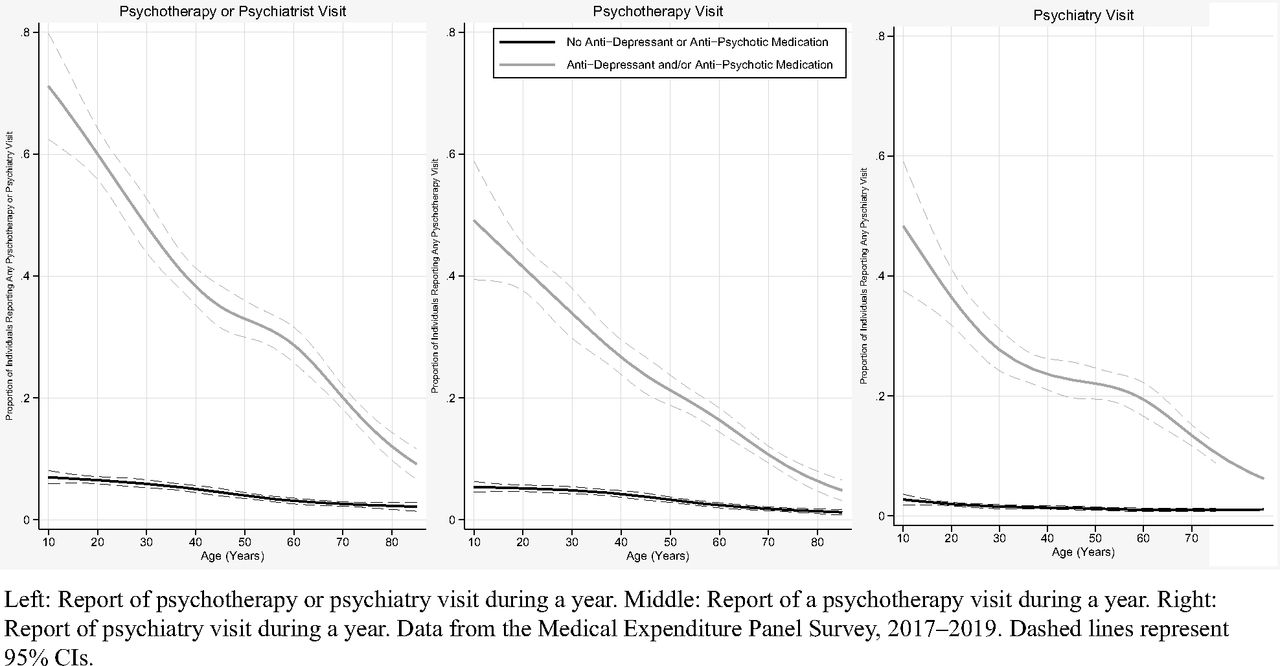
Proportion of population reporting psychotherapy and/or psychiatry visit by age and antidepressant/antipsychotic use during a year, 2017–2019.
Discussion
Our study supports different patterns and levels of use by age and sex at the population level for psychotherapy and psychiatry visits. Females were more likely than males to report a psychotherapy visit after the late teen years. In contrast, males were more likely to report a psychotherapy visit before 10 years of age. This pattern between the sexes is also seen for psychiatry visits until 60 years of age, when there was no notable difference between the groups. Age also has a notable influence on use of psychotherapy with the highest rates of use in the teens to late twenties for both males and females. In contrast, psychiatry visits seem relatively stable between the teens and sixties. Females were also more also likely to report antidepressant use than males, but antidepressant users peaked around age 60 with minimal decrease after age 60 for both males and females.10
There was less difference by sex for psychotherapy visits or psychiatry visits among the youngest or oldest age cohorts. The lowest rate for individuals reporting a psychotherapy (and psychiatry) visit is in the youngest and oldest age ranges, which to our knowledge has not been reported as granularly.11 It seems likely that some combination of differential mental health disorders seen at different ages,12 availability related to insurance,13 differences in social acceptance, and/or previous exposure to these visit types contribute to these patterns. The continual decline of psychotherapy and psychiatry visits among individuals reporting an antidepressant/antipsychotic medication should also be considered in conjunction with the possible indications of these medications as well as the overall patterns of use for different visit types, which is likely, in part, related to lower rates of major depressive disorder in older populations.12
Numerous demographic and socioeconomic categories were associated with psychotherapy and psychiatry visits such as geographic region and race/ethnicity. Given an inability to adequately control for mental health status or past treatments, we would hesitate to draw causal conclusions to explain the differences between different socioeconomic and demographic factors.
The study has important limitations. First, we opted not to build multivariable logistic regression models that included a wider array of demographic and socioeconomic factors given concern regarding the “table 2 fallacy.”14 Second, our data were self-reported, which could result in misreporting of visits. Of note, the survey does have mechanisms for improving reporting and validating visits.9 Third, we were unable to conduct any long-term trending due to changes in survey methodology that improved reporting of visits in recent years.9
Psychotherapy and psychiatry utilization have different population level patterns with use being most common among females between 15 to 30 years of age. Younger individuals reporting antidepressant or antipsychotic medication use were much more likely to report psychotherapy and/or psychiatry visits. Numerous socioeconomic and demographic characteristics were associated with psychotherapy visits and/or psychiatry visits, but better data are needed to determine causation of these differences.
Notes
This article was externally peer reviewed.
Funding: None.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/0/000.full.
- Received for publication December 15, 2021.
- Revision received February 19, 2022.
- Revision received February 28, 2022.
- Accepted for publication March 1, 2022.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.