
Abstract
Purpose: This study assessed the prevalence of loneliness, burnout, and depressive symptoms from a national sample of family medicine physicians.
Methods: We conducted a cross-sectional survey of 401 physicians who were members of the American Academy of Family Physicians (AAFP) and AAFP National Research Network between December 7, 2019, and January 20, 2020. The study participants completed an anonymous, 30-item survey measuring loneliness, burnout, symptoms of depression, fatigue, in addition to providing demographic information.
Results: The response rates were 16.3% (401 of 2456) for all the physicians, 7.0% (113 of 1606) for the AAFP NRN member physicians, and 33.9% (288 of 850) for the AAFP member insight physicians. The prevalence of loneliness, burnout, and depressive symptoms was 44.9% (165 of 367), 45.1% (181 of 401), and 44.3% (163 of 368) respectively. The physicians who experienced a greater feeling of loneliness compared with those who experienced a lesser feeling of loneliness were more likely to report at least 1 manifestation of burnout (69.1% vs 27.4%, P < .01), screen positive for depression (66.0% vs 27.6%, P < .01), and experience a higher degree of fatigue (59.5% vs 32.4%, P < .01). Depressive symptoms (odds ratio [OR] = 5.08; 95% confidence interval [CI], 4.64-7.94; P < .001), overwhelming exhaustion (OR = 7.19; 95% CI, 4.03 to 12.02; P < .001), and burnout (OR = 4.61; 95% CI, 2.96-7.19; P < .001) were associated with loneliness status.
Conclusion: Our findings demonstrate that loneliness is common in practicing family medicine physicians and is significantly associated with burnout and depression. Future work is needed to understand the various interactions and relationships among loneliness, burnout, and depression to help inform effective interventions.
- Burnout
- Cross-Sectional Studies
- Depression
- Family Medicine
- Family Physicians
- Loneliness
- Mental Health
- Occupational Burnout
- Prevalence
- Primary Care
- Primary Health Care
- Surveys and Questionnaires
Introduction
Loneliness, defined as the internal perception of inadequate personal relationships,1 poses a significant health concern. Loneliness is associated with a variety of negative physical and mental health conditions, such as hypertension, cardiovascular disease, stroke, depression, suicide, and even death.2⇓–4 The prevalence of loneliness has been cited as high as 35% in US adults above 45 years old.5 Given these concerns, leaders in the field have called for loneliness to be deemed a public health priority in the United States.6
As a state of emotional discomfort, loneliness likely is related to other conditions of psychological distress such as burnout. Literature supports that over 50% of physicians experience symptoms of burnout, such as emotional exhaustion, cynicism, and reduced professional efficiency.7⇓–9 Burnout among health care providers is associated with increased medical errors,10,11 dishonest clinical behaviors,12 lower patient satisfaction,13,14 and greater job turnover.15 Similar to loneliness, burnout has been called a public health crisis in the United States.16
While there is literature that contributes to our understanding of burnout in health care providers, less is known about loneliness experienced by physicians and the relationship between loneliness and burnout. Loneliness is thought to be prevalent among physicians, with a Harvard Business Review study illustrating that those with professional degrees, such as physicians, have the highest rates of loneliness among all professions.17 Previous research in a sample of physicians in Kansas illustrated that the prevalence of loneliness was 43% among respondents.18 While loneliness has been linked to physician burnout,18⇓⇓⇓–22 this has not been demonstrated in a national sample of practicing physicians.
Given the known individual and systematic impacts of physician psychological distress, in addition to the relationship between physician well-being and quality of care,23 it is important to learn about emotional stress experienced by physicians. A greater understanding of the national experience of physician loneliness, burnout, and other forms of emotional distress would allow for a more informed and generalizable discussion about individual and organizational approaches to mitigate negative impacts. This study aimed to assess the prevalence of loneliness, burnout, and depressive symptoms from a national sample of family medicine physicians.
Methods
Study Design and Participants
The study was a cross-sectional survey of physicians who were members of the American Academy of Family Physicians (AAFP) and AAFP National Research Network (NRN) between December 7, 2019, and January 20, 2020. The study participants (n = 401) completed an anonymous, 30-item survey that included questions regarding loneliness, burnout, symptoms of depression, fatigue, in addition to personal demographic information. The survey link was emailed to all members of the AAFP NRN and the AAFP Member Insight Exchange, a subset of AAFP members who agree to be contacted for surveys. The AAFP Institutional Review Board gave this study exempt status on review.
Table 1 presents the demographic information of the respondents. The mean age of respondents was 50.2 years (standard deviation [SD] = 11.1). A slight majority were female (53.1%), most were employed full-time (84.4%), worked in urban areas (85.0%), and were members of AAFP Member Insight Exchange (71.8%). The mean years in clinical practice among the physicians was 18.9 years (SD = 11.3).
Respondents' Characteristics, (n = 401)
Study Instruments
Loneliness
We assessed the physicians' level of loneliness using a 3-item University of California, Los Angeles (UCLA) Loneliness Scale, a validated shortened screening tool to measure loneliness.24,25 The questions are: How often do you feel that you lack companionship? How often do you feel left out? How often do you feel isolated from others? Participants recorded their responses on a 3-point Likert-like scale (1 = Hardly ever, 2 = Sometimes, and 3 = Often). Scores for the 3 questions were summed, with a possible score ranging from 3 to 9. As a standard practice,25,26 respondents who had a total score of 6 or above were considered “lonely.”
Burnout
Assessment of burnout among the respondents used 2 single-item measures of overwhelming exhaustion and depersonalization adapted from the full Maslach Burnout Inventory (MBI-22), which has been validated.27 The overwhelming exhaustion item (“I feel burnout from my work”) and depersonalization item (“I've become more callous toward people since I became a physician”) have been shown to be useful screening questions for burnout.28⇓–30 These 2 items have shown the highest factor loading27,31,32 and strong correlation28,33 with their respective emotional exhaustion and depersonalization domains in the MBI-22.28 The 2 single items have been used in previous studies to measure manifestations of burnout among physicians.8,34⇓–36 The respondents recorded the degree to which each item applied to them on a 7-point Likert-like scale (0 = Never, 6 = Every day). The scores of each domain were grouped into low, moderate, and high burnout categories using established cutoffs.8,27,34,36 Higher scores are indicative of greater exhaustion and depersonalization, and greater burnout. Consistent with convention,8,34,36 we considered respondents who scored high (score of greater than 3) on exhaustion and/or depersonalization domains as having at least 1 manifestation of professional burnout.
Symptoms of Depression and Fatigue
We screened for symptoms of depression using a 2-item Primary Care Evaluation of Mental Disorders Patient Health depression-screening questionnaire (PHQ-2). The questions asked the participants about their feelings of being down, depressed, or hopeless and if they have been bothered by little interest or pleasure in usual activities during the past month. The 2-question screener has a reported 96% sensitivity and 57% specificity for depression.37,38 The PHQ-2 is an accurate depression screening in adults and used in previous studies to screen for symptoms of depression among physicians.18,30,39⇓–41
We measured the physicians' levels of fatigue during the past week using a standardized linear analog scale (0 = as bad as it can be, to 10 = as good as it can be) similar to what is described by West and colleagues.42 Respondents who scored 5 or less on the scale were considered to have higher levels of fatigue.30,34,39
Statistical Analyses
Standard descriptive statistics were used to create a demographic profile and describe the prevalence of loneliness, burnout, depression, and fatigue among the respondents. Mann-Whitney U test/independent samples t-test and/or Kruskal-Wallis test/1-way ANOVA (for continuous variables), and Likelihood Ratio Chi-square (for categorical variables) were used to evaluate the association between variables. Generalized linear mixed models were used to calculate associations between the loneliness classification modeled as a binary outcome against a single fixed effect for independent variables (age, gender, employment status [whether a participant is employed part-time, full-time, fully retired, or not in the workforce for other reasons], practice location, membership [AAFP Member Insight Exchange and AAFP NRN], depression, emotional exhaustion, depersonalization, and fatigue).
Adjusted odds ratios were estimated by modeling all significant independent variables against the loneliness classification, controlling for respondent age, gender, employment status, practice location, and membership. Adequate power (>0.85) to detect significant relationships among the variables with 2 degrees of freedom, P < .05, and 0.21 effect size required a sample size of 350 respondents.43,44 All analyses were 2-sided with α of 0.05. The IBM SPSS (Statistical Package for the Social Sciences; Armonk, NY), version 26 was used for these analyses.
Results
The response rates were 16.3% (401 of 2456) for all the physicians, 7.0% (113 of 1606) for the AAFP NRN member physicians, and 33.9% (288 of 850) for the AAFP member insight physicians. There was a 4.5% margin of error at a 95% confidence level between the study sample and the overall physicians who were members of the AAFP population, demonstrating that our sample generally represented the overall AAFP population.45 Table 2 summarizes the prevalence of loneliness, burnout, depression, and fatigue. Throughout the document, we used the term depression to indicate a positive screen for depressive symptoms.
Loneliness, Burnout, Depression, and Fatigue Among Physicians Who Participated in the Study, (n = 401)
Loneliness
The overall prevalence of loneliness was 44.9% (165 of 367). The mean score and standard deviation on the 3-item UCLA Loneliness Scale was 5.3 ± 1.9, with more than half of the physicians sometimes or often feeling a lack of companionship, left out, or isolated from others (Figure 1).The mean loneliness score varied by gender, with female respondents scoring higher (5.6 ± 1.9) than male respondents (5.1 ± 1.9, P = .012; Table 2). As Table 3 shows, loneliness was significantly associated with years in clinical practice. Physicians with more years in practice had lower levels of loneliness (P = .019). There was not a significant association between age-group, gender, employment status, practice location, or membership and loneliness score.
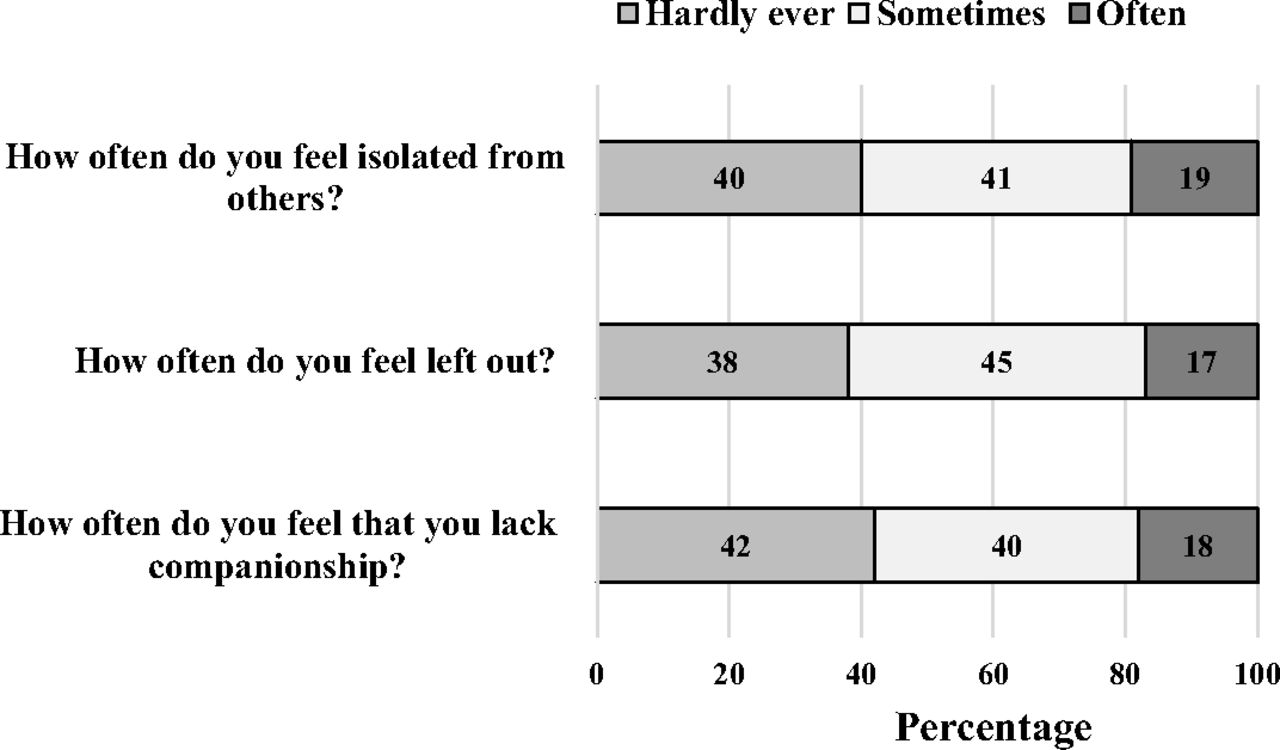
Percentage of responses to the 3-item University of California, Los Angeles (UCLA) Loneliness Scale
Odds Ratios for Independent Variables and Loneliness, (n = 401)
Burnout
In aggregate, 45.1% of the physicians reported at least 1 manifestation of burnout. The manifestation of burnout varied by sex, with 56.9% of female respondents compared with 41.7% of male respondents reporting manifestations of burnout (P = .004).
Depression and Fatigue
Overall, 44.3% (163 of 368) of the respondents screened positive for depression. Depression by sex, with 51.0% (100 of 196) of female respondents versus 36.8% (63 of 171) of male respondents screening positive (P = .004). Nearly 46.9% (161 of 343) of the respondents reported excessive fatigue during the prior week. The level of fatigue varied by sex as 55.2% (101 of 183) of the female respondents compared with 36.9% (58 of 157) of the male respondents reported experiencing excessive fatigue during the prior week (P < .001).
Loneliness and Other Types of Emotional Distress
As shown in Table 4, respondents with higher loneliness scores reported at least 1 manifestation of burnout (69.1% vs 27.4%, P < .01), were more likely to screen positive for depression (66.0% vs 27.6%, P < .01) and experienced a higher degree of fatigue (59.5% vs 32.4%, P < .01).
Relationship of Burnout, Depression, and Fatigue with Loneliness Among the Physicians
Findings of the mixed model analyses indicated that there was a significant positive association between loneliness and depression (odds ratio [OR] = 5.08; 95% confidence interval [CI], 4.64-7.94; P < .001; Table 3). This association remained significant after adjusting for the respondent age, gender, employment status, practice location, and membership (adjusted OR [aOR] = 2.24; 95% CI, 0.97-5.19; P < .001). In addition, respondents who reported a high level of overwhelming exhaustion experienced a higher level of loneliness (OR = 7.19; 95% CI, 4.03-12.02; P < .001; Table 3). This association remained significant after adjusting for all respondent characteristics (aOR = 1.26; 95% CI, 0.99-1.61; P < .01).
A higher level of loneliness associated positively with manifestations of burnout (OR = 4.61; 95% CI, 2.96-7.19; P < .001; Table 3), high score of depersonalization (OR = 4.76; 95% CI, 2.58-8.77; P < .001; Table 3), and a high degree of fatigue (OR = 4.63; 95% CI, 1.91-7.63; P < .001). These associations were not significant after adjusting for the respondent's age, gender, employment status, practice location, and membership.
Discussion
While previous research has investigated physician burnout and physician depression, this cross-sectional survey is one of the first studies to also look at physician loneliness and its associations with other forms of emotional distress. In this study, 44.9% of a national sample of family medicine physicians identified as lonely. The prevalence of depression and burnout was 44.3% and 45.1%, respectively. Physicians who experienced a greater feeling of loneliness were more likely to report at least 1 manifestation of burnout, screen positive for depression, and experience a higher degree of fatigue than those who experienced a lesser feeling of loneliness. The associations between loneliness and depression in addition to loneliness and exhaustion remained significant after adjusting for the respondents' age, gender, employment status, practice location, and membership.
The high prevalence of loneliness in this national sample of family medicine physicians and the association with both depression and burnout mirrors results from a prior study assessing Kansas family physicians.18 In addition, our high depression and burnout prevalence rates are in line with findings of previous studies.18,34,39,46 Family medicine physicians typically spend their days interacting with other health care professionals, staff, and patients; however, our results demonstrate that loneliness and emotional distress can occur even in clinical environments. Family medicine physicians often have to cope with substantial administrative and regulatory burdens.47 Such tasks may be adversely affecting their ability to interact with colleagues in meaningful ways and could potentially be leading to loneliness.19,48 Instead of focusing on developing meaningful clinical relationships with patients, physicians may be becoming more focused on “clicking the boxes,” and documentation due to increased government regulation, malpractice suits, and health system demands. Further exploration of the factors influencing the loneliness and emotional distress among family medicine physicians may reveal additional or different contributing factors and thus inform interventions. Although we captured perceived social isolation in this study, other authors have suggested that there are also structural and professional components to isolation, illustrating the potential multi-factorial effect of the workplace environment.19,49
Loneliness and depression are known to be associated in the general population,50 though loneliness and burnout are correlated in certain populations, such as medical residents.21,22 To our knowledge, this is the first study illustrating a relationship of loneliness to both depression and burnout in a national sample of physicians. Although loneliness, burnout (overwhelming exhaustion), and depression are overlapping constructs of helplessness, these states of emotional distress seem to be distinct phenomena,51 where loneliness is due to unmet social needs, burnout is a negative work-related state of mind, and depression is a sadness that may impact all areas of someone's life. There is a paucity of research on the temporal relation between loneliness and burnout, although other authors have suggested that loneliness may increase vulnerability to environmental stressors leading to burnout and that social networks and relationships may help mitigate the negative impacts of burnout.21,22 In support of this, one study illustrated that lower levels of social capital were associated with decreased academic performance in minority medical students,52 highlighting the importance of social ties in a health care context.
Physician loneliness was not associated with practice location or employment status. Our results corroborate other studies that have not documented a significant difference in loneliness between respondents in rural and urban settings.53⇓–55 Generalizability of our findings may be somewhat limited, as 85% of the respondents practiced in urban settings. While social and professional isolation may be more common in rural practice settings, structural isolation can occur in any practice setting.49
While age was not associated with loneliness scores, physicians with additional years of practice were less likely to consider themselves lonely. Previous literature on other forms of physician emotional distress suggests that burnout and depression begin early in the medical career and increase throughout training;34,56 our results illustrate that this may also be the case for loneliness. The reasons for this are not clear, but we hypothesize that physicians who are more established in their clinical settings have had more time to develop meaningful relationships within physician groups and in their community. It may also be that younger physicians, accustomed to working in groups during the training, are assigned into practice settings where there are fewer professional interactions, which in turn contributes to isolation.57 Notably, this trend of younger persons suffering more loneliness is also illustrated in the general population, which suggests the potential contribution of external factors such as increased societal fragmentation, concerns with self-identity, and significant life transitions.1,58,59
Overall, our data highlight the urgent need to examine the underlying causes and components of physician loneliness to inform interventions that elevate physician wellbeing. Although there is significant attention on physician burnout, our results illustrate that the current narrative on physician unhappiness must expand to include loneliness.60 As other authors have noted, there are likely 3 types of isolation contributing to physician distress: professional, structural, and social isolation.49 The increasing fragmentation of medicine and “disconnected workplace” for family medicine physicians may result in structural and professional isolation, while difficulty making and sustaining meaningful relationships with patients and colleagues may contribute to social isolation.19,48 These multi-level factors must all be considered in future organizational and individual strategies to reduce loneliness among physicians. In addition, our results endorse the need to better understand loneliness in younger family medicine physicians, potentially involving solutions such as curricular changes that mitigate emotional distress in training physicians.61
Study Limitations
There were some limitations to the study given the cross-sectional nature and low response rate. Response rates were typical of surveys8,9,18,39,46 but were lower in the AAFP NRN members. The lower response rate for AAFP NRN members may have been because compensation was not provided for this survey; when compensated, the response rates tend to be in the more typical range for AAFP NRN members.62,63 The low participation rate likely contributes to some non-responder bias that could affect the interpretation of the results. Emotionally distressed physicians may be less motivated to respond to the survey, or more likely to participate because the topic may be relevant to them. Given the anonymous nature of the survey that was emailed to members of the AAFP NRN and AAFP Member Insight Exchange, which are not necessarily mutually exclusive groups, we are unable to account for any double-counting of responses. In addition, while we found correlations among loneliness, depression, and physician burnout, we are unable to determine which of these factors if any, leads to the other two. However, prior literature has shown that loneliness predicts depressive symptomatology, even after controlling for objective social isolation, stress, and social support.50 While this study was unable to ascertain the reasons for physician loneliness, further research should explore these root causes, which could help drive practice changes and inform interventions focused on physician wellbeing. In addition, future research should focus on longitudinal monitoring of younger physicians to determine which factor represents a tipping point for the others or if they co-occur.
Conclusion
The prevalence of loneliness in practicing family medicine physicians is high and is significantly associated with burnout and depression. Our findings contribute to the growing body of evidence demonstrating the disproportionate amount of emotional distress experienced by physicians. In response, health care systems, employers, and payers need to prioritize understanding and addressing the factors relating to physician wellbeing. Future research ought to study the temporal relationship between loneliness, burnout, depression, and the factors related to the manifestation of these conditions to inform effective interventions.
Notes
This article was externally peer reviewed.
Funding: None.
Conflicts of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/3/531.full.
- Received for publication October 28, 2020.
- Revision received January 16, 2021.
- Accepted for publication January 18, 2021.




{kind=link}