
Abstract
Objective: To provide a potential biological, mechanistic link for the well-established association between primary care access and reduced mortality, this study sought to measure the impact of having a usual source of health care on leukocyte telomere length (LTL).
Data Sources: Our study population included 3202 participants aged 50 to 84 years from National Health and Nutrition Examination Survey 1999 to 2001.
Study Design: Cross-sectional Study. LTLs between people with and without a usual source of care were compared using unadjusted and adjusted linear regression models. Fully adjusted models accounted for demographic characteristics, health conditions, and health behaviors.
Principal Findings: After controlling for individual factors, health conditions, and health behaviors, people who had a usual source of health care had significantly longer LTL (β = 89.8 base pairs, P-value = .005) compared with those without a usual source of care; corresponding to approximately 7 years of life.
Conclusions: Having a usual source of health care is associated with longer LTL among older adults. This study provides a potential biologic link for the noted association between primary care access and reduced mortality that has been observed at the individual and population level.
- Aging
- Cross-Sectional Studies
- Healthy Aging
- Leukocytes
- Linear Models
- Nutrition Surveys
- Primary Health Care
- Telomere
Introduction
Continuity of care is a key function of primary care that has been associated with a myriad of favorable health outcomes including better self-rated health, improved therapeutic response, improved adherence to treatment, lower costs, and more favorable health care utilization patterns.1⇓⇓–4 A recent systematic review concluded that continuity of care was associated with reductions of mortality.5 Despite these clear benefits, continuity of care is declining in the United States.6 Having a usual source of care, defined as having a regular place to seek health care when needed, has been used as a marker for primary care continuity and access in the health services research literature.7⇓⇓–10
Although the evidence for continuity is robust, the mechanism by which human factors in health care, like the doctor-patient relationship, impact broad physical health outcomes like mortality remains uncertain. Hypotheses to date focus on the increased opportunities for preventive health care,8 increased physician knowledge, and better adherence to treatment regimens for chronic conditions.11 However, there has yet to be a clear biologic link that provides a mechanism to explain the association between having a usual source of primary care and reduced mortality.
One possible biologic link between the observed association between access to primary care and reduced mortality is telomere length. Telomeres are repeating noncoding repeats of the nucleotides (TTAGGG) at the end of chromosomes that promote stability of the chromosome and impact its ability to replicate.12 Telomere length shortens with each cell replication and when shortened to a critical point, causes a cell to enter senescence.13,14 Telomere length has been identified as a useful biomarker for aging and chronic stress.15,16 The National Health and Nutrition Examination Survey (NHANES) made data for telomere length of respondents publicly available in 2014 for the years 1999 to 2000 and 2001 to 2002.
This data release enabled us to examine the association between having a usual source of health care and telomere length in a nationally representative sample of older adults. This is the first analysis that measures the impact of having a usual source of health care on a biologic marker of aging and provides a potential biological mechanism for the well-established association between continuity of care and reduced mortality on both the individual and ecologic level.
Methods
Data Source
NHANES is a cross-sectional survey conducted and managed by Centers for Disease Control and Prevention. NHANES employs a multistage, complex, stratified probability sampling design and oversamples specific segments of the population including racial minorities and lower socioeconomic status individuals.17 Measurement of telomere length was performed for 1999 to 2000 and 2001 to 2002 NHANES cycles, and telomere data became publicly available in 2014. During this 4-year period, 10,291 NHANES participants aged 20 years and older were asked to provided DNA sample, and 7827 participants provided a valid DNA sample.
We included participants from NHANES 1999 to 2002 cycles who were 50 to 84 years old and had complete data for the variables in our study, including telomere length, usual source of health care, age, sex, race, education level, cardiovascular disease (CVD) history, emphysema history, hypertension history, smoking status, and physical activity.
Measurement
The outcome variable was leukocyte telomere length, and the exposure variable was usual source of care. There were 9 potential confounding variables that included sex, age, race, education level, health insurance coverage, CVD history, emphysema history, high blood pressure history, smoking status, and physical inactivity. Selection of these variables was guided by previously noted associations in the literature.18 Other covariates we explored in our analysis that were not included in final models due to lack of significance (after baseline adjustment for age, age squared, and white blood cell [WBC] count) included income to poverty ratio, body mass index, asthma history, any liver condition history, chronic bronchitis history, cancer or malignancy history, diabetes history, high cholesterol history, and alcohol consumption.
Leukocyte Telomere Length
DNA was extracted from whole blood samples and leukocyte telomere length (LTL) assayed using polymerase chain reaction (PCR). Telomere length was measured relative to standard reference DNA (T/S ratio). Each sample was assayed 3 times on 3 different days and mean calculated. T/S ratio was converted to base pairs (BP) using the following formula: BP = 3274 + 2413 * (T/S ratio). More details of the telomere length assay performed for the NHANES samples is described in detail elsewhere.18⇓–20
Usual Source of Care
We used the NHANES questionnaire on hospital utilization and access to care to determine whether a participant had usual source of care or not. Participants who answered, “Yes”/“There is more than 1 place” to the question, “Is there a place that you usually go when you are sick or need advice about your health” and answered, “Clinic or health center”/“Doctor’s office or HMO” to the question, “What kind of place do you go to most often: is it a clinic, doctor’s office, emergency department, or some other place” at the same time were identified as “having usual source of care”; those who answered, “There is no place” to the question, “Is there a place that you usually go when you are sick or need advice about your health” were identified as “having no usual source of care.” Participants with other answers to the 2 questions above were excluded.
Covariates
All information on covariates was derived from the NHANES questionnaire. Age was treated as a continuous variable. Sex was categorized as Male or Female. We categorized race/ethnicity into 4 categories: Non-Hispanic White, Non-Hispanic Black, Mexican American and Hispanic, and other races. Education level was defined as “Less than High School,” “High School Graduates/GED or Equivalent,” “Some College or AA degree” and “College Graduate or above.” Health insurance coverage was determined by participant’s answer to the question, “Are you covered by health insurance or some other kind of health care plan.” History of emphysema was determined by participant’s answer to the question, “Has a doctor or other health professional ever told you that you had emphysema.” History of high blood pressure was assessed by a similarly worded question. Participants were identified as having history of CVD if they answered “Yes” to any of the 5 questions asking about history of congestive heart failure, coronary heart disease, angina/angina pectoris, heart attack, and stroke.
Smoking status was categorized in 3 levels: current smoker, former smoker and never smoked. Participants who answered “No” to the question, “Have you smoked at least 100 cigarettes in your entire life” were identified as “Never Smoked;” those who answered “Yes” to the question, “Have you smoked at least 100 cigarettes in your entire life” and answered “Every day” or “Some days” to the question, “Do you now smoke cigarettes” were defined as “Current Smoker;” those who answered “Yes” to the question, “Have you smoked at least 100 cigarettes in your entire life” and answered “Not at all” to the question, “Do you now smoke cigarettes” were defined as “Former Smoker.”
Participants who answered “No” or “Unable to do activity” to both the questions, “Over the past 30 days, did you do any vigorous activities for at least 10 minutes that caused heavy sweating, or large increases in breathing or heart rate” and “Over the past 30 days, did you do moderate activities for at least 10 minutes that cause only light sweating or a slight to moderate increase in breathing or heart rate” were identified as having physical inactivity; and those who answered “Yes” to either of the questions above were defined as not having physical inactivity.
Statistical Analysis
According to NHANES protocols, data were weighted, and primary sampling unit and stratum were accounted for in the analysis. Sample weights used for the present study were based on 4 years of mobile examination center records. To compare categorical characteristics between participants who had a usual source of care and those who had not, SAS (SAS Institute, Cary, NC) SurveyFreq procedure was utilized to generate unweighted numbers, weighted proportions, and P-values for c2 tests. SAS SurveyMeans procedure was used to compare Age and Telomere Length between 2 exposure groups with weighted means, standard deviation, and P-values for t-test presented. The bivariate associations between telomere length with exposure and covariates were assessed using bivariate linear regression. We also examined the effect of exposure and covariates on telomere length adjusting for age, age squared, and WBC count. We adjusted for WBC count because the dependent variable in the models is LTL, and WBC count has been shown to have an influence on LTL.21⇓–23 Three multivariate linear regression models were constructed to assess the association between usual source of health care and telomere length: Model 1 was adjusted for gender, age, age squared, WBC count, race, and education level, and health insurance coverage; Model 2 was further adjusted for CVD, emphysema, and high blood pressure history; Model 3 was further adjusted for smoking status and physical inactivity. For all analyses of linear regression, SAS SurveyReg procedure was utilized, and β-coefficients, standard errors (SE) and P-values were presented.
All P-values were 2-sided and a P < .05 was considered statistically significant. SAS version 9.4 was used to perform all analyses.
Results
There were 3175 NHANES respondents ages 50 to 84 years included in the analysis with complete data for the variables of interest. Table 1 shows the distribution of sociodemographic variables, disease status, and health behaviors by usual source of care status. Those with a usual source of care were more likely to be female (54.3% vs 45.7%; P = .018), white (82.2% vs 67.69%; P < .001), older (63.2 vs 59.0 years; P < .001) and have a higher level of education (P = .009) than those without a usual source of care. Those with a usual source of care were also more likely to have CVD (17.5% vs 6.6%; P < .001) and high blood pressure (45.2% vs 18.1%, P < .001) but were less likely to smoke (15.3% vs 38.1%; P < .001) or be physically inactive (42.3% vs 58.9%, P = .003).
Demographic Characteristics of NHANES 1999-2002 Participants Aged 50-84 Years by Usual Source of Care (n = 3175), Percent for Categorical Variables and Standard Error for Continuous Variables in Parenthesis
Table 2 shows the bivariate relationships between covariates and telomere length, adjusted solely for age (including an age-squared term) and WBC count. Covariates shown are those with P < .15, our predefined cutoff for inclusion the multivariate models. Even without adjustment for any covariates including age, participants with a usual source of care had a LTL 69.1 base pairs longer (P = .041) than those without a usual source of care. After adjustment for age, age squared, and WBC, the difference in telomere length is 122.9 base pairs (P < .001). Several factors were found to be significant at a P = .05 level. Shorter telomere lengths were found in men (−75.2 bp; P < .001), and those with a history of emphysema (−116.9 bp; P = .045). Those with a high school (+61.9 bp; P = .042) or college (+70.6 bp; P = .028) education had longer telomeres than those without a high school diploma. Those with high blood pressure (+74.8 bp; P = .003) had longer telomeres than those without a history of high blood pressure.
Unadjusted and Adjusted Relationships Between Telomere Length (Base Pairs) and Covariates Among NHANES 1999–2002 Participants Aged 50–84 Years
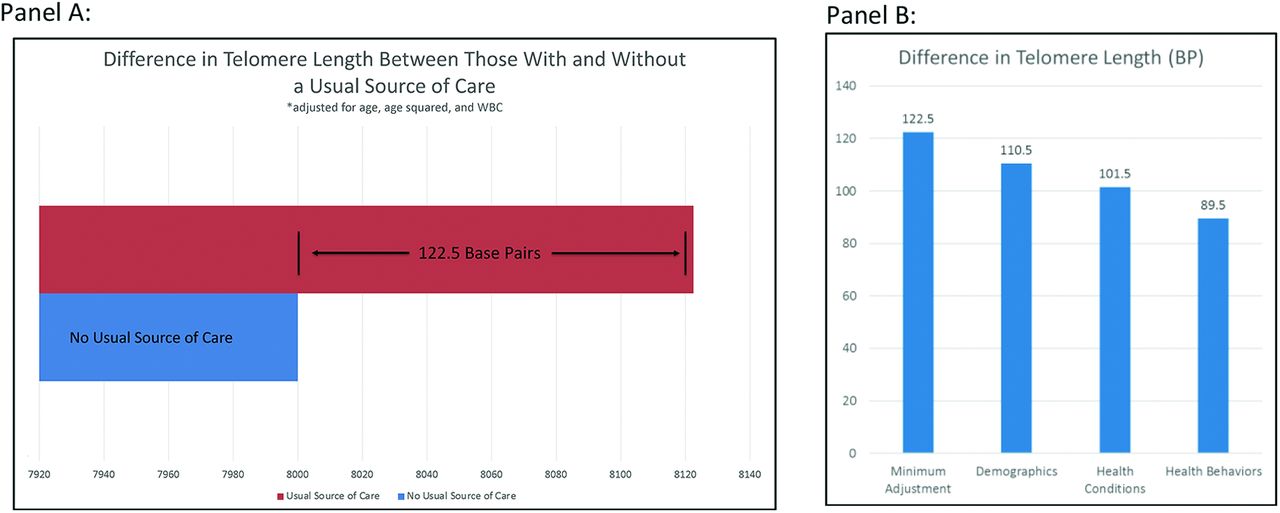
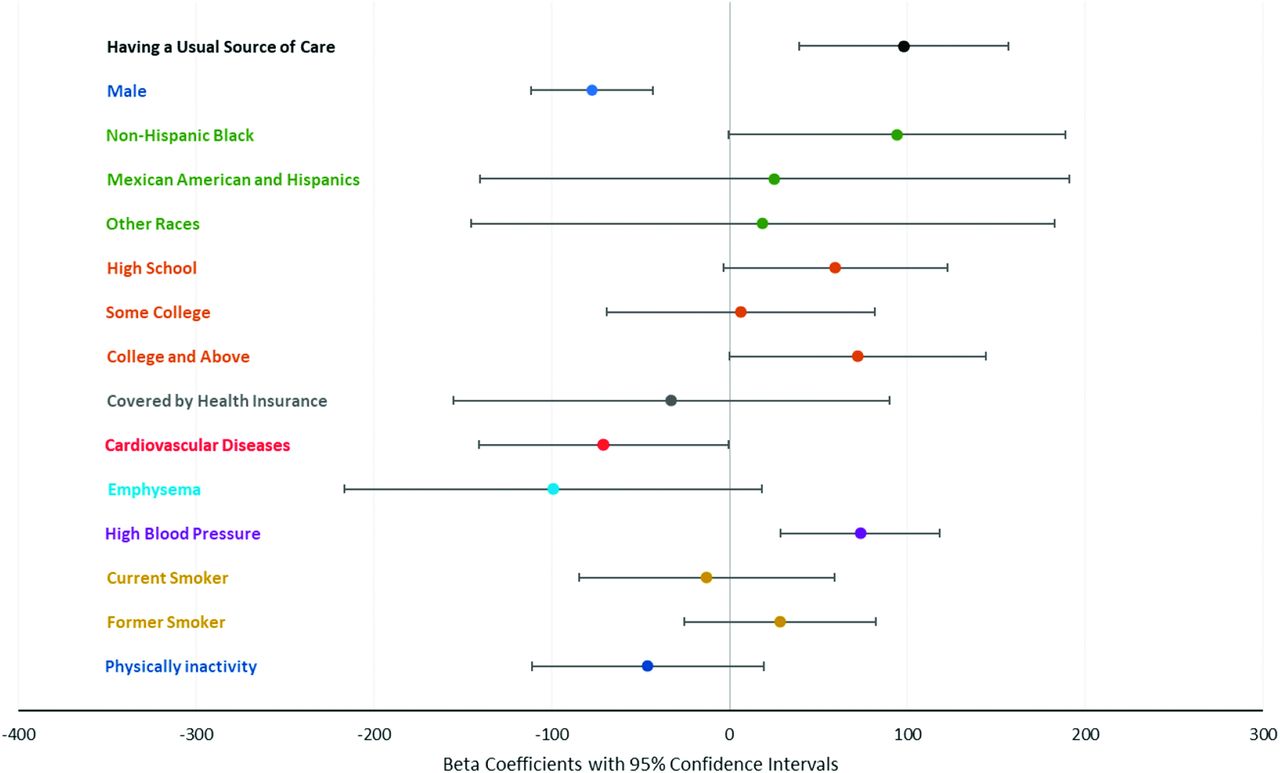
Table 3 shows the relationship between the covariates and telomere length after further adjustment. The difference in telomere length for usual source of care was attenuated to 115.5 bp (P < .001) when controlling for sociodemographic variables, it was further attenuated to 108.5 bp (P = .001) when adjusting for disease status, and further attenuated to 98.3 base pairs (P = .003) when adjusting for health behaviors (Figure 1). In the final model, those with a history of high blood pressure (+73.6 bp, P = .003) had longer telomeres. Being male (−77.3 bp; P < .001), was associated with shorter telomere length. Smoking status and physical activity were not associated with telomere length in the final model. Black race (+94.3 bp; P = .060) and college education (+72.1 bp; P = .061) were borderline significant predictors of telomere length. Higher WBC count was borderline significantly associated with shorter telomeres in all models. Age was significant when not accompanied by age squared in the models but were not significant when they were both included in the adjusted models. Figure 2 presents the β coefficients of all variables in the fully adjusted models with 95% CIs for ease of interpretation.
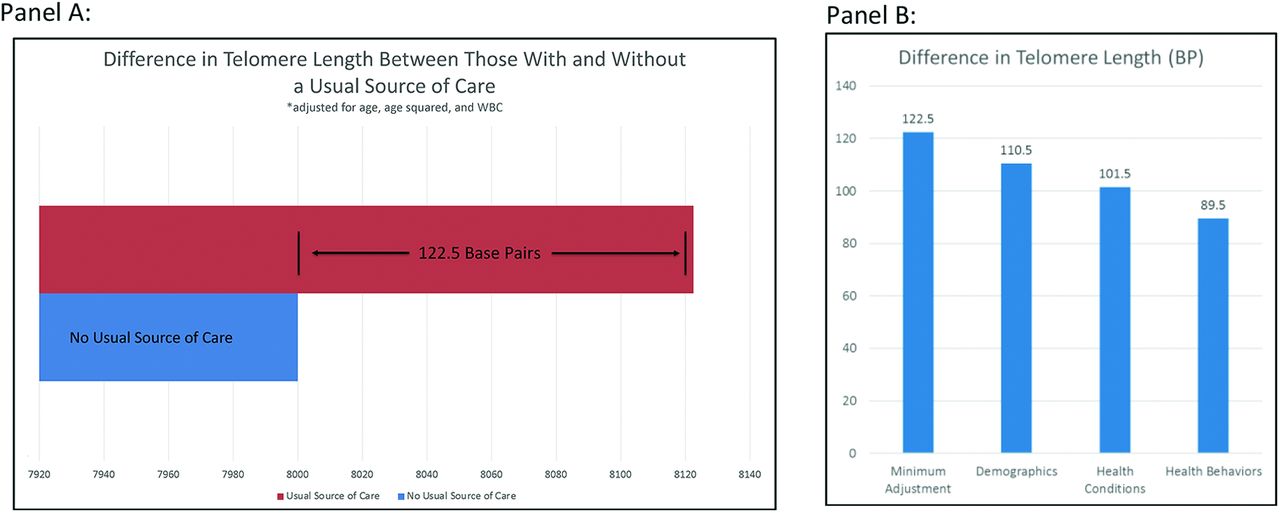
The difference in telomere length between those with and without a usual source of care (A); and the attenuation in the difference in telomere length in the stepwise models that account for demographics, health conditions, and health behaviors (B). Abbreviation: WBC, white blood cell.
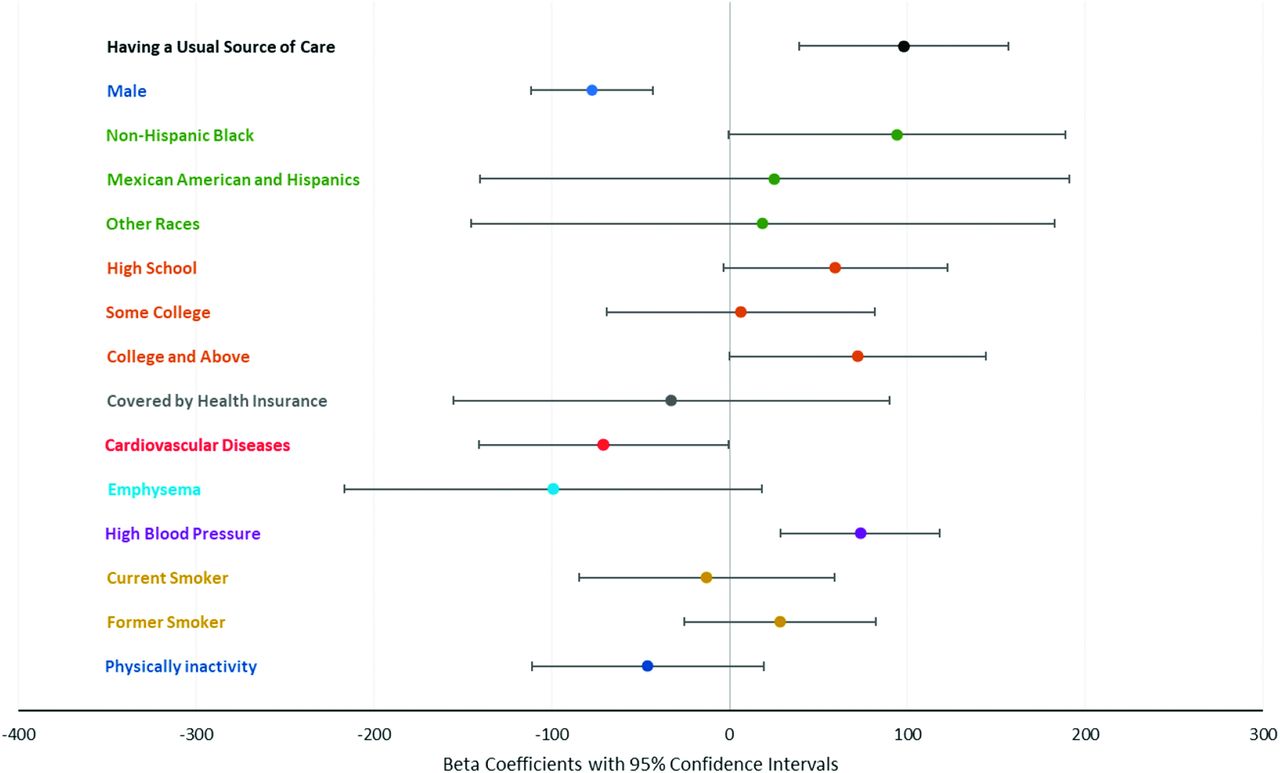
Forest plot of β coefficients and 95% CIs for the relationship between each variable in the fully adjusted model and leukocyte telomere length (base pairs).
Adjusted Relationship Between Telomere Length (Base Pairs) and Usual Source of Care Among NHANES 1999–2002 Participants Aged 50-84 Years Using Multivariate Linear Regression
Discussion
Having a usual source of care was associated with longer telomere length in a nationally representative, cross-sectional sample of adults over age 50 years. This difference remained significant after accounting for differences in sociodemographic characteristics and disease status between those with and without a usual source of care. This difference was attenuated by 11.5% when controlling for the modifiable risk factors of smoking status and physical inactivity suggesting that a small proportion of the effect of usual source of care may be due to addressing health behaviors in the primary care setting. The difference in telomere length observed in the fully adjusted models represents an approximate 7-year difference between those with and without a usual source of care. These results are important because they provide preliminary evidence for a potential causal mechanism for the observed relationship between improved access to primary care and primary care continuity and reduced mortality.5,7
There are likely multiple mechanisms by which having a usual source of primary care may impact aging and telomere length such as better management of chronic conditions, and counseling of patients on healthy lifestyle change. Our study suggests that modifiable risk factors such as smoking and physical activity levels (both of which have been found to be associated with LTL in previous studies24,25) may partially explain the association between usual source of care and telomere length, which may provide support for the physician’s role in counseling lifestyle change.
There have been no previous studies that examined the relationship between having a usual source of care on LTL, but there have been some studies that have examined how the neighborhood level socioecologic environment is associated with LTL. Having a usual source of care may be related to other characteristics of the patient’s neighborhood,26,27 so it is possible that some of the effect we observed may be due to these factors. One multisite study found that respondents who lived in neighborhoods characterized by lower aesthetic quality, safety, and social cohesion had shorter telomeres than those who lived in neighborhoods with a more salutary social environment, even after adjusting for individual-level socioeconomic status and biomedical and lifestyle factors related to telomere length.28 A Dutch study found that those who reported poor neighborhood quality had LTLs 174 base pairs shorter than those reporting good neighborhood quality.29 A study of African Americans in Atlanta, Georgia found that after controlling for sociodemographic and biomedical and psychosocial factors, a 1-SD increase in perceived neighborhood problems was associated with 7.3% shorter telomere length in women and overall unfavorable perception of neighborhood was also associated with 5.9% shorter telomere length among women.30 Further work should explore how the association we observed in this study is impacted by neighborhood level factors, which are unfortunately unavailable in the NHANES data.
Our study is in line with other previously published research that found that Black people have longer LTL;31 it is a finding that applies to people from the African continent as well as African Americans. One theory is that it may be due to melanoma-related selection pressure, as shorter telomere length is associated with less risk of this type of cancer.32 The finding that telomere length was greater in those diagnosed with high blood pressure contradicts many studies have not found an association.33⇓⇓–36 These previous studies were done in Asian and Middle Eastern Populations. Another analysis of the NHANES telomere data found a direct association with high diastolic blood pressure but an inverse association with high systolic blood pressure.23 This suggests that the relationship between LTL and blood pressure may be more complex than reported in previous research, at least among a multiracial/ethnic population in the United States.
This study has several limitations. It is a cross-sectional sample and does not have information about the length of time an individual has had a usual source of care, so respondents may have differing lengths/strengths of relationships with their usual care providers. Longitudinal studies will be necessary to determine if the presence of care continuity is responsible for changes in these risk factors and subsequent changes in telomere length. Usual source of care is a crude measure of continuity and there are more robust measures of continuity37,38 that could be used to further explore this relationship. The vast majority of the sample reported having a usual source of care, but there is likely great variability in how often the participants use that source of care. With a more refined measure that allowed us to characterize those who utilized care regularly versus seldom, it is likely we would find an even larger telomere length difference between those without a source of care and regular users of care than the sizable base pair difference that we observed. This data are from 2004 and were released in 2014. Although the data are old, the relationship between continuity of care and positive health outcomes has persisted across the last several decades and is shown in contemporary studies.5,39⇓⇓–42 Thus, we are reassured the age of the data does not invalidate the central conclusion of the article. It would be helpful to be able to contextualize our finding that the difference in LTL between those with and without a usual source of care translated to approximately 7 years of life with other studies that have examined the impact of continuity of care on mortality in older adults. While both cross-sectional and prospective studies have been done, the way the mortality has been measured as an outcome variable has been odds ratios or hazard ratios between those with and without continuity of care or those with high versus lower intensity of primary care. These values are difficult to translate into life years in the context of these studies.39⇓⇓–42 We also do not have information about the neighborhood social or built environment of the respondents, which might further influence the relationship between usual source of care and LTL observed in this study. Future studies should account for neighborhood of residence as both a potential confounder and effect modifier of the relationship between usual source of care and LTL. Aspects associated with having a usual source of care, including but not limited to increased opportunities for preventive health care, increased physician knowledge, and better adherence to treatment regimens for chronic conditions should also be examined in relation to LTL to further elucidate the pathway by which having a usual source of may influence LTL.8
In conclusion, despite the limitations of this work, this study provides the first evidence that continuity of primary care may have an impact on telomere length and the aging process. The association between having a usual source of care persisted after adjusting for demographic, health condition, and health behavior variables at the individual level. This may be one of the biologic mechanisms for the observed associations between robust primary care access, continuity of care, and reduced mortality.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: This work was partially funded by the Resource Center for Minority Aging Research (Grant 02 P30 AG031054-11); and the Research Centers in Minority Institutions (Grant U54 8U54MD007588).
To see this article online, please go to: http://jabfm.org/content/33/6/832.full.
- Received for publication January 7, 2020.
- Revision received June 23, 2020.
- Accepted for publication June 24, 2020.




{kind=link}
{kind=link}