
Abstract
National telehealth policy thus far has focused on broadening access to service, specialties, and originating sites. Yet telehealth policy can further equity by providing system-level change needed to reduce structural determinants that hamper telehealth access in historically marginalized, low income, and limited English-speaking populations. The authors propose policy solutions for states and CMS to help address these structural determinants of telehealth care. A telehealth “ecosystem” grounded in the following core components would ensure equitable access to care: use of technology inclusive of economically marginalized patients, access to the technology and broadband for completing virtual visits, and concrete support for patients as they develop their digital and telehealth skills.
- COVID-19
- Digital Divide
- Health Policy
- Health Services Accessibility
- Healthcare Disparities
- Minority Health
- Telemedicine
- Underserved Populations
Introduction
During the COVID-19 pandemic, the use of telehealth has grown rapidly, with various policies setting the stage for its expansion.1 Expanding telehealth nationally has created opportunities to bridge gaps in access to health care among underserved patients. Although telemedicine and telehealth policies to date have focused largely on reimbursement problems that predate the pandemic, as states now delve into postpandemic telehealth policy, priorities can shift toward changing system-level determinants that limit economically marginalized patients' access to care. Equity in telehealth primary care occurs when system infrastructure meets the patients at their technological capacity,2 and helps strengthen access to the system.
Current Trends in US Telehealth Policy
Currently, each state has its own definition of telemedicine/telehealth.3,4 State policies currently focus on designating services, professionals, and settings through which telemedicine is reimbursable.3 What is reimbursed, and how, varies widely across states.4 As of May 2020, all state Medicaid programs allow primary care services to be delivered via telemedicine, and 31 states also allow maternity services.5 As of September 2021, eighteen allow telephone reimbursement.3
On November 2, 2021, the Centers for Medicare & Medicaid Services (CMS) announced policy changes for Medicare payments and required that certain services, including behavioral health care services, be added to Medicare telehealth services through December 31, 2023; additional time was given to evaluate if those services should be retained permanently.6 As Medicare works to expand telecommunication technologies beyond geographic and specialty barriers, however, policies also must address ongoing structural barriers to access.
During the COVID-19 pandemic, members of our safety-net family medicine team received comments from our low income, limited English proficiency (LEP) patients about their not always successful attempts to use telehealth services. We here synthesize our experiences with these urban, underserved, under-resourced, and ethnically diverse patients, to help inform policy solutions addressing various structural determinants of telehealth care mentioned by our patients.
Equity in Telemedicine: Areas of Success
Care at a distance has reduced transportation barriers and barriers such as having to take time off from work for appointments.7,8 This is particularly important for working-class patients who may not have sick day privileges and thus risk their jobs if they miss work. Telehealth thus also provides some convenient touchpoints that complement chronic care management in the traditional in-person setting.
In addition, using technology patients already have, such as smartphones, helps fill technology gaps in under-resourced communities.2 While not all patient portal platforms are compatible with smartphone use,9 phone visits can still be conducted using this technology, to help bridge access gaps among the most underserved.2,9,10 Yet not all states or payers currently reimburse for phone visits, making this mode of communication not feasible for many.4
Philanthropic entities have partly augmented federal investments to provide technology, hotspots, and infrastructure, including support staff.11 There is increasing recognition that telehealth “navigators” are vital to enhancing the use, accessibility, and efficacy of telehealth,11,12 and policy makers have an opportunity to endorse their use.
Equity in Telemedicine: Areas for Improvement
Despite these successes, many occasions remain for meeting patients' needs, from the standpoint of equity. The most underserved and under-resourced patients have limited access to computers and smartphones.13 Older devices are not always capable of running the newer software that many telemedicine systems require. In 1 study of FQHCs, 48.5% of primary care visits during the pandemic study period occurred via telephone, while only 3.4% occurred via video.14 Technological barriers low-income patients face likely resulted in phone visits occurring over 14 times more frequently than video visits, in this sample. This is a clear call for improvement in this area.
Even when patients have appropriate devices, limited experience with computers and required software (sometimes called “limited digital literacy”) is a barrier for many.15 Expanding digital skills training would help patients learn to use existing portals.16,17 Moreover, telemedicine efforts can be increased by using communication applications that patients already use, such as WhatsApp, whose widespread presence offers a means of addressing accessibility as a structural determinant of telehealth care.2,18
Currently, telehealth platforms mostly are English-only, which does not meet the diverse language needs of LEP patients.19 For patients needing video interpretation services, setting up video connection with an interpreter may pose an added barrier.16
Another challenge for low-income patients and telemedicine is lack of access to private space for virtual visits.20 Low-income patients may live in close quarters with other people, or may be unhoused and have no private space for a telemedicine visit. Such patients have little protection of their rights to privacy and confidentiality.
These patients often have limited home broadband access, which poses another challenge to access.20 If a patient does not have reliable internet, they may not have a fair experience with their provider; their visit may be truncated or otherwise unsuccessful, causing frustration and delays in care. We propose the following policy solutions for states and CMS to consider to help address these structural determinants of telehealth care.
Recommendations
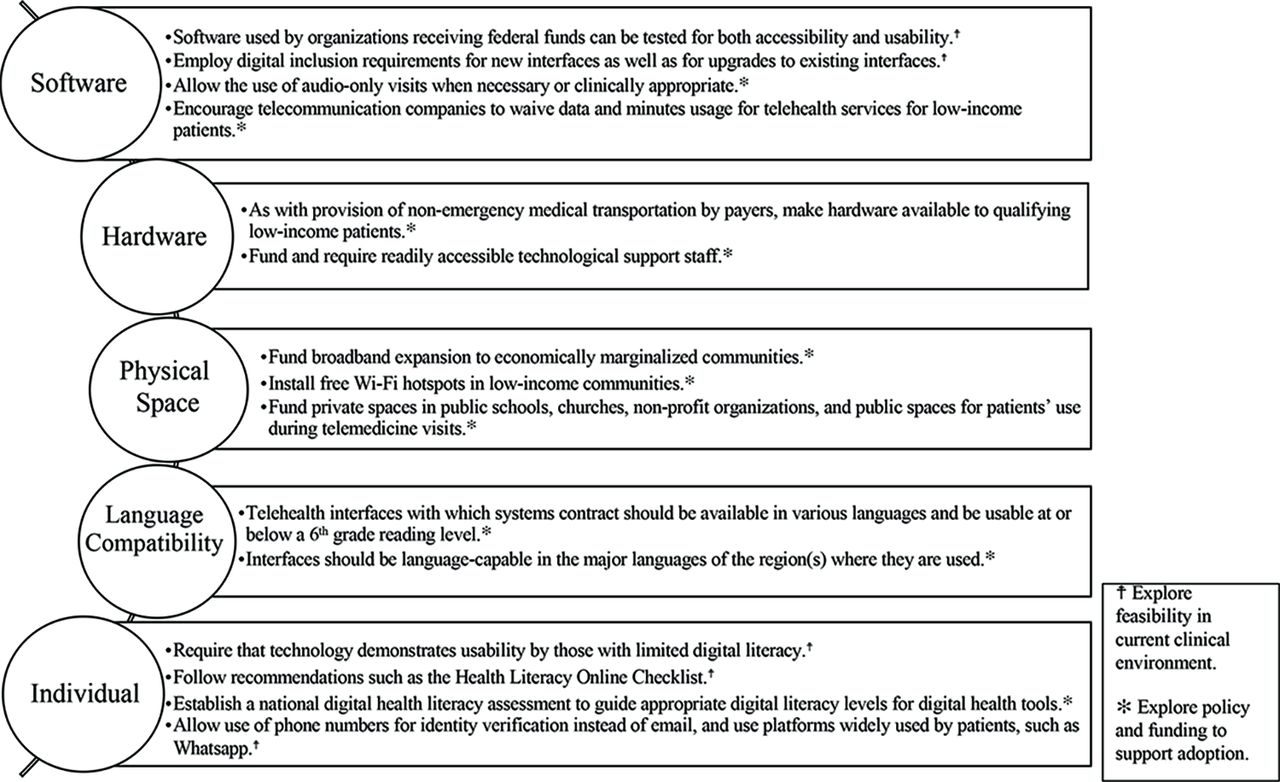
Building a telehealth “ecosystem” providing equitable access to care requires employing inclusive technology, ensuring equitable access to the necessary technology and broadband, and supporting patients as they learn to use telehealth systems. Based on these components, we offer these recommendations for national and state policy consideration (Figure 1):
Funding for upgrades, ongoing telehealth system investment, and modernization could require health system technology to be inclusive of, and demonstrate usability by, historically marginalized patients and those with limited digital literacy. Strategies include:
Software used by organizations receiving federal funds can be tested for accessibility and usability. This testing should prioritize and include groups experiencing disadvantages in using current telehealth systems. Telehealth accessible to patients experiencing barriers will also be inclusive of those not experiencing them.18
Telehealth interfaces employed in safety-net clinics should demonstrate that they are user-friendly to the patients they serve. This applies to both new interfaces and upgrades to existing interfaces. Patient advisory committees could be a means to perform the testing.
Organizations receiving federal funds should follow recommendations for user-friendly digital health tools, such as Health Literacy Online, by the Office of Disease Prevention and Health Promotion.
Where telehealth systems do not demonstrate accessibility and usability by digitally marginalized and under-resourced communities, health care systems can employ platforms, media, and practices their patients already use widely. For example, policy can facilitate using a phone number instead of email for registration and identity verification, or using links via text messages or end-to-end encrypted video calls via applications not allowed before the pandemic, such as WhatsApp.
Telehealth interfaces with which systems contract should be available in various languages, and be usable at or below a sixth-grade reading level.
Software developers can be required and incentivized to provide multilingual technology, so that interfaces are language-capable in the major languages of the region(s) where they are used. Such technology might include website capacity to switch languages in real time, as the CDC website does, among others.
The National Assessment of Adult Literacy could be updated to include a digital health literacy assessment, to guide appropriate digital literacy levels for telehealth and digital health tools.
Hardware access can be handled similarly to provision of non-emergency medical transportation by payers, and made available to qualifying low-income patients to enable digital access to appointments.2,21
Broadband expansion and digital infrastructure must reach economically marginalized communities. Strategies include:
Free Wi-Fi hotspots providing internet access with speed sufficient to maintain a successful video visit.
Encouraging telecommunication companies to waive data and minutes usage for telehealth services for low-income patients.
Readily accessible technological support staff can be required by policy and funded at the federal, state, and payer levels.
Such support staff should be available to help new patients prepare for video visits, while patients are learning to use patient portals, and during all video visits, should problems arise.
Audio-only visits should be supported when necessary and clinically appropriate.
Payment for and coverage of audio-only visits should be ensured when video capacity is not an option.2 Prioritizing software and hardware access, as described above, will make telephone visits instead of video encounters the exception, used only when appropriate and while telehealth equity infrastructure is built.
Private spaces in public schools, churches, non-profit organizations, and public spaces could be funded for patients' use during telemedicine visits. Strategies include.
Designating private areas in trusted spaces in their communities for patients to use.
Creating private areas in shelters for unhoused individuals to conduct telemedicine visits.

Policy Recommendations to Steer Telehealth Toward Equity.
Conclusions
Telehealth policy has focused thus far on broadening specialty and service access and allowable originating sites. As policy makers look to the future, beyond these needs, they can steer telehealth toward equity by providing system-level change to dismantle structural barriers limiting telehealth access in historically marginalized and low-income populations. While clinics' and primary care physicians' resources may be limited, policy makers and payers can enable the above strategies through various means. Together, we can ground our telehealth “ecosystem” in equity going forward.
Acknowledgments
The authors would like to thank Seira Santizo Greenwood, Chief of Staff of the Center for the Study of Latino Health and Culture (CESLAC), for her instrumental support, without whom this manuscript would not have been possible, and Cynthia L. Chamberlin, CESLAC historian, for her editorial assistance.
Notes
This article was externally peer reviewed.
Funding/support: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/35/3/588.full.
- Received for publication December 16, 2021.
- Revision received March 7, 2022.
- Accepted for publication March 8, 2022.





{kind=link}