
Abstract
Introduction: Unplanned readmissions can be avoided by standardizing and improving the coordination of care after discharge. Telemedicine has been increasingly utilized; however, the quality of this care has not been well studied. Standardized measures can provide an objective comparison of care quality. The purpose of our study was to compare quality performance transitions of care management in the office vs telemedicine.
Methods: The Epic SlicerDicer tool was used to compare the percentage of encounters that were completed via telemedicine (video visits); or via in-person for comparison, Chi-squared tests were used.
Results: A total of 13,891 patients met the inclusion criteria during the study time frame. There were 12,846 patients in the office and 1,048 in the telemedicine cohort. The office readmission rate was 11.9% with 1,533 patients out of 12,846 compared with telemedicine with the rate of readmission at 12.1% with 126 patients out of 1,045 patients. The P-value for the Chi-squared test between the prepandemic and study time frame was 0.15 and 0.95, respectively. Demographic comparability was seen.
Discussion: Our study found a comparable readmission rate between patients seen via in-office and telemedicine for Transitions of Care Management (TCM) encounters. The findings of this study support the growing body of evidence that telemedicine augments quality performance while reducing cost and improving access without negatively impacting HEDIS performance in health care systems.
Conclusion: Telemedicine poses little threat of negatively impacting HEDIS performance and might be as effective as posthospitalization traditional office care transitions of care management.
- Chi-Square Test
- Continuity of Care
- Health Policy
- Hospital Medicine
- Patient Discharge
- Patient Readmission
- Primary Health Care
- Telemedicine
- Transition of Care
Introduction
Hospital readmissions are often preventable events widely believed to reflect poor quality of care. A high rate of patient readmissions may indicate the inadequate quality of care in the hospital and a lack of appropriate postdischarge planning and care coordination.1 Unplanned readmissions are associated with increased mortality and higher health care costs.2⇓⇓–5 Unplanned readmissions can be prevented by standardizing and improving care coordination after discharge and increasing support for patient self-management.2 Effective strategies for reducing unplanned readmission may help improve the quality of care, outcomes, and higher-value care.5 Physician groups can influence unplanned readmission outcomes by appropriate medication reconciliation at discharge, reduction of infection risk, and ensuring proper outpatient follow-up. Telemedicine has historically been utilized to address health care access challenges, especially in areas with limited physician resources or rural settings.7 Telemedicine has also shown other public health benefits, for instance, it can reduce the overutilization of medical facilities by minimizing unnecessary admissions, shorten diagnosis and treatment initiation times, lower the risk of intrahospital infections, and decrease hospital admissions.8 Patient feedback on telemedicine indicates high satisfaction levels, citing convenience, comfort, and reduced costs.9,10
To evaluate the quality of care provided by health care providers and government agencies like CMS and National Committee for Quality Assurance (NCQA), industry-standard measures called Health care Effectiveness Data and Information Sets (HEDIS) are used. These measures are supported by the National Quality Forum (NQF), which comprises of leaders from medical associations to insurance companies and are important for researchers investigating quality performance.2,11,12 The Plan All Cause Readmission (PCR) is readmission rate within 30 days of discharge from an adult acute inpatient or observation stay is a key measure of health care quality. This metric is evaluated for health plan members aged 18 to 64 in commercial and Medicaid plans, as well as those aged 18 and older in Medicare plans. It provides insight into the effectiveness of Transitions of Care Management (TCM), allowing for targeted improvement efforts to improve patient outcomes and reduce health care costs.2
Recent studies have shown that telemedicine is comparable in quality to in-person visits, which suggests that increasing its use in value-based care can positively impact health outcomes and provide various benefits.6 Thus, this study aimed to evaluate telemedicine as a venue for delivering postdischarge follow-up care. The objective of this study was to compare the quality of hospital discharge follow-up visits or TCM Visits between telemedicine and traditional office-based care.
Methodology
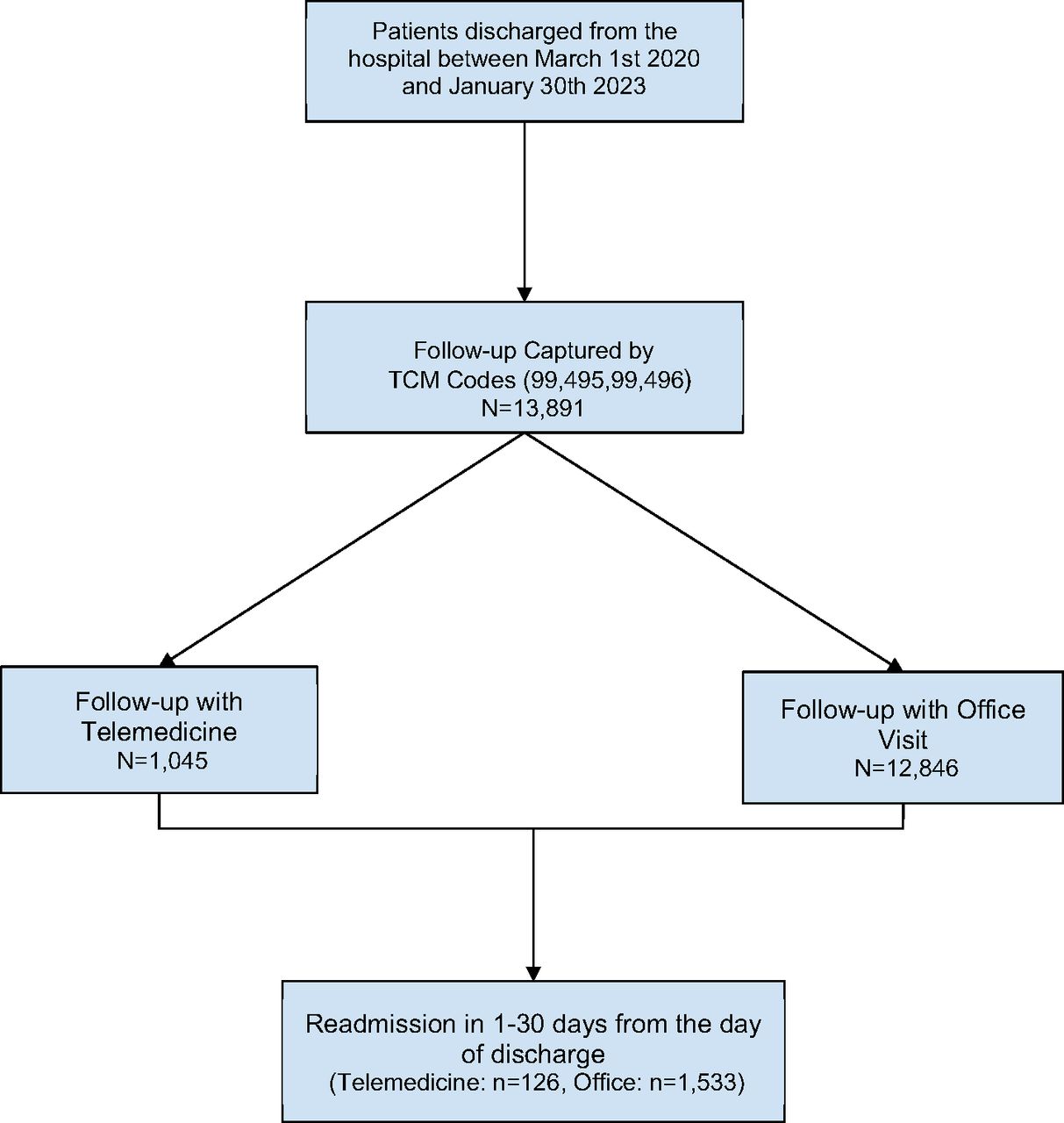
This retrospective cohort analysis was determined to be exempt from full review by the WellSpan Health Institutional Review Board. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) format for cohort studies was followed. The study was conducted in a large, integrated health system spanning central Pennsylvania and northern Maryland (WellSpan Health comprising of 8 hospitals). Data were captured with CPT codes used for TCM (99495, 99496) and the cohort was divided based on mode of follow-up (Telemedicine or In-office visit) (See Figure 1). Deidentified, secondary data were extracted from the electronic medical record (EMR) to compare HEDIS quality performance from March 1, 2020, to January 30, 2023, across more than 200 primary care outpatient care sites between the divided cohort. Epic’s SlicerDicer tool was used to compare the percentage of encounters completed via telemedicine versus in-person visits followed by readmission to the hospital within 30 days. Chi-squared tests determined statistically significant differences between groups. The p-value was set at 0.05.

Schema for selection of study population and cohort divisions. Abbreviations: TCM, transitions of care management.
Multivariable logistic regression controlled for sociodemographic factors, comorbidities, and digital literacy. In this analysis, we considered various factors that could potentially bias or confound results, including the COVID-19 pandemic, age, race, sex, and social determinants of health (SDOH). To account for these factors, we obtained deidentified demographic data that was stratified by age, race, sex, and SDOH. In addition, we utilized an “overall adult risk score” as a measure of overall health risk, which was determined based on multiple diagnoses, SDOH, and health care utilization.6 This risk score is calculated by Epic EHR, although not a validated scoring system as it was created by Wellspan Health, as discussed in our prior publication, “the SDOH component of this overall health risk score included assessment of social risk needs (depression risk, tobacco and alcohol use, violence exposure and social isolation, food or transportation insecurity, and financial strain), providing a more granular risk profiling compared with other standardized scoring systems.”6
To ensure the accuracy of data obtained through SlicerDicer, all the sessions were built with the guidance of the health system’s business intel specialist. In addition, a multi-physician SlicerDicer expert team manually chart reviewed samples of patients from the data set to ensure sequential accuracy and final readmission percentages obtained from the system were comparable to NCQA national readmission rate. To ensure accurate representation of the population over time, we used a quality performance baseline from before the COVID-19 pandemic (January 18, 2018, to February 29, 2020) comparing this to the study time frame. This was done to control for selection bias and assure data consistency.12,13
Results
A total of 13,891 patients met the inclusion criteria during the study time frame. There were 12,846 patients in the office cohort and 1,048 in the Telemedicine cohort. The office readmission rate was 11.9% with 1,533 patients out of 12,846 patients readmitted. The telemedicine readmission rate was 12.1% with 126 of 1,045 patients readmitted.
The prepandemic office readmission rate was 14.1% (1797 of 12,754 patients readmitted) and the telemedicine readmission rate was 10.9. The total number of patients in the prepandemic telemedicine group was relatively small, with 26 of 238 patients readmitted. The P-value for the Chi-squared test between the prepandemic and study time frame was 0.15 and 0.95 respectively. There was demographic comparability between cohorts, by race, ethnicity, legal sex, age, and insurance type. Demographics were consistent for patients in both groups across prepandemic and study timeframes, where comparable percentages were found (Table 1).
Patient Demographics Across Cohorts
Discussion
We found comparable readmission rates between patients seen via in-office and telemedicine for TCM encounters. The most notable finding was the insignificant difference between cohorts which alludes to no significant difference in the quality of this care or comparable quality performance (ie, rates of readmission after a postdischarge follow-up).
In recent years, remote patient monitoring has expanded the capacity of telemedicine further and aids in conducting a detailed evaluation of patient which was previously not possible with the use of sophisticated devices, medical apps and virtual exams led by patients instructed through the examination.14 The findings of this study support the growing body of evidence that telemedicine might augment quality performance while reducing cost and improving access without negatively impacting HEDIS performance in health care systems.6,15⇓–17 This is also in line with a recent data highlight published by CMS where thirty-day readmission rates were lower when there was telehealth follow-up compared with hospitalizations without follow-up visits.18 Another study found that patient’s who had telemedicine appointments had a lower 30-day hospitalization rates compared with in-person appointments.19
As health care broadly moves toward value-based care which focuses on improving patient outcomes while reducing costs across the health systems, practitioners and policy makers alike are recognizing the importance of data and technology in the form of telemedicine in this shift toward value-based care. Use of telemedicine can play a crucial role for TCM and reducing the readmission burden on health systems while keeping in line with the quadruple aim.
Our study is limited. First, it relies on provider accuracy; for example, if a visit did not have a hospital discharge follow-up CPT code, it was not captured. Second, if the patient chose to have a hospital discharge follow-up outside the health care system, it was not captured. We assumed that patients who followed up outside of the 2 week period were not captured by TCM codes in both study groups. Third, there was also a lack of data for the telemedicine group in the prepandemic era, so the baseline comparison was office rates and national readmission rate. The study was conducted during the COVID-19 pandemic which provided a natural ecologic experiment and a factor which cannot be adjusted for but provides starting points for future research. Lastly, the telemedicine sample was small and contained a larger percentage of younger patients between the 2 groups. Larger multisite studies could be performed in the future to replicate results with the intentional use of telemedicine for TCM and provide even stronger evidence for telemedicine quality. In future studies, we could address more granular details on diagnosis by type and venue to understand if there is a correlation with disease type, but this was beyond the scope of our methods and breaches the scope of NQF’s HEDIS measure description.
Conclusion
This cohort study found comparable rates of 30-day readmission for patients with TCM visitors seen via telemedicine versus in-office. This comparable quality performance alludes to the potential suitability of telemedicine as a care venue for hospital discharge follow-up care. Thus, telemedicine poses little threat of negatively impacting HEDIS performance and might be as effective as posthospitalization traditional office care transitions of care management.
Notes
This article was externally peer reviewed.
Funding: No funding was received for this study.
Conflict of interest: The authors have no conflicts of interest to disclose.
To see this article online, please go to: http://jabfm.org/content/37/2/166.full.
- Received for publication June 1, 2023.
- Revision received September 29, 2023.
- Accepted for publication October 9, 2023.




{kind=link}