
Abstract
Purpose: Food insecurity (FI) is a hidden epidemic associated with worsening health outcomes affecting 33.8 million people in the US in 2021. Although studies demonstrate the importance of health care clinician assessment of a patient’s food insecurity, little is known about whether Family Medicine clinicians (FMC) discuss FI with patients and what barriers influence their ability to communicate about FI. This study evaluated FM clinicians’ food insecurity screening practices to evaluate screening disparities and identify barriers that influence the decision to communicate about FI.
Methods: Data were gathered and analyzed as part of the 2022 Council of Academic Family Medicine’s Educational Research Alliance survey of Family Medicine general membership.
Results: The majority of respondents reported (66.9%) that their practice has a screening system for food insecurity, and most practices used a verbal screen with staff other than the clinician (41%) at specific visits (63.8%). Clinicians reported “rarely or never asking about FI” 40% of the time and only asking “always or frequently” 6.7% of the time. Inadequate time during appointments (44.5%) and other medical issues taking priority (29.4%) were identified as the most common barriers. The lack of resources available in the community was a significant barrier for clinicians who worked in rural areas.
Conclusions: This survey provides insight into food insecurity screening disparities and identifies obstacles to FMC screening, such as time constraints, lack of resources, and knowledge of available resources. Understanding current communication practices could create opportunities for interventions to identify food insecurity and impact “Food as Medicine.”
- CERA
- Family Medicine
- Food Insecurity
- Health Communication
- Nutrition Assessment
- Screening
- Social Determinants of Health
- Surveys and Questionnaires
Introduction
Food Insecurity (FI) is a social determinant of health defined as “a household-level economic and social condition of limited or uncertain access to adequate food.”1 FI has been identified as a hidden epidemic within the US, affecting 13.5 million households, or 10.2% of the general population in 2021.2 Of those households, 3.8% have been identified as having very low food security, defined by disrupted eating patterns, or reductions in either food quality or intake.1,3 FI is associated with worsening outcomes in pediatric development, including higher rates of asthma, behavioral, academic and emotional concerns and increased emergency department use.4⇓–6 Adults who face FI are at greater risk for chronic diseases, including hypertension, obesity, and depression7⇓⇓⇓–11 and FI leads to increased all-cause mortality.12 Due to the related health outcomes, food insecure individuals have higher annual health care costs estimated at $1834 higher per year than for food secure adults.13 Evidence suggests that addressing FI may improve health outcomes, and decrease health care costs.14 With the 2022 governmental Task Force on Hunger, Nutrition, and Health working to accelerate access to “Food is Medicine” and the National Institute for Health asking for additional research to understand and address FI, there is a need for facilitated health system screening, referrals, and appropriate interventions. Evaluation of best use of screening mechanisms is necessary with the changing standards of care.15,16 Although the United States Preventive Services Taskforce (USPSTF) and the American Academy of Family Physicians (AAFP) do not have current guidelines for FI screening, this is a preventive health topic in development.17
Family Medicine clinicians are uniquely poised to identify patients with FI, as they are often familiar with both the patient’s medical and social history in the setting of longstanding relationships. Studies have demonstrated that despite this, formal clinician FI screening is rarely utilized, with only 24% of hospital organizations and 16% of physician practices performing FI screening.18
Despite the similarities in FI levels, (11.6% rural vs 12.7% metropolitan),3 in rural areas, FI may be further exacerbated due to reduced access to resources (eg, food banks, financial support, social services) compared with urban areas. Furthermore, rural clinicians often treat an older population suffering from more chronic conditions and who may be at higher risk of worse outcomes due to inadequate nutrition and less attention to FI given the competing demands of medically complex patients.19
Although studies demonstrate the importance of health care clinician assessment of a patient’s food security,4,5 little is known about whether Family Medicine clinicians discuss FI with patients and what barriers influence clinicians’ ability to screen and communicate on this sensitive topic. Although many clinicians understand the potential impact of FI on patient outcomes, they may avoid addressing social needs due to the complexity of clinical issues.20,21 Family Medicine clinicians may also harbor stereotypes of what types of patients experience FI, introducing bias into FI assessments and increasing the risk of missed assessments. Lack of training on how to talk to patients about FI and lack knowledge about existing resources to offer patients may also affect clinicians’ comfort with FI screening and communication. Clinicians may also expect that the system is addressing this issue through other methods making their need to address it unnecessary.22,23 This study aimed to determine the extent to which Family Medicine clinicians discussed FI with patients; evaluated barriers impacting whether clinicians screen for FI; and identified factors influencing the decision to discuss FI with patients.
Methods
We included 5 questions addressing FI as part of the 2022 Council of Academic Family Medicine’s (CAFM) Educational Research Alliance (CERA) survey of Family Medicine educators and practicing physicians, which is a nationally representative sample of academic Family Medicine clinicians. Our research team worked with research mentors, the CERA survey Director, and the CERA steering committee to evaluate questions for consistency with the overall subproject aim, readability, and existing evidence of reliability and validity. Pretesting was conducted with Family Medicine educators who were not included in the sampling frame, and included evaluating questions for flow, timing, and readability. For the full survey, participants with a US address were selected based on membership type (resident and student members were excluded). The pool excluded program directors, clerkship directors, and department chairs as these members are surveyed separately by CERA. Invitations to participate in the study included a personalized greeting and survey link, which was conducted through SurveyMonkey. Nonrespondents received 4 requests for survey completion. The survey was distributed to 5161 respondents, of whom 80 declined participation and 210 had undeliverable addresses. In total, the survey was provided to 4871 CAFM organization members for completion between January 11, 2023, and February 12, 2023. Self-reported demographics of the sample pool are based on membership data from the Association of Departments of Family Medicine, the North American Primary Care Research Group, and the Society for Teachers of Family Medicine including region of the country, degree earned, gender, age, race/ethnicity and whether members self-identify as an Underrepresented Minority.
The FI component of the CERA survey included 5 questions on FI related to attributes and barriers to screening and diagnostic inquiry. The respondents were asked 1) How is FI screening performed (Select 1: Article form, Tablet/online questionnaire, Verbal screen with staff member, Verbal screen with clinician); 2) How often is screening for FI performed (Select 1: Once/new patient visits, Specific visit (ie, annual physical, prenatal visits, etc.), All visits); 3) How often do you, as the clinician, personally ask a patient about FI? (Select 1: Never, Rarely, Sometimes, Frequently or Always); 4) As the clinician, what would influence your decision to ask about FI? (Rank top 3: The subject comes up in conversation; The patient reports a change in living status; such as loss of a job or home; The patient or patient’s family has a history of homelessness or poverty; The patient seems malnourished or has an abnormal Body Mass Index (BMI); I use my intuition; If I have time after addressing clinical issues; or FI screen (already done) identifies an issue); and 5) What do you perceive as the most challenging obstacles in addressing food security with your patients? (Rank in order: Inadequate time during appointments; Lack of knowledge about the issue of FI; Lack of knowledge about available resources for FI; Lack of resources in my community to address FI; Other medical issues take priority; FI is not common enough in my ambulatory practice; Lack of training on how to talk to patients about FI; Discomfort in talking to patients about FI; or FI assessment is outside of the scope of my practice).
Data Analysis
Descriptive statistics were computed for demographics, practice settings, and responses to survey questions on FI. The association of survey respondents’ demographic/practice variables with their response to how often they personally asked about FI was assessed using Pearson Chi-squared test for categorical variables and 1-way ANOVA for age. A generalized linear model was used to evaluate the demographics/practice factors that influenced ranking of the 4 most ranked reasons in the decision for clinicians to screen for FI. For each demographic/practice factor, this analysis assessed if there was a differential influence of the demographic/practice factor among the 4 reasons, and then examined how much (if any) the factor was associated with ranking each reason. From the fitted generalized linear model, the proportion (with 95% confidence interval, CI) that ranked a reason among the top 3 were computed and compared among the factor levels, with the factor effect expressed as odds ratios (with 95% CI). The same analysis was performed for the 4 most ranked barriers for screening for FI. In addition, the association of location of demographics/practice setting with rank score (1, 2, 3, or unranked) of “lack of resources available in the community” as barrier was tested using Wilcoxon rank-sum or Kruskal-Wallis tests. All statistical analyses were performed using SAS (version 9.4; SAS/STAT 14.3).
The study was approved by the American Academy of Family Physicians Institutional Review Board (IRB) in December 2022. The University of Iowa’s IRB determined that this study is exempt from IRB review.
Results
Respondent Demographics
The overall response rate for the CERA general membership survey was 25% (1216/4871). Of the 1216 respondents, 285 did not see patients in a clinical setting. An additional 18 did not answer at least 1 of the 4 FI questions and were excluded, leaving 18.7% (n = 913) respondents who were included in the analysis. Based on self-reported demographics, respondents were distributed across all regions of the US and worked in urban (51.5%), suburban (32.4%) or rural (16.1%) practices with 27.3% of respondents reporting that they worked in underserved areas. Most respondents identified as White (74.7%) and female (63.3%), with 17.8% identifying as underrepresented in medicine.
Clinician Screening Practices
Two-thirds of the respondents (66.9%) reported that their practice has a screening system for FI either verbally by staff (41%), by article questionnaire (29.7%) or by online form (19.8%). Only 9.5% of clinicians reported personally asking patients about FI. Of the 9.5% of clinicians that personally asked patients about FI, this was most often done at specific visits (63.8%), such as physicals or prenatal visits. Overall, only 6.7% of clinicians “always” or “frequently” ask about FI, with most clinicians asking sometimes (53.3%), and almost 40% of clinicians rarely or never asking about FI. Although most demographic characteristics (Table 1) did not correlate with the frequency of clinicians asking about FI, a significant association was observed with clinician gender (Table 2). Female clinicians “always/frequently” ask about FI 75% of the time and are less likely than male clinicians to “rarely/never” ask about FI (OR 2.07; 95% CI 1.11-3.85; P = .022). Clinicians that identified as working in an underserved area were less likely to ask about FI (P = .0005; Table 2). However, those that asked about FI asked “always/frequently” 21.7% of the time, “sometimes” 22.7% of the time, and “rarely/never” 34.4% of the time (with rarely/never as a reference category; Frequent/Always OR 0.53; 95% CI 0.28-1.01; P = .054; Sometimes OR 0.56; 95% CI 0.41-0.76; P = .0002).
Demographic Characteristics of Survey Respondents
Demographic Characteristics of Survey Respondents Based on How Often Clinician Personally Asked about Food Insecurity
Factors Influencing FI Screening
When asked what would influence the decision to discuss FI with patients, the number 1 reason clinicians indicated was that the issue was already identified during the encounter in a separate FI screen (29%) (data not shown). Most commonly, the top 3 reasons for discussing FI included a change in patient living status (67%), patient/family history of homelessness/poverty (65%), or “when it comes up in conversation” (57%) (data not shown). These reasons were more likely to influence the decision to discuss FI instead of appearance, or BMI outside the recommended range, intuition, and time after addressing clinical issues. Clinicians identifying as female versus male were significantly more likely to ask about FI based on a change in living status (OR 1.82; 95% CI 1.26-2.62, P < .0001) (Figure 1A). Clinicians over age 60 compared with those under 40 years old were more likely to ask about FI if the patient had either a family history of homelessness or poverty (OR 2.22; 95% CI 1.09-4.56, P < .02) (Figure 1B), but younger physicians were more likely to ask if it came up in conversation (OR 0.39; 95% CI 0.20-0.74, P < .0001) (Figure 1D). As respondents over age 60 were more likely to earn their degree before the year 2000, a similar significance was observed when comparing the year of degree earned (Figure 1C and 1E and Appendix Table 1).

Clinician gender, age and graduate degree year influence Food insecurity (FI) screening based on patient-identified factors. (A) Female clinicians are more likely to screen for FI if a “patient reports a chance in living status compared with male clinicians (OR 1.82; 95% CI 1.26-2.62, P < .0001). (B and C) Clinicians older than 60 yrs. (OR 2.22, 1.09-4.56, P < .02) or who received their degree before 2000 (OR 0.55; 95% CI 0.34-0.89; P = .004) were more likely to screen for FI based on a patient’s history of homelessness or poverty. (D and E) Clinicians younger than 40 yrs. (OR = 0.39; 95% CI = 0.20-0.74; p < 0.0001) or who received their degree after 2010 were more likely to screen for FI based if the subject came up in conversation (OR = 1.81; 95% CI = 1.14-2.87; p =0.003).
Top Factors Influencing Providers Decisions to Discuss Food Insecurity (FI) with Patients, by Respondent's Demographic Characteristics
Obstacles Influencing the Decision to Ask about FI
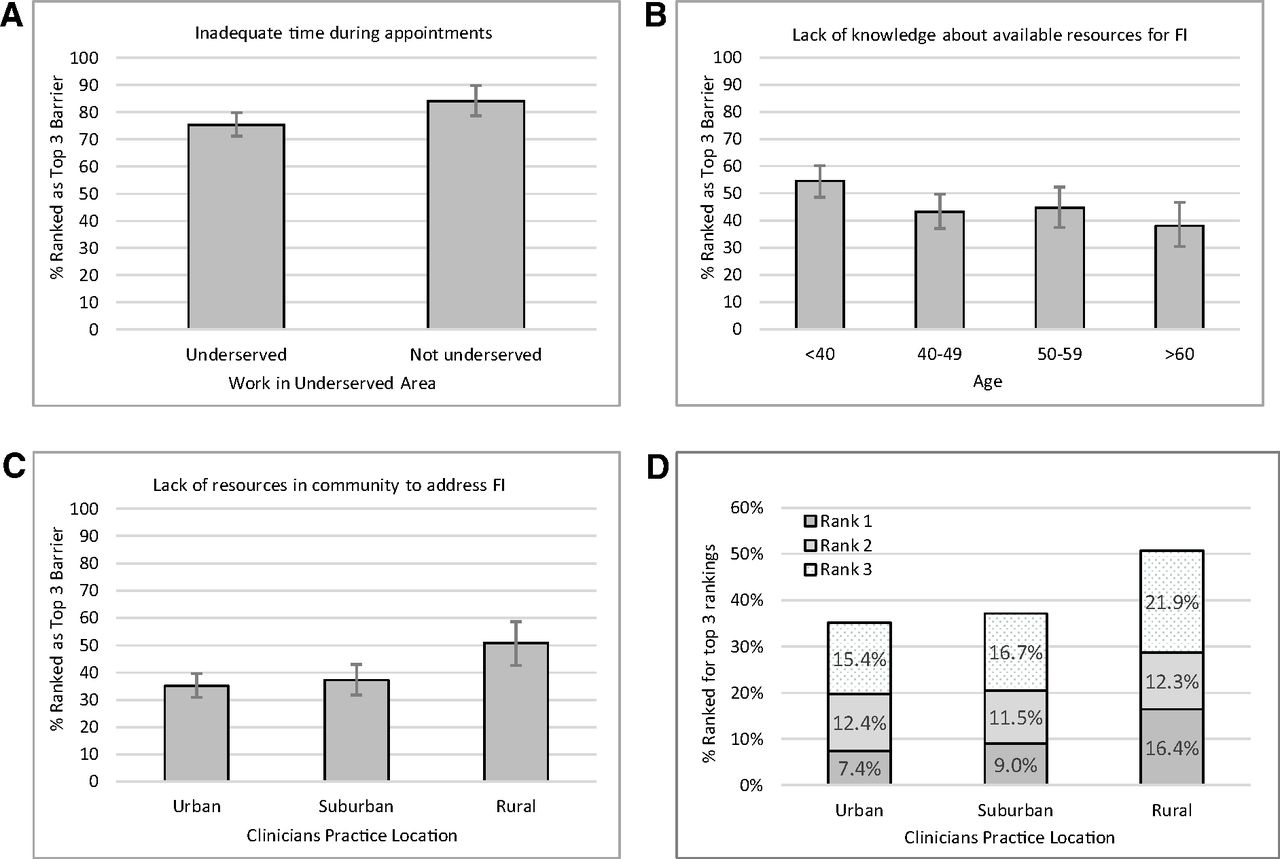
Although certain factors influenced the decisions to screen, additional obstacles that could have impacted the decision to ask about FI were evaluated. Inadequate time during appointments (44.5%) and other medical issues taking priority (29.4%) were most selected as the number 1 obstacles for clinicians (Appendix Table 2). Specifically, inadequate time during appointments was more often ranked as a top obstacle by clinicians not working in underserved areas (OR 0.58; 95% CI; 0.36-0.91; P = .01) (Figure 2A). Lack of knowledge about available resources (45.6%) or the availability of resources (38.4%) was identified as a top 3 obstacle. Older clinicians (>60 yrs.) were less likely to cite “lack of knowledge about available resources” as an obstacle than younger clinicians (<40 yrs.) (OR 0.52; 0.27-0.99; P < .05) (Figure 2B). Lack of resources available in the community was an obstacle cited significantly more by clinicians who worked in rural areas than in urban areas (OR 0.53; 95% CI 0.30-0.91; P = .001) (Figure 2C). Lack of community resources was ranked as the number 1 obstacle by 16.4% of rural clinicians compared with 9% for suburban clinicians (P = .001) and 7.4% for urban clinicians (P = .001) and as a top 3 choice for 50.6% of rural clinicians compared with 35.2% of urban clinicians (Figure 2D).

Clinician demographics influence ranking of top 3 barriers to discussing Food insecurity (FI) during patient encounters. (A) Clinicians working in underserved areas were less likely to rank “inadequate time during appointments” as a top barrier (OR 0.58; 95% CI 0.36-0.91; P = .01). (B) Clinicians under 40 yrs. of age were more likely than clinicians over 60 yrs. of age to rank “lack of knowledge about available resources for FI” in the top barriers (OR 0.52; 95% CI 0.27-0.99; P < .05). (C) Clinicians practicing in rural locations were more likely to rank “lack of resources in the community to address FI” as a top barrier compared with urban locations (OR 0.53; 95% CI 0.30- 0.91; P = .01). (D) Lack of community resources was ranked as the number 1 barrier by rural clinicians compared with suburban clinicians (P = .001) and compared with urban clinicians (P = .001).
Most Challenging Obstacles in Addressing Food Insecurity (FI), by Respondent's Demographic Characteristics
Discussion
The majority of respondents (66.9%) reported that their practice had a screening system for food insecurity; and most practices used verbal screens with staff other than the clinicians (41%) at specific visits (63.8%). Clinicians reported “rarely or never asking about FI” 40% of the time and only asking “always or frequently” 6.7% of the time. Inadequate time during appointments (44.5%) and other medical issues taking priority (29.4%) were identified as the most common barriers. The lack of resources available in the community was a significant barrier for clinicians who worked in rural areas.
Recent Increases in FI Screening in the Medical Context and the Importance of Screening
The results of this CERA general membership survey provided insight into FI screening and disparities and identified potential obstacles to clinician screening. The 2017 to 2018 National Survey of Health care Organizations and Systems indicated that only 16% of physician practices screened for FI speaking to the hidden nature of the epidemic.18 However, the results of this CERA study showed most clinicians (66.9%) said their practice had some screening in place which may be an indirect result of the “food as medicine” initiatives. This CERA study evaluated only Family Medicine clinicians compared with a pool of hospitals and physician practices and the large difference between the values may suggest that FI screening is likely increasing across primary care practices and may have differential uptake in Family Medicine settings. Although primary care practices have available screening tools for social determinants of health (SDOH) and current task forces call for screening, there is no clear standard of care for how to screen, and data suggest few medical practices and hospitals screen for all SDOH.18 Similarly, this study indicated that only 6.7% of Family Medicine clinicians personally ask “always” or “frequently” about FI and nearly one-third of respondents do not screen. Patient centered communication skills encourage maintaining the relationship first in difficult conversations24 and further study is needed to understand how a clinician determines when to discuss FI while in the context of protecting the patient clinician relationship. With the current vision to intervene in FI, screening for FI is only 1 step in the FI landscape, it will not substantively solve the disparities or inequities in the under resourced communities.
When deciding whether to ask about FI, clinicians often relied on several aspects of information gathering to choose whether to initiate a discussion about FI. The 2 most ranked factors for clinicians asking about FI were a positive FI screen (29.9%) and if FI came up in conversation (23.6%) suggesting that clinicians may decide not to independently discuss FI. However, a patient-reported change in living status or a history of homelessness/poverty were the top 2 reasons clinicians gave for choosing to screen for FI. Although these factors may be associated with FI, they likely only identify a subset of patients experiencing FI, as FI can be temporary and impacts people across a broad income spectrum.3 Interestingly, female clinicians were more likely to select a change in living status as a factor leading them to ask about FI, and additional research is needed to understand how gender influences screening decisions. It is likely that the patient specific factors or demographics that impact clinicians choosing to engage in a discussion about FI may also reflect sensitivity to best communication practices and the clinicians’ concern about impacting the patient-clinician rapport. Further research to dissect the specific impacts about FI discussion timing is needed.
Reluctance to Screen in Less Well-Resourced Areas or When Knowledge of Resources Is Limited
With new policy recommendations to increase access and participation in federal nutrition programs through the 2022 Task Force Report Informing the White House Conference on Hunger Nutrition and Health,16 there may be more access to resources. Despite this effort, the survey found that 2 other major obstacles to addressing FI were lack of knowledge of available resources or the lack of community resources. There is some overlap between these 2 as there may be resources, but the clinician may be unaware. Alternatively, there may be little to no resources available in the community or access to resources in nearby urban settings may be out of patient reach.3 Interestingly, clinicians who self-identified as working in an underserved area were statistically less likely to ask about FI. With underserved areas having limited food access,3 this seems counterintuitive; however, further research could explore the hypotheses that the number of positive screens may outweigh available resources leading to a reduction in screening, that clinicians may screen less in settings with high prevalence assuming the issue is likely present, or how stigma and norms around inquiry may differ across settings.
Although not statistically significant, there was a trend toward rural clinicians asking about FI less frequently. This could partially explain the lower reported screening by clinicians in underserved communities, as there is overlap between the 2 populations. This lower FI screening rate may also reflect the lack of available resources for patients in underserved or rural communities, which limits clinicians’ ability to effectively address FI concerns in this at-risk population.
This survey found that rural clinicians were more likely than their urban counterparts to identify lack of community resources as a top obstacle to addressing FI in the clinical context. Given high rates of rural FI, reducing barriers to clinical screening in this context is critical, as is improving availability of and access to rural services.
Limited Time for Screening
Inadequate time during appointments and other medical issues taking priority were listed as the top 2 barriers limiting clinicians’ ability to discuss FI with patients. With the increasing number of patients that clinicians are expected to see during clinic, the time to address issues such as FI decreases. Combined with the patient's acute concerns, little time is available for preventive health and other screening.25 In addition, in rural or underserved areas where acute clinical concerns may be increased due to limited access to primary care or burden of health concerns, the ability for clinicians to find time during clinical encounters to discuss FI may be further limited.26
Advances in approaches to patient screening that include computer-based survey tools that can be administered to patients outside of the clinical context on their own time, are promising alternatives for promoting patient satisfaction and managing clinical time constraints.27 Despite the benefits of computer-based screening tools, these tools have the potential to mask FI concerns due to issues such as literacy and language barriers. Research evaluating whether practices with higher screening rates also had social workers for a “warm hand-off” or immediate access to additional support services could help identify strategies for implementation. Despite time-saving approaches to screening which could help identify patients in need, further research is needed to evaluate implementation of FI screening and its impact on specific health outcomes. In addition, it remains important to further develop and evaluate best practices for clinicians on how to efficiently communicate with patients regarding positive screens without adversely affecting the clinician patient relationship.
Limitations
Although this study evaluated the screening practices and obstacles for Family Medicine clinicians in a national CERA survey, several limitations were apparent. The CERA response rate was 25%, which is consistent with many national surveys, but raises concern over respondent bias and generalizability. CERA data are self-reported and subject to bias. The survey reflects the opinions of a sample of academic Family Medicine clinicians nationally and may not be reflective of nonacademic Family Medicine clinicians. In addition, the CERA survey instrument did not ask about the clinician’s health system or referral systems which may provide support for positive FI screens which and could play a significant role in determining whether clinicians see the value in FI screening. Although there is a strong association between FI and poor health outcomes, the impact of FI screenings and best practice responses impacts on health outcomes remains unclear and requires further study.
Conclusions
In conclusion, with FI impacting more than 10% of the US population, and only 6.7% of surveyed clinicians from our survey asking always or frequently about FI, food insecure patients and the accompanying health implications are likely being missed. Understanding FI screening practices and obstacles will offer an opportunity for interventions designed at identifying and addressing FI while increasing knowledge about best patient clinician communication practices to protect patient clinician relationship while impacting patient food security.
Acknowledgments
Authors are grateful for the support of the 2022 Council of Academic Family Medicine’s (CAFM) Educational Research Alliance (CERA).
Appendix
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/37/2/196.full.
- Received for publication August 25, 2023.
- Revision received November 3, 2023.
- Accepted for publication November 13, 2023.




{kind=link}
{kind=link}