
Abstract
Inhaled corticosteroid (ICS)–based therapy is often used for patients with chronic obstructive pulmonary disease (COPD). However, this approach is under scrutiny because of ICS overuse in patients for whom it is not recommended and because of concerns about adverse events, particularly pneumonia, with long-term ICS use. Evidence suggests ICS may be beneficial in specific patients, namely, those with high blood eosinophil counts (eg, ≥300 cells/µL) or who are at a high risk of exacerbations. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2020 ABCD assessment tool, these patients belong in group D. For these patients, recommended initial treatment includes ICS in combination with long-acting β2-agonists (LABAs) when blood eosinophil counts are ≥300 cells/µL or LABA + long-acting muscarinic antagonist (LAMA) when patients are highly symptomatic, that is, with greater dyspnea and/or exercise limitation. Follow-up treatments for patients with persistent dyspnea and/or exacerbations may include LABA + ICS, LABA + LAMA, or LABA + LAMA + ICS, with use of ICS being guided by blood eosinophil counts. In this review, differences in the inflammatory mechanism underlying COPD and asthma and the role of ICS treatment in COPD are summarized. Furthermore, findings from recent clinical trials where use of ICS-based dual or triple therapy in COPD was compared with LABA + LAMA therapy and trials in which ICS withdrawal was evaluated in patients with COPD are reviewed. Finally, a step-by-step guide for ICS withdrawal in patients who are unlikely to benefit from this treatment is proposed. A video of the author discussing the overall takeaway of the review article could be downloaded from the link provided: https://www.youtube.com/watch?v=Uq7Sr5jqPDI.
- Chronic Obstructive Pulmonary Disease
- Inhaled Corticosteroids
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)
- Eosinophil
Introduction
Inhaled corticosteroids (ICS), which are anti-inflammatory agents whose effects are mediated by activation of glucocorticoid receptors, are the cornerstone of asthma treatment.1,2 However, their use in chronic obstructive pulmonary disease (COPD) is controversial.2⇓–4 Although asthma and COPD share similar pathophysiologic features, such as chronic inflammation of the respiratory tract and airflow limitation, they differ markedly in the pattern of inflammation.5 Different inflammatory cells are recruited to bronchial airways, and various inflammatory mediators are subsequently released.5 For example, in asthma, the cells that infiltrate the airway surface include eosinophils, activated mucosal mast cells, and T cells, whereas in COPD, infiltrates mostly comprise neutrophils and T cells.5 Furthermore, in patients with asthma, ICS suppress inflammation by switching off activated inflammatory genes with the help of nuclear enzyme histone deacetylase 2, which are poorly expressed in inflammatory cells and peripheral lungs in patients with COPD.5
Despite immunologic differences in disease etiology, ICS are overused in patients with COPD.6⇓⇓–9 This sparks interest because they are not indicated in most patients10 and can increase the risk of a number of adverse events including pneumonia.11 Therefore, identifying the right patients with COPD who will benefit from ICS treatment is important. ICS are only recommended in specific patients with COPD and can be used with effect in combination with single or dual bronchodilators (long-acting β2-agonists [LABAs] and long-acting muscarinic antagonists [LAMAs]).10 Bronchodilators reduce airflow obstruction and air trapping by causing bronchodilation and reducing hyperinflation, respectively.12 While ICS monotherapy in COPD does not improve lung function or reduce mortality rates,13 when combined with a LABA, reductions in exacerbations and moderate improvements in lung function and health status have been observed.14 In this review, the benefits and risks of ICS treatment in patients with COPD are discussed.
Global Initiative for Chronic Obstructive Lung Disease Patient Classification
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) outlines a strategy for the management of COPD, which is updated regularly based on recently published scientific literature.10 In the 2017 update, the “ABCD” assessment tool was revised to offer improved individualized treatment to patients.10 Since the 2019 update, the ABCD tool is used only to guide initial treatment, while follow-up treatment is based on the most treatable trait and current treatment. Using the tool, patients are classified into groups A to D based on symptom severity (measured by the COPD Assessment Test [CAT] or the modified British Medical Research Council questionnaire [mMRC]) and exacerbation history (Figure 1). Patients in group A have fewer symptoms and none or 1 moderate exacerbation, while patients in group D have frequent exacerbations (≥2) or ≥1 exacerbation that may lead to hospital admission and report more symptoms.10
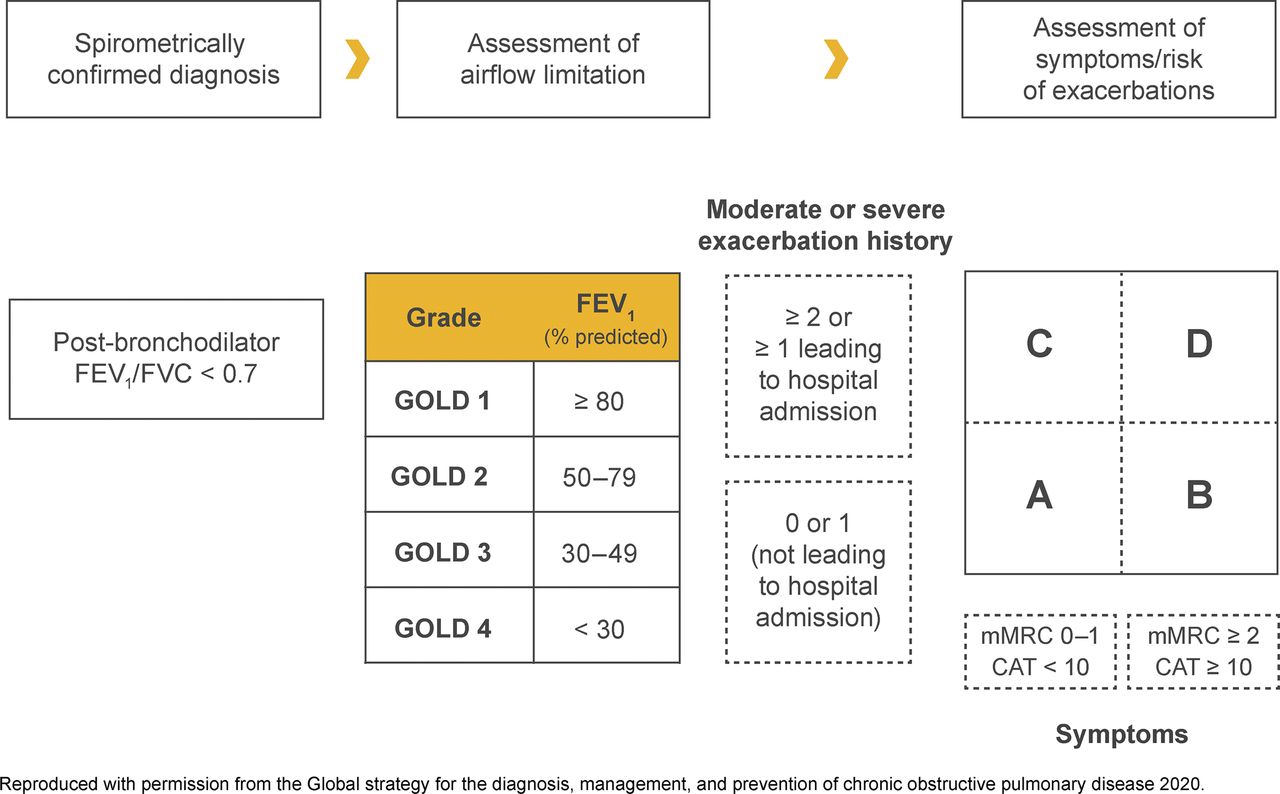
GOLD ABCD assessment tool. Abbreviations: CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced viatal capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, modified British Medical Research Council questionnaire.
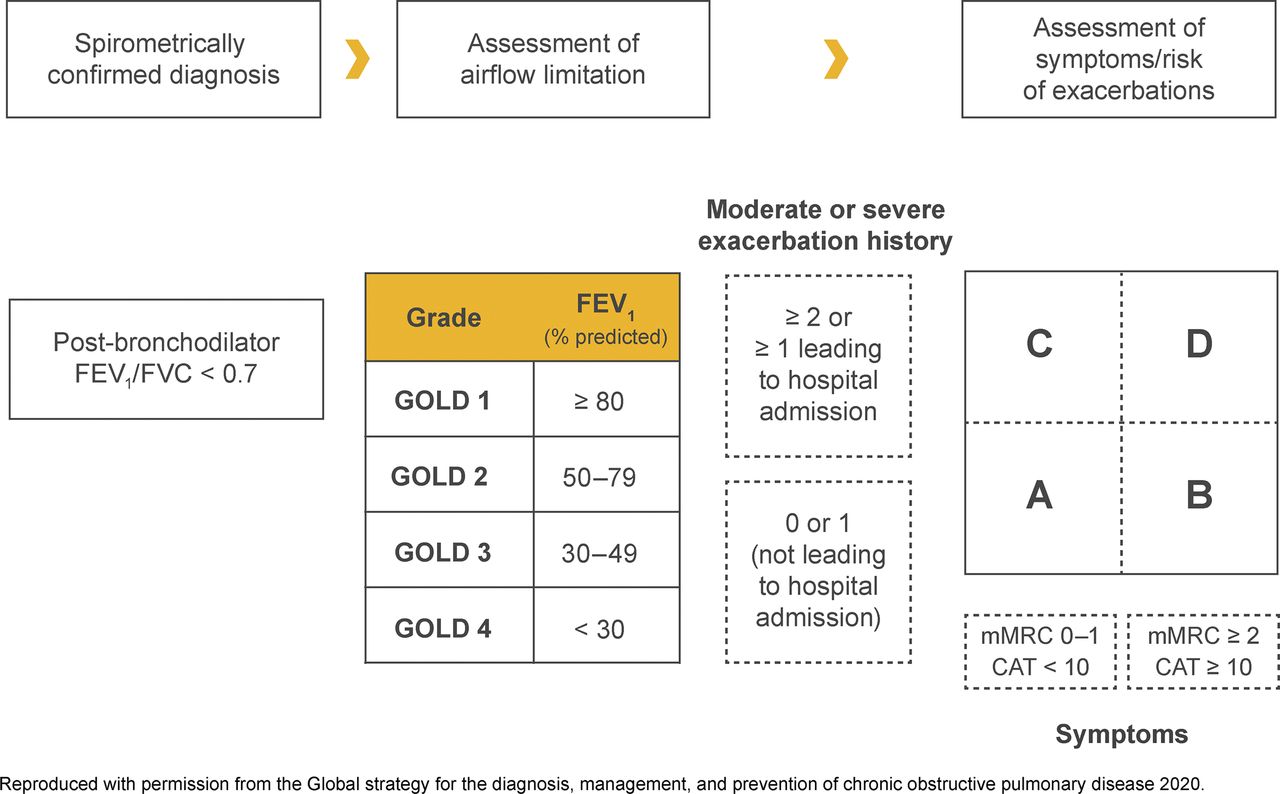
According to GOLD 2020, recommendations for initial pharmacological therapies are based on individualized assessment of symptoms and exacerbation risk (ABCD group).10 However, follow-up treatment recommendations do not depend on the patients’ GOLD group determined at diagnosis.10 An overview of treatment options is shown in Figure 2.15 During initial pharmacological management, short- or long-acting bronchodilators should be offered to all group A patients.10 For group B patients, a long-acting bronchodilator, either a LABA or a LAMA, is recommended as initial therapy. Use of 2 bronchodilators may be considered for group B patients with severe breathlessness or during follow-up assessment if severe breathlessness persists despite monotherapy. If symptoms do not improve despite therapy with dual bronchodilators, a step-down to monotherapy may be considered. For group C patients, a long-acting bronchodilator, preferably a LAMA, is recommended as initial therapy. If exacerbations persist during follow-up assessment, a LABA + LAMA or LABA + ICS combination is recommended.10 For group D patients, initial therapy with LAMA is recommended; if patients have more severe symptoms (CAT ≥20) with greater dyspnea and/or exercise limitation, LABA + LAMA is preferable10 because dual bronchodilator combination is superior to monotherapy,16 and if patients have blood eosinophil counts ≥300 cells/μL or a history of asthma, LABA + ICS may be considered the first choice.10

Treatment options for COPD. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting antimuscarinic antagonist, PdE4, phosphodiesterase-4; SABD, short-acting bronchodilator.
Some adult patients present with clinical characteristics of both asthma and COPD, commonly referred to as asthma-COPD overlap (ACO).1 Patients with ACO have higher disease burden, including frequent hospital stay, shortness of breath, use of oral corticosteroids and oxygen therapy, and emergency department visits, than patients with COPD alone.17 For patients with ACO, LAMA or LABA + ICS is recommended.1
Patients with COPD may have concomitant chronic conditions such as cardiovascular disease, metabolic syndrome, skeletal muscle dysfunction, osteoporosis, anxiety, depression, or lung cancer; therefore, comorbidities should be identified and treated to avoid influence on hospitalization or mortality.10,18 Moreover, management of COPD by appropriate nonpharmacologic interventions, such as smoking cessation, nutritional counseling, vaccination, and pulmonary rehabilitation, should also be considered (Figure 2). Although use of ICS is recommended in high-risk patients or GOLD group D,10,19 ICS are frequently inappropriately prescribed outside current treatment recommendations for patients with less severe COPD as well,6,8 which is both not of value and potentially dangerous due to adverse effects.
Use of ICS in COPD
Despite a lack of scientific evidence, ICS were prescribed to patients with COPD starting in the early 1980s because of their effectiveness in asthma.20 Since then, clinical outcomes with ICS monotherapy and ICS in combination with a bronchodilator have been investigated in numerous trials.13,21,22 Results from early trials showed that, while ICS monotherapy reduced moderate exacerbations, LABAs were more effective in improving lung function.23 These findings prompted trials of ICS + LABA combinations, where reduced exacerbations and improved lung function and health status were observed in patients with COPD.14,24 Many of these early trials predated the usage of LAMAs, which did not allow patients to have the opportunity to be treated with LABAs + LAMAs, but have since been shown to be better than LABA + ICS for lung function (ILLUMINATE, LANTERN)25,26 and exacerbations (FLAME).27⇓–29 In the FLAME trial, patients received a LAMA during a 4-week run-in period, and those who had a COPD exacerbation were withdrawn from the study.29 Therefore, while ICS-based therapy may be beneficial in some patients, of concern is the inappropriate overuse of ICS in patients with COPD.
Inappropriate prescribing of ICS has been regularly reported. In a cross-sectional survey of primary and secondary care physicians and their patients in the United States and in 5 European countries in 2011, 39% of GOLD A and 52% of GOLD B patients were receiving ICS alone or in combination with a LABA and/or LAMA.30 Similarly, in a database study in the UK in 2013, 50% of patients without concomitant asthma in GOLD stage 2 (ie, with moderate airflow limitation) and 49% of those without exacerbations in the previous year were prescribed ICS-based therapy.7 Results from a cross-sectional study using 2013 data from the National Ambulatory Medical Care Survey showed that while LABA or ICS was prescribed to 32.3% of patients, more patients (20.2%) were prescribed LABA + ICS versus LABA + LAMA (8.8%).9 In another cross-sectional study of 5% of Medicare beneficiaries, use of LABA + ICS in patients with COPD increased from 41.1% in 2008 to 49.6% in 2013.31 In a population-based study in the UK, ICS was inappropriately prescribed in almost half of GOLD A/B patients with COPD.6 Moreover, in this study, addition of ICS did not provide additional clinical benefit.
Results from several studies have shown that long-term use of ICS alone or in combination with a LABA increased the risk of pneumonia.11,32⇓–34 For example, in a 1-year double-blind study, the risk of pneumonia was significantly higher when an ICS was used in combination with a LABA versus LABA alone.32 Further, findings from a patient-level meta-analysis suggested that patients with COPD and lower blood eosinophil counts (<2%) who were treated with ICS had more pneumonia events than those with higher counts.35 In a nested case-control analysis, discontinuation of ICS was associated with a 37% decrease in the rate of pneumonia.36 However, larger studies are needed to validate this result. In at least 1 study (the SUMMIT trial), however, ICS alone or in combination with a LABA did not increase the risk of pneumonia in patients with moderate COPD.37,38 Other adverse events associated with ICS use include the risk of decreased bone density and fractures,39 diabetes,40 cataracts,41 adrenal suppression,42 and mycobacterial infections.43 Given that long-term ICS use is associated with potentially severe adverse events identifying patients who would benefit is necessary to avoid unnecessary ICS exposure.
Clinical Trial Evidence for LABA + LAMA vs LABA + ICS
Evidence from numerous clinical studies indicates LABA + LAMA combinations result in better clinical outcomes than LABA + ICS in patients with moderate-to-severe COPD with or without a history of a recent exacerbation (Table 1).25⇓–27,29,43⇓⇓⇓⇓–48 In these studies, LABA + LAMA combinations reduced hyperinflation; improved inspiratory capacity, expiratory flow, and bronchodilation; and resulted in fewer exacerbations and a longer time to first exacerbation. Results of a Cochrane review of 11 studies involving 9839 patients with moderate-to-severe COPD without recent exacerbations showed greater improvements in lung function (forced expiratory volume in 1 second [FEV1]) and quality of life (QoL), fewer exacerbations, and a lower risk of pneumonia with LABA + LAMA versus LABA + ICS.49 In the Assessment of switching salmeterol/Fluticasone to Indacaterol/Glycopyrronium in A Symptomatic COPD Patient Cohort (FLASH) study, a direct switch from LABA + ICS to LABA + LAMA improved predose FEV1 and forced vital capacity in COPD patients.50 Although most studies support the beneficial effects of LABA + LAMA versus LABA + ICS, the latter has shown greater benefit in some instances. For example, in the Informing the Pathway of COPD Treatment (IMPACT) study, which involved 10,355 patients with symptomatic COPD and a history of exacerbation within a year before enrollment, the LABA + ICS combination of vilanterol + fluticasone furoate was superior to the LABA + LAMA combination of vilanterol + umeclidinium in reducing the rate of exacerbations.51 However, some of these patients had a history of asthma and about two thirds of patients in the LABA + LAMA arm had effectively stepped down therapy (ie, withdrew ICS), which likely lead to COPD exacerbations.51,52 In the triple therapy and LABA + ICS arms patients were either maintained or stepped up to an ICS-containing therapy.51,52 Results from an open-label crossover study and a retrospective study of the Korean Obstructive Lung Disease (KOLD) cohort in patients with ACO showed that treatment with LABA + ICS improved lung function.53,54 Therefore, these results further highlight the importance of identifying the right patients who can benefit from ICS treatment. To identify such patients, a predictive marker for the effectiveness of ICS therapy could aid clinical decision-making.
Summary of Clinical Trials Comparing LABA + LAMA with LABA + ICS
Eosinophils as Markers of Response to ICS
Exacerbations are periods of acute worsening of respiratory symptoms and account for the largest proportion of COPD burden on the health care system.10 Lowering eosinophilic airway inflammation is associated with a reduction in COPD exacerbations.55 Moreover, higher blood eosinophil counts are purported to predict increased exacerbation rates and greater treatment effect with LABA + ICS versus LABA alone in patients with COPD.34,56,57 For example, in a post-hoc analysis of 2 clinical trials in patients with moderate-to-severe COPD and ≥1 exacerbation within a year before screening, the LABA + ICS combination of vilanterol + fluticasone furoate reduced exacerbations up to 24% in patients with blood eosinophil counts of ≥2 to <4%, 32% in those with counts of 4% to <6%, and 42% in those with counts ≥6% compared with vilanterol alone.55 These results suggest that an increased blood eosinophil count is likely a predictive marker for response to ICS-based treatment in patients with COPD. However, there are several inconsistencies that should be addressed. First, results from other studies are discordant with these findings and do not show an association between eosinophil counts and treatment response. Results from a French study involving a cohort of smokers and ex-smokers showed no difference in symptoms, lung function, exacerbation rate, comorbidities, or treatment in patients with COPD and different eosinophil levels.58 In another study involving smokers without COPD (COPD History Assessment In Spain cohort) and patients with COPD (body mass index, degree of airflow obstruction, functional dyspnea, and exercise capacity cohort), blood eosinophil counts were similar in both cohorts and exacerbation rates did not differ in patients with and without eosinophilia.59 Second, although blood eosinophils are considered as a biomarker for ICS-based therapy,60 they do not represent tissue eosinophilia.61 Finally, eosinophil count cutoffs have been a controversial issue.10,62 Authors of a recent review reported several barriers to the use of blood eosinophils to predict response to ICS therapy (eg, comorbidities, effort needed to calculate eosinophil counts, diurnal variation in individual blood eosinophil levels, and current medications and treatment) and recommended caution in its use as a biomarker.63 Despite these inconsistencies, GOLD 2020 generally recommends blood eosinophil counts ≥300 cells/μL as a threshold for deciding ICS-based therapy; a threshold of ≥100 cells/μL can be considered in patients who have experienced ≥2 moderate exacerbations/year or ≥1 severe exacerbation requiring hospitalization in the preceding year.10
When Is Escalation to LABA + LAMA + ICS Appropriate?
Response to dual bronchodilator or LABA + ICS treatment could guide escalation to triple therapy. According to the GOLD 2020 report, escalation to triple therapy with a LABA + LAMA + ICS is recommended for patients who develop exacerbations despite maximized LABA + LAMA treatment or if patients have persistent breathlessness or exercise limitation despite LABA + ICS.10 Addition of roflumilast or a macrolide or stopping ICS is recommended if exacerbations persist despite triple therapy.10 The efficacy of triple therapy delivered by 2 inhalers or a single inhaler has been reported in several studies;51,64⇓⇓⇓–68 however, single-inhaler therapy is generally preferable to avoid inhalation errors and improve adherence.69 Table 2 summarizes clinical trial evidence for ICS-based therapy in patients with COPD. In 2 clinical trials, fluticasone + umeclidinium + vilanterol significantly improved lung function and QoL compared with placebo + fluticasone + vilanterol in patients with COPD.66 In the GLISTEN study, glycopyrronium + fluticasone + salmeterol delivered using 2 inhalers improved lung function and QoL, and reduced the use of rescue medication in patients with moderate-to-severe COPD over 12 weeks compared with placebo + fluticasone + salmeterol.64 In the long-term (52-week) TRILOGY study, single-inhaler, fixed-dose beclomethasone + formoterol + glycopyrronium improved lung function and reduced exacerbations compared with beclomethasone + formoterol.67 In the TRINITY study, this fixed-dose triple therapy reduced exacerbation rates compared with tiotropium alone and had similar effects as open triple therapy of beclomethasone + formoterol plus tiotropium.70
Current Clinical Trial Evidence for ICS-Based Therapy in Patients with COPD
The Lung Function and Quality of Life Assessment in COPD with Closed Triple Therapy (FULFIL) study was designed to resemble real-life clinical practice by allowing patients to continue on their prestudy medication up to randomization and including patients with common comorbidities who are often excluded from other studies.65 Results of this study showed that single-inhaler fluticasone + umeclidinium + vilanterol significantly improved lung function and patient-reported outcomes, and reduced the rate of moderate or severe exacerbations, compared with budesonide + formoterol in patients with advanced, symptomatic COPD who were at risk of exacerbations.65 Results of the IMPACT study showed that single-inhaler fluticasone + umeclidinium + vilanterol significantly reduced the annual rate of moderate or severe exacerbations compared with fluticasone + vilanterol (by 15%) or umeclidinium + vilanterol (by 25%) in patients with symptomatic COPD (Figure 3).51 The risk of pneumonia was significantly higher with triple therapy versus umeclidinium + vilanterol. Approximately 20% of patients in IMPACT had bronchodilator reversibility, and therefore met the criteria for asthma and needed an ICS. Thus, these patients were likely vulnerable to exacerbation on withdrawal of ICS. In addition, almost 40% of the patients were receiving triple therapy at baseline and patients with a history of asthma were included, which may have affected results.52 In the TRIBUTE study, single-inhaler beclomethasone + formoterol + glycopyrronium significantly reduced the rate of moderate-to-severe exacerbations compared with indacaterol + glycopyrronium in patients with symptomatic COPD and an exacerbation history despite maintenance therapy (Figure 3). The occurrence of pneumonia was similar in the 2 groups.71 In the KRONOS study, single-inhaler budesonide + glycopyrrolate + formoterol fumarate improved lung function versus budesonide + formoterol fumarate in patients with mild-to-very-severe COPD who may not have had a COPD exacerbation the preceding year.72 Notably, in the IMPACT, TRIBUTE, and KRONOS studies, approximately two thirds of patients were receiving ICS at baseline;52,71,72 in some of these patients, ICS was discontinued and, unsurprisingly, a proportion of these patients experienced exacerbations. These findings reinforce the need to step down carefully. For patients who continue to experience exacerbations despite treatment with triple therapy,70 treatment with phosphodiesterase-4 inhibitors or macrolides or withdrawal of ICS is recommended.7

A summary of recent ICS withdrawal studies. Abbreviations: BDP, beclomethasone dipropionate; CI, confidence interval; FF, fluticasone furoate; GLY, glycopyrronium, ICS, inhaled corticosteroid; FEV1, forced expiratory volume in 1 second; IND, indacaterol; LABA, long-acting β2-agonist; LAMA, long-acting antimuscarinic antagonist; NA, not applicable; SFC, salmeterol and fluticasone; UMEC, umeclidinium; VI, vilanterol; Tio, tiotropium.
ICS Withdrawal
The potential for withdrawing ICS has been evaluated in several studies in an effort to inform future clinical decisions for those patients with COPD who may not truly need ICS-based therapy. In the Indacaterol: Switching Nonexacerbating Patients with Moderate COPD from Salmeterol/Fluticasone to Indacaterol (INSTEAD) Active-Comparator trial73 and the Real-Life Study on the Appropriateness of Treatment In Moderate COPD Patients (OPTIMO)74 at low risk of COPD exacerbations, no differences in lung function, breathlessness, rescue medication use, health status, or COPD exacerbations were observed among patients who switched to a LABA (indacaterol) from an LABA + ICS (salmeterol + fluticasone) combination73 or those who withdrew ICS from their LABA + ICS maintenance treatment.74 In the Withdrawal of Inhaled Steroids During Optimized Bronchodilator Management (WISDOM) study, patients were stepped up from their existing therapy to triple therapy, before being stepped down.75 ICS was withdrawn from patients taking triple therapy in 3 steps over a 12-week period. ICS withdrawal in high-risk patients taking tiotropium + salmeterol + fluticasone met the prespecified noninferiority criterion with respect to the first moderate or severe COPD exacerbation when compared with patients who continued triple therapy.75 However, a statistically significant reduction in FEV1 of 43 mL was reported after ICS withdrawal from low-dose ICS + LABA + LAMA to LABA + LAMA at the last step at week 52.
In 2 post-hoc analyses of WISDOM, ICS withdrawal resulted in higher exacerbation rates in patients with elevated eosinophil counts (≥300 cells/µL) and a history of frequent exacerbations (≥2 per year).76,77 Similarly, in the SUNSET study, withdrawal of ICS in patients on long-term (≥6 months) tiotropium + salmeterol + fluticasone with ≤1 exacerbation the previous year resulted in a small decrease in lung function, which was not considered clinically important (Figure 3).78 The annualized rate of moderate or severe COPD exacerbations did not differ after ICS withdrawal. Only patients with baseline blood eosinophil counts ≥300 cells/µL were at an increased risk of exacerbations compared with patients with lower eosinophil counts. While patients with an eosinophil count of >600 cells/µL were excluded in both the FLAME and SUNSET trials, almost no patients with this level of eosinophilia were included in WISDOM. Results from these clinical trials were replicated in the 2-year real-life Outpatient Care with Long-Acting Bronchodilators: COPD Registry in Germany (DACCORD) study of approximately 6000 patients.79 In a subgroup analysis of that study, ICS withdrawal did not increase the risk of exacerbation.79
Although accumulating results suggest that ICS withdrawal may not negatively impact patients, results of other studies suggest otherwise. In a post-hoc analysis of the TIOSPIR study of more than 17,000 patients, ICS therapy was associated with increased risk of exacerbation irrespective of exacerbation history.80 In a 5-year follow-up of the GLUCOLD study, withdrawal of ICS in patients with moderate-to-severe COPD led to an increase in airway inflammation and a decrease in lung function.81 Further, while results of a meta-analysis of randomized trials and real-world studies showed that ICS withdrawal did not increase the rate of overall COPD exacerbation,82 the risk of moderate or severe exacerbation was increased versus continuing ICS-based therapy. Though the increased risk was not significantly different, it was clinically relevant. And, although significant impairment in lung function and QoL was observed with ICS withdrawal, the differences were smaller than the respective minimal clinically important difference. According to GOLD 2020, if patients were inappropriately prescribed ICS, do not respond to ICS treatment, or show side effects, a switch from LABA + ICS or LABA + LAMA + ICS to LABA + LAMA can be considered.7 Overall, these results emphasize that while ICS can be withdrawn to reduce unnecessary therapy and the risk of pneumonia in certain patients, careful monitoring is essential since withdrawal of ICS can decrease lung function or increase exacerbation risk in some patients. A step-by-step guide for ICS withdrawal has been proposed based on these observations (Figure 4).4,83

A proposed step-by-step approach for ICS withdrawal in patients with COPD. Abbreviations: ACO, asthma-COPD overlap; CAT, COPD Assessment Test; CCQ9, Chronic COPD Questionnaire; COPD, chronic obstrutive pulmonary disease; FeNO, fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LABD, long-acting bronchodilator; LAMA, long-acting antimuscarinic antagonist; mMRC, modified British Medical Research Council questionnaire; ppb, parts per billion.
Conclusion
ICS is prescribed in many patients with COPD of varying severity and exacerbation risk. Overuse of ICS should be discouraged as long-term use is associated with various adverse events, primarily pneumonia. According to current GOLD treatment recommendations, ICS use should be considered in patients with more severe disease (group D patients with more symptoms), higher exacerbation risk (≥2 moderate exacerbations or ≥1 leading to hospitalization), history of asthma, or ACO. Identification of patients likely to benefit from ICS is essential as the potential risk of ICS therapy may outweigh the benefits if not correctly targeted. Step-by-step withdrawal of ICS should be completed in patients who are not clearly indicated for ICS therapy.
Acknowledgments
The author meets the criteria for authorship as recommended by the International Committee of Medical Journal Editors. The author received no direct compensation related to the development of the manuscript. Writing, editorial support, and formatting assistance was provided by Suchita Nath-Sain, PhD, and Maribeth Bogush, PhD, of Cactus Communications, which was contracted and compensated by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI) for these services. BIPI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Notes
This article was externally peer reviewed.
To see this article online, please go to: http://jabfm.org/content/33/2/289.full.
Conflict of interest: AK serves on the advisory board and speakers’ bureau for Boehringer Ingelheim, AstraZeneca, Purdue, Teva, Trudel, and Novartis; serves on the advisory board for GlaxoSmithKline, Mylan, Paladin, and Novo Nordisk; is a speaker for Grifols and Merck Frosst; and an advisor on Johnson and Johnson’s smoking cessation website design, outside of the submitted work.
Funding: The research was funded by Boehringer Ingelheim Pharmaceuticals, Inc.
- Received for publication June 26, 2019.
- Revision received October 11, 2019.
- Accepted for publication October 14, 2019.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.
- 85.
- 86.
- 87.
- 88.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Global Initiative for Chronic Obstructive Lung Disease Patient Classification
- Use of ICS in COPD
- Clinical Trial Evidence for LABA + LAMA vs LABA + ICS
- Eosinophils as Markers of Response to ICS
- When Is Escalation to LABA + LAMA + ICS Appropriate?
- ICS Withdrawal
- Conclusion
- Acknowledgments
- Notes
- References
- Figures & Data
- References
- Info & Metrics