
Abstract
Background: CRC screening is recommended for adults aged 45–75. Mt-sDNA is indicated for asymptomatic individuals between the ages of 45 and 85, but not for those with rectal bleeding, iron deficiency anemia, adenomatous polyps, previous colonoscopy within 10 years, family history of CRC, positive results from CRC screening tests within the past 6 months, or age less than 45 and greater than 85. We aimed to determine the prevalence of mt-sDNA use when not indicated and factors associated with inappropriate testing.
Methods: 7,345 patients underwent mt-sDNA testing and were randomized using EMERSE. Charts for the first 500 patients were reviewed to determine whether mt-sDNA was ordered appropriately according to the USPSTF criteria. Seven patients were excluded due to having more than one inappropriate ordering for mt-sDNA.
Results: Of 500 patients, 22.2% had an inappropriately ordered mt-sDNA test. The most common reason for inappropriate ordering was having a previous colonoscopy done within the past 10 years. Rates of inappropriate testing significantly varied by race and the specialty of the ordering provider, with internal medicine providers ordering the most mt-sDNA tests. Rates of inappropriate testing did not significantly vary by sex or type of insurance.
Discussion: Our study suggests that providers may not be familiar with guidelines for the indicated use of mtsDNA, leading to inappropriate referrals and increased costs. Patients at increased CRC risk would benefit from a more sensitive procedure such as a colonoscopy. Future studies could understand the motivation to order testing outside approved indications through provider surveys and interviews.
- Colorectal Cancer
- Cost Effectiveness
- DNA
- Internal Medicine
- Prevalence
- Preventive Medicine
- Public Health
- Referral and Consultation
- Screening
Introduction
Colorectal cancer screening (CRC) is recommended for adults aged 45 to 75.1 Indirect screening options include fecal immunochemical tests (FIT) and multitarget stool DNA (mt-sDNA) (Cologuard). Mt-sDNA is indicated for asymptomatic individuals between the ages of 45 and 85.2 Mt-sDNA is not indicated in patients with rectal bleeding, iron deficiency anemia, adenomatous polyps, previous colonoscopy within 10 years, family history of CRC, positive results from CRC screening tests within the past 6 months, or age less than 45 and greater than 85.3 Our study’s purpose was to determine the prevalence of mt-sDNA use when not indicated and understand the most common reasons why mt-sDNA was not indicated but ordered anyway.
Methods
A total of 7,345 patients within a Midwestern metropolitan health system’s EMR system underwent mt-sDNA testing between January 1, 2021, and December 31, 2021. Electronic Medical Record Search Engine (EMERSE) was utilized to randomize the sample, from which the first 500 randomized patients were reviewed from an ambulatory electronic health record of an academic health system.4 Any patient who was ordered and successfully completed mt-sDNA testing within the date range was included. Patients were excluded based on unsuccessful completion of testing, if there was more than 1 inappropriate reason for testing, or missing EMR information.
Medical records were reviewed to determine whether the tests were ordered appropriately according to the US Preventive Services Task Force criteria released in 2016.1 7 patients were excluded due to having more than 1 inappropriate ordering for mt-sDNA. Race, sex, insurance type, and the specialty of the ordering provider were recorded as part of demographic data on our selected participants. JASP statistical software was used to conduct Chi-squared and 2-proportion Z-test analyses.
Results
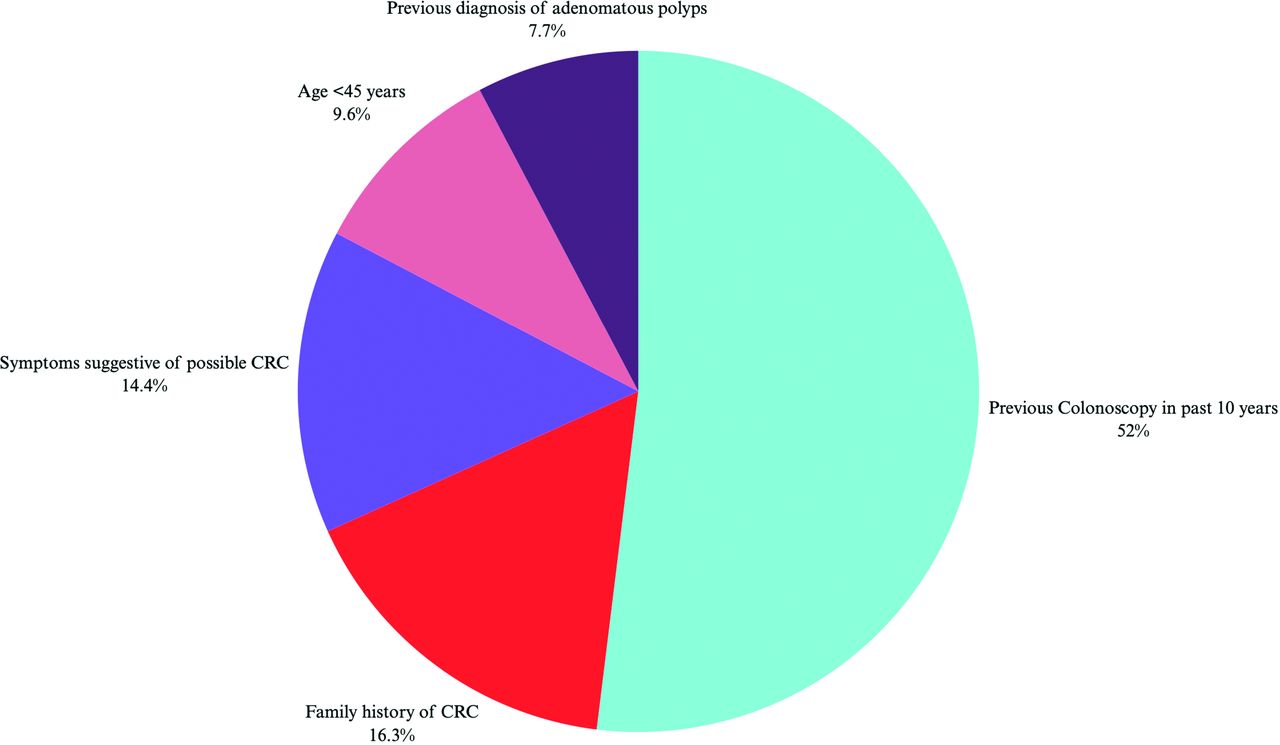
Of the 500 patients, (22.2%; n = 104) had an inappropriately ordered mt-sDNA test. The most common reason for inappropriate ordering was having a previous colonoscopy done within the past 10 years (51.9%; n = 54) (Figure 1). The specialties that ordered the most mt-sDNA were family medicine (58.4%; n = 292) and internal medicine (34.6%; n = 173) (Table 1). Race differences in inappropriate testing were significant, with White race being most likely to receive inappropriate testing (26.2%; n = 72; P < .001). Specialty specific rates of inappropriate testing were also significant, with Internal Medicine providers most likely to conduct inappropriate testing (28.3%; n = 49; P < .001). No statistically significant difference was found in male versus female rates of inappropriate testing (22.4% vs 19.6%; P = .40). Similarly, rates of inappropriate testing based on insurance type, Commercial or Government insurance, were not statistically significant (16.8% vs 23.1%; P = .07).

Reasons for inappropriate testing. Abbreviation: CRC, Colorectal cancer screening.
Rates of Off-Label Testing for Sample Characteristics
Discussion
Our study assessed the rate at which mt-sDNA was inappropriately ordered, the most common reasons for why mt-sDNA was not indicated but ordered anyway, which specialties ordered the most mt-sDNA, and whether rates of inappropriate testing varied by race, sex, insurance type, and the specialty of the ordering provider. This research was not designed to determine why patients and physicians selected mt-sDNA over colonoscopy.
This is the second study to evaluate the inappropriate use of mt-sDNA. In a sample of 902 patients, Agarwal et al. found 17.7% of all mt-sDNA tests were inappropriately ordered tests, most commonly because of being up to date with screening colonoscopy.5 Similarly, in our sample, more than 20% of patients had inappropriate ordering of mt-sDNA, most commonly because patients were up-to-date on screening colonoscopy or were above average risk for CRC. This trend could be explained by several factors. Patients may refuse colonoscopy, and mt-sDNA may be substituted. Physicians may also offer mt-sDNA as a low-risk alternative for patients at high-risk for adverse events after colonoscopy. Lastly, providers may be unfamiliar with guidelines for appropriate use of mt-sDNA.
Significant race differences existed in the rate of inappropriate testing, with White race being more likely to receive testing when contraindicated. This finding underscores differences in health care access and quality among race groups, as well as the burden of unconscious bias which may be at play in the landscape of mt-sDNA testing. In contrast, we found no significant sex differences in the rates of inappropriate testing, which is similar to previous findings by Agarwal et al.5 In addition, differences in insurance type did not significantly correlate to differences in inappropriate testing, which contextualizes our findings within the larger health care ecosystem. Our findings also demonstrate that the frequency of inappropriate testing significantly varies by the specialty of the provider, with Internal Medicine being the specialty with the highest rate of inappropriate testing. Future research assessing the trend of inappropriate mt-sDNA testing should consider these specialty-specific differences to better understand the reasons why physicians and patients would elect for mt-sDNA over colonoscopy in situations where mt-sDNA would be inappropriate.
If our findings are confirmed, they have cost implications as the direct cost of mt-sDNA is $650.6 Furthermore, patients at increased CRC risk would benefit from a more sensitive procedure such as a colonoscopy, rather than mt-sDNA.7 Future studies could understand the motivation to order testing outside approved indications through provider surveys and interviews.
Limitations include a limited number of specialists, though the vast majority of tests are ordered by primary care providers. In addition, this study was conducted at a single institution within an outpatient setting; future studies spanning multiple institutions or geographic locations are required to more reliably assess the findings of this study. Our study was conducted during the COVID-19 pandemic, when there was increased use of noninvasive CRC screening; it is possible that our data captured an increased number of inappropriate mt-sDNA testing as a result.
We suggest that increasing provider education on the appropriate ordering of noninvasive screening may help decrease the rate of inappropriate referrals, save costs, and improve clinical outcomes in patients at higher risk for CRC.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: The authors have no conflicts of interest to report.
To see this article online, please go to: http://jabfm.org/content/37/2/328.full.
- Received for publication April 27, 2023.
- Revision received November 21, 2023.
- Revision received November 28, 2023.
- Accepted for publication December 4, 2023.




{kind=link}