
Abstract
Despite recent setbacks, disease-modifying treatments (DMTs) for Alzheimer disease (AD) might become available within a few years. These DMTs are likely to be used in the early stages of AD to avoid the progression to manifest dementia, which implies that a large reservoir of prevalent cases would need to be evaluated when DMTs first become available. Primary care providers (PCPs) would play a vital role in managing the patient flow to specialty care. We review the literature on diagnostic tests that could be used by PCPs and estimate the impact of different testing approaches on demand for specialty care.
While many tests have been evaluated, only the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) perform acceptably for detection of early-stage cognitive decline with sensitivities and specificities of 55% to 82% and 72% to 84%, respectively, for the MMSE; and 77% to 96% and 73% to 95%, respectively, for the MoCA. However, neither test is sufficiently specific for the AD pathology and would result in 4 to 5 false positives for each true positive. Blood-based tests for AD biomarkers may soon become available for clinical use. A plasma amyloid-β (Aβ) test has been shown to have a sensitivity of up to 97% and specificity of up to 81%. Adding this test to the MMSE or MoCA could reduce false positives by approximately 80%.
These findings suggest a combination of brief cognitive tests and blood-based biomarker tests will allow PCPs to identify patients with potential early stage AD efficiently and triage them for further evaluation.
- Alzheimer Disease
- Amyloid Beta-Peptides
- Biomarkers
- Cognitive Dysfunction
- Dementia
- Diagnostic Tests
- Disease Progression
- Mental Status and Dementia Tests
- Primary Health Care
- Sensitivity and Specificity
Despite multiple setbacks, such as the recent termination of the clinical trial program for aducanumab, there is still hope that a disease-modifying treatment (DMT) for Alzheimer disease (AD) will become available within the next few years.1 For example, BAN2401 was the first candidate treatment that has shown an effect on cognitive decline in a recently published Phase II trial.2 These DMTs or other medications are likely to be used in the early stages of AD to prevent progression to manifest dementia. This preventive treatment paradigm means that a substantial number of patients would need to be evaluated, diagnosed, and treated for early-stage disease. The number of patients would be particularly large when DMTs first became available because of the large reservoir of prevalent cases. A recent study has shown that the US health care system is ill prepared to meet this demand because of a lack of specialists and diagnostic and treatment centers.3 Estimated wait times of up to 19 months could potentially lead to around 2.1 million patients progressing to Alzheimer's dementia while waiting for treatment. Even in the absence of a treatment, the demand for diagnostic evaluation of cognitive impairment will increase with population ageing and emerging evidence that a correct diagnosis alone changes clinical management.4,5
Situated early in the care pathway, primary care providers will play a vital role in managing the patient flow to specialty care, as they will be responsible for triaging patients for further evaluation. To carry out this responsibility, primary care providers need proper tools, guidance, time, and reimbursement. This article will focus on the tools for the evaluation of cognitive impairment in the primary care setting. We present an overview of the pathobiology of AD, the DMTs in development and the diagnostic process with an emphasis on diagnostic tools for primary care providers, and simulate the impact of different of different approaches to the initial evaluation in the primary care setting on demand for specialty evaluation and treatment.
Pathobiology of AD
AD is a progressive neurodegenerative disease that is the most common cause of dementia in the United States, where the estimated prevalence of Alzheimer's dementia is 14.5% in adults over 65 years old.6 Amyloid-β (Aβ) plaques and neurofibrillary tangles of τ protein are the cardinal pathologic features that distinguish AD from other etiologies of dementia. The amyloid hypothesis (Figure 1) states that Aβ plaques, which can be detected by positron emission tomography (PET) scan with the Pittsburgh B (PiB) radiotracer (also known as the PiB-PET scan) or testing for Aβ levels in cerebrospinal fluid (CSF), build up in the brain due to an imbalance of Aβ production and clearance. They contribute to the formation of neurofibrillary tangles of τ protein and other downstream processes that eventually lead to neuronal death.7 As more neurons die, the patient will start exhibiting cognitive impairment. While the core clinical manifestation of AD is episodic memory impairment, other cognitive domains may also be affected, especially as the disease progresses.8,9
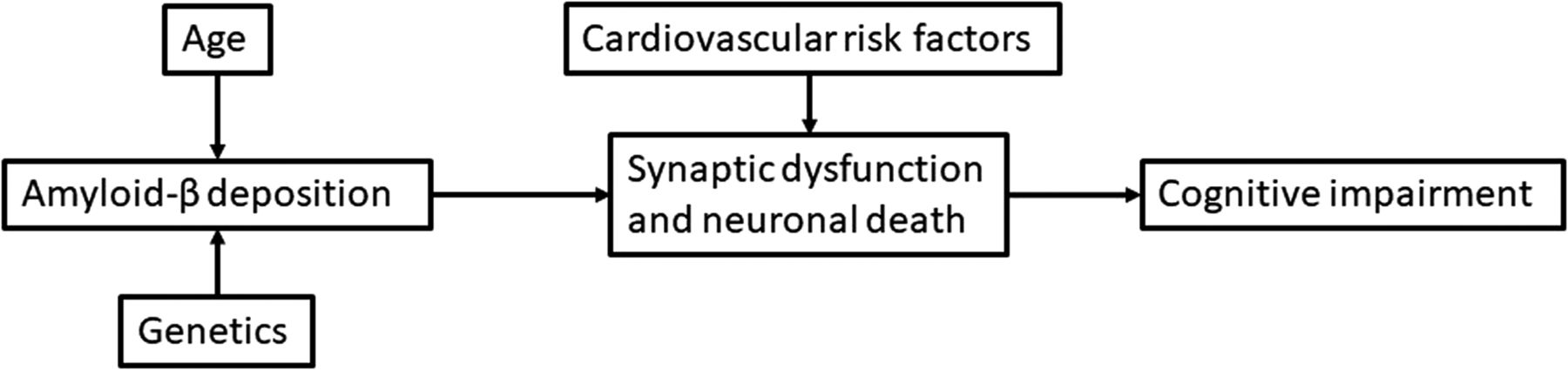
Biological model of Alzheimer disease.
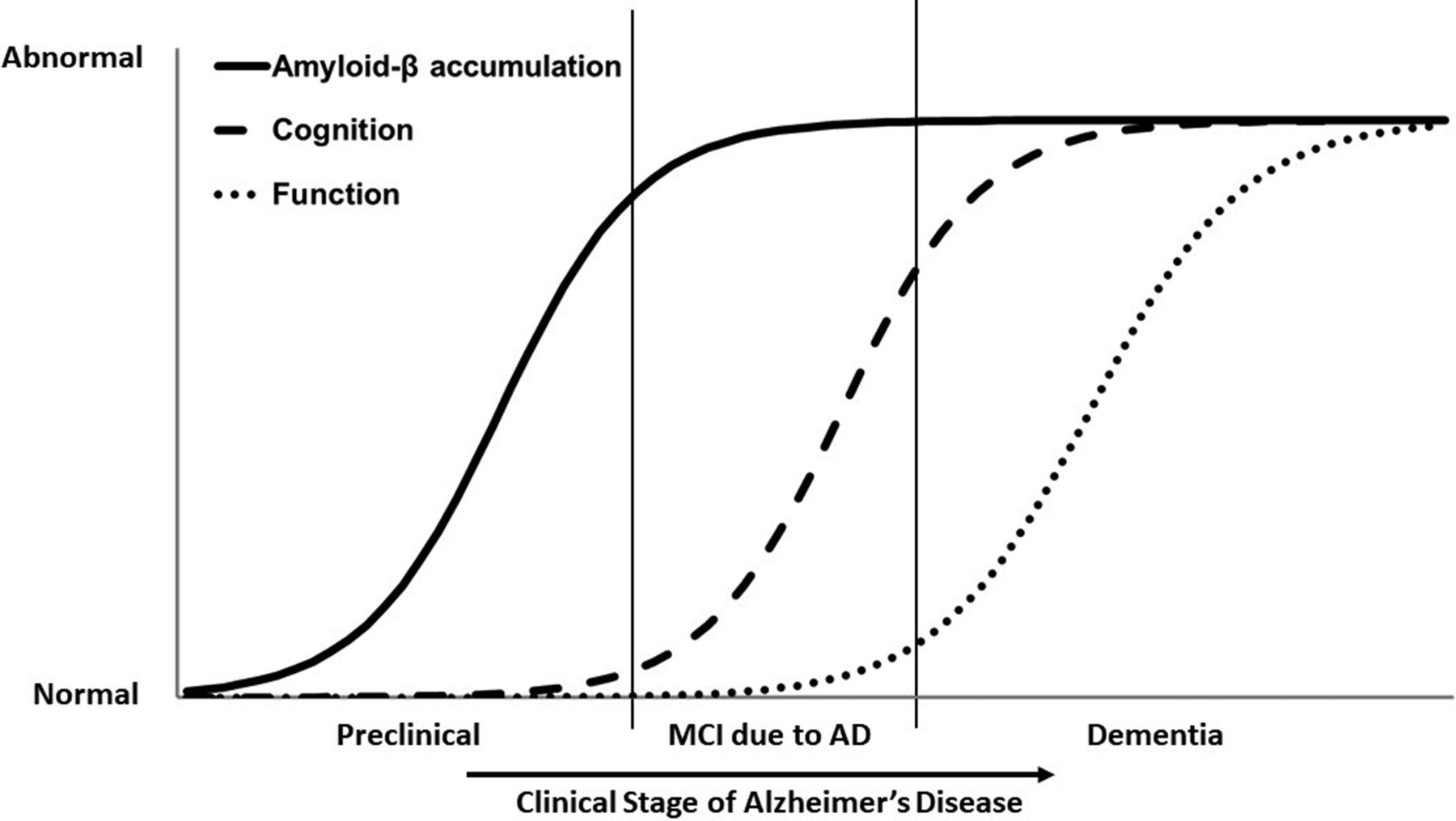
The diagnosis of AD is based on its biological hallmarks, and patients are classified into 3 stages based on clinical presentation: preclinical AD, mild cognitive impairment (MCI) due to AD, and Alzheimer's dementia (Figure 2).9 During the preclinical stage, there is no perceptible cognitive impairment, but changes in biomarkers, such as Aβ, are detectable by CSF testing and imaging. This preclinical stage may precede cognitive impairment by as much as 20 years.10,11 The next stage of AD is characterized by MCI that is detectable with neuropsychological exams; day-to-day occupational and social functioning are mostly preserved.8,12,13 The final stage of AD is dementia, which can be further subclassified into mild, moderate, and severe depending on the impact on activities of daily living.9

Classification of patients in Alzheimer disease. MCI, mild cognitive impairment.
Disease-Modifying Treatments in Development
Disease-modifying treatments (DMTs) target the pathogenic pathway of AD to delay the onset or progression of dementia. Unlike currently available symptomatic treatments, they need to be initiated before the development of moderate-to-severe dementia, implying a need to identify patients early in the disease process.
The DMTs in these active clinical trials (Table 1)14⇓⇓⇓⇓⇓⇓⇓⇓–23 target either the amyloid or τ-pathogenic pathways, but there are drugs with other mechanisms of action in the earlier stages of development.24,25 The earliest expected primary completion date for Phase III trials is in July 2022, which suggests that DMTs may become commercially available as early as 2023.
Disease-Modifying Treatments for Alzheimer's Disease in Phase 2 and Phase 3 Clinical Trials
Diagnostic Evaluation of Mild Cognitive Impairment
As the 2018 American Academy of Neurology guideline recommends, establishing a diagnosis of mild cognitive impairment (MCI) through validated tests is important because clinicians could provide important care through counseling, management of modifiable risks and nonpharmacological treatments, even in the absence of a DMT.26
The diagnostic process to evaluate cognitive function starts with short cognitive tests to detect or confirm early-stage impairment, most likely in primary care settings. Primary care providers might additionally look for alternative causes for the impairment and complicating factors that may affect the management of the patient, such as depression, cerebrovascular disease and medication and alcohol use. They would also document family history and potentially assess genetic risk.
Confirmatory diagnostic testing of MCI and identification of the underlying pathology will likely require the expertise of dementia specialists because of the complexity of the required tests and the differential diagnosis. A comprehensive neuropsychological test battery may be performed by specialists to verify and detail the degree and pattern of the cognitive impairment. Biomarker testing with either CSF analysis or PET imaging can be done to diagnose AD as the underlying etiology, but both tests are typically not yet available or covered outside of clinical research.8 Cases with mixed etiology can present with a complex pattern of symptoms and biomarker and imaging findings. Furthermore, patients with MCI may remain stable or revert to normal cognition in some cases. Given these variabilities and complexities in the disease presentation, specialists are better equipped to sort out these clinical and biomarker findings to work through the differential diagnoses and, should a DMT become available, assess the patient for treatment indications. Because specialist evaluation is complex, costly, and capacity constrained, optimizing evaluation at the primary care level is critical to reduce wait times.
Brief Cognitive Tests for MCI
Organizations like the Alzheimer's Association27 and the Gerontological Society of America28 are recommending various screening tests, such as the General Practitioner Assessment of Cognition and the Mini-Cog, to be used, for example, for cognitive assessment as part of the Annual Wellness Visit. These instruments have been validated for detection of dementia but not of MCI.29⇓–31
Beyond the General Practitioner Assessment of Cognition and Mini-Cog, there are a number of cognitive tests that have been proposed for evaluating MCI, but—similar to previous reviews—we found limited evidence supporting the use of most of these cognitive tests.29⇓⇓⇓–33 The best researched and most widely used tests in the United States to date are the mini-mental state examination (MMSE) and the Montreal Cognitive Assessment (MoCA). These tests are potentially suitable for use in primary care settings; as they take only approximately 10 to 15 minutes to administer and score without the need for dedicated equipment or specially trained personnel. They test multiple cognitive domains, but differ in how each of the domains are weighted (Table 2), which may influence their performance in detecting MCI.34
Comparison of the Scoring of Cognitive Domains by the MMSE and MoCA
MMSE
The MMSE was originally developed to assess the cognitive function of elderly, hospitalized patients with a wide range of health conditions, not specific for dementia.35 There is considerable variability in the reported diagnostic performance of the MMSE for MCI and dementia due to the heterogeneity of the patient samples, the cutoff scores, and the diagnostic criteria.29,31,36 Systematic reviews have reported that the MMSE performs relatively well in identifying possible Alzheimer's dementia, but its ability to detect MCI has been found to be suboptimal.29,31
There are several possible reasons for the limited performance of the MMSE to detect MCI: The memory and executive functioning tasks are underrepresented, and the score is sensitive to the literacy and education level of the patient.31,37,38 Furthermore, MMSE has a narrow dynamic performance range for normal individuals, creating a ceiling effect that limits the discrimination between high-scoring MCI patients and cognitively normal individuals.31,39,40
MoCA
In contrast to MMSE, MoCA was developed specifically to detect MCI29,40 and addresses some of the shortcomings of MMSE.39 It includes more complex tasks, including its test of executive function, which helps mitigate the ceiling effect.39 Although education still affects MoCA scores, MoCA tries to address the issue by adding 1 point to the scores of patients who have 12 or fewer years of education.32,40
In its original validation study, MoCA performed better than the MMSE at distinguishing MCI from normal cognition,40 and its psychometric properties have since been further validated.29,31,41,42 Studies that directly compared the abilities of the MMSE and MoCA for distinguishing MCI from normal cognition reported sensitivities of 55% to 82% and specificities of 72% to 84% for the MMSE,43⇓⇓⇓⇓⇓–49 and sensitivities of 77% to 96% and specificities of 73% to 95% for the MoCA. Meta-analyses have further suggested that MoCA may be the best MCI screening test available.30,32
Newer Cognitive Tests
The mini-Addenbrooke's cognitive examination (m-ACE)34,50,51 may have equivalent or even a slightly improved performance than the MMSE and MoCA, but as a newer test, it is not as well validated.
Computerized cognitive tests have been developed, and once they are better validated, they may improve the convenience of cognitive screening and allow the collection of additional clinical variables, such as response time and eye-movement, and facilitate detection of cognitive changes over time.52⇓⇓⇓–56
Laboratory Tests
As cognitive screening test have limited specificity for different etiologies of MCI, and PiB-PET scan and CSF testing are too expensive and invasive, respectively, for use as screening tools, blood tests with reasonable specificity for the AD pathology could improve the efficiency of the evaluation process in the primary care setting.
So far, there is no blood test for biomarkers indicative of AD pathology. Several plasma biomarkers that are specific to the AD pathology, such as Aβ and tau, or indicative of nonspecific neuronal injury, such as neurofilament light chain are in development, and others are being explored.57⇓⇓⇓⇓–62 Similar to CSF biomarkers,8 plasma biomarkers may be most useful when used in combination.
Aβ
Developing an Aβ blood test for routine clinical use proved to be challenging because of the low concentration of Aβ in plasma, the peripheral production of Aβ by platelets and the binding of Aβ to plasma proteins.63 In addition, sample storage and processing can affect the quality and reproducibility of the results.64
While early studies of plasma Aβ levels had inconsistent results,65,66 more recent studies were more promising: Nakamura et al,67 for example, reported a sensitivity of 97% and a specificity of 81%, suggesting that a test for routine clinical use might become available in the foreseeable future.67⇓–69
Tau
Changes in CSF tau levels seem later than changes in CSF Aβ levels, but there may still be a role for blood-based tau testing, as plasma tau levels correlate with AD, CSF tau levels, Aβ and tau deposition in the brain as detected by PET imaging, and cortical thickness.66,70,71 Substantial development work remains necessary before a plasma-based tau test will become available.72
Neurofilament Light Chain
As a biomarker for nonspecific neuronal injury, plasma neurofilament light chain (NfL) testing may have value when used in combination with plasma Aβ and tau testing. The correlation between plasma and CSF NfL levels is better than the correlation of plasma and CSF tau levels.70 Plasma NfL levels are also higher in Aβ-positive patients than in Aβ-negative patients.73 Plasma NfL tests are today mostly used in research.
Alternative Diagnostic Modalities in Development
There are other diagnostic modalities in earlier stages of research. Retinal scans that measure Aβ deposition in the retina are currently in various stages of clinical trials in the US, Europe, and Australia.74 An earlier study had shown that retinal Aβ plaque burden correlates with central nervous system (CNS) Aβ plaque burden.75 Since abnormal speech patterns and eye movements are potential signs of AD, automated tools and computational techniques are being developed to analyze speech and eye movement recordings.76⇓–78 Some researchers are studying olfactory dysfunction in AD,79⇓–81 while others are analyzing electroencephalography patterns.82⇓–84
Impact on Downstream Patient Caseloads
Based on US Census projections, there will be 98.8 million individuals 55 years and older in 2020.85 Extrapolating from published prevalence estimates, 10.7 million of these individuals will have MCI.26,88 Of the individuals with MCI, 6.6 million of them will have evidence of Aβ deposition in the brain.12
Using published sensitivities and specificities,45 cognitive testing of this general population with the MMSE alone would identify 5.4 million true-positive individuals with MCI due to AD (ie, have both MCI and Aβ deposition) and 27.1 million false-positive individuals. Based on the sensitivity and specificity of plasma Aβ testing reported by Nakamura et al,67 the sequential addition of plasma Aβ testing of the individuals who showed MCI on the MMSE could potentially reduce the number of false-positive cases to 5.2 million, while still detecting 5.3 million true-positive patients. Similarly, cognitive testing with MoCA45 alone would identify 5.6 million true-positive MCI due to AD patients and 21.9 million false-positive patients. MoCA, followed by plasma Aβ testing,67 would identify 5.4 million true-positive patients and 4.2 million false-positive patients.
The results (Table 3) shows how the MMSE will result in 5 false-positive cases for every 1 true-positive case detected. Replacing the MMSE with the MoCA will reduce the ratio to 4 false-positive cases for every 1 true-positive case detected. The addition of plasma Aβ testing might reduce the ratio of false to true-positive cases to about 1 to 1. In other words, it might prevent approximately 80% of the false-positive cases based on MMSE or MoCA testing from getting unnecessarily specialist referrals for confirmatory diagnosis.
Projected Impact of Diagnostic Testing on Demand for Specialty Evaluation
Discussion
In our review of effective and efficient tools that could aid primary care providers to detect MCI due to AD, we found that a large number of cognitive tests and other modalities exist but also that their utility is not well supported. Most of the cognitive tests are either not usable in primary care settings because of their length and complexity, or not well validated, or perform poorly for the detection of MCI.29⇓⇓–32 So far, only the MMSE and the MoCA have been shown to combine acceptable diagnostic accuracy and suitability for administration in primary care.
While cognitive tests perform reasonably well in determining the degree and pattern of cognitive impairment, they are inherently limited in their ability to identify the underlying etiology. A variety of diagnostic modalities attempt to differentiate the underlying etiology without expensive PiB-PET scans or invasive CSF testing, but none of them have been approved for clinical use yet. Currently, the most promising modalities are plasma biomarker tests, such as for Aβ, τ, and Nfl.65,67⇓⇓⇓–71,73 While there have been technological challenges to developing these tests, recent studies demonstrated promising results and suggest that they will be available for routine clinical use in the future, possibly in combination with each other or some of the other biomarkers in development.57⇓⇓⇓⇓–62
Our calculations underscore that a combination of cognitive testing and plasma biomarkers is probably necessary for efficient testing for MCI due to AD in primary care settings. Both the MMSE and the MoCA when used alone would result in 4 to 5 false positives for every 1 true-positive case. The addition of plasma Aβ testing would eliminate approximately 80% of these false-positive cases, reducing the number of patients who would require specialty referral by more than two-thirds. Our findings thus highlight the importance of having a reliable plasma biomarker test, especially since there is a shift toward a biological definition of AD from the historic clinical one.87
The aging US population coupled with the large reservoir of prevalent cases that would require evaluation when a DMT for AD is first approved imply a critical role for primary care providers, as they will have to prioritize patients with the greatest likelihood of benefiting from treatment for specialist visits. Intensified efforts to improve cognitive screening tools and to develop plasma biomarkers for routine use are dearly needed to enable primary care providers to play that critical role.
Notes
This article was externally peer reviewed.
Funding: This project was funded by Biogen Inc.
Conflict of interest: SM serves on the board of directors of Senscio Systems, Inc. and the scientific advisory board of aicure technologies, Boston Millennia Partners and ZanoZano. He has received consulting fees from AARP, Biotronik, Bristol-Myers Squibb, and Defined Health. JL and JH report no financial conflicts of interest.
To see this article online, please go to: http://jabfm.org/content/32/6/931.full.
- Received for publication November 5, 2018.
- Revision received June 27, 2019.
- Accepted for publication June 27, 2019.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.↵




{kind=link}
{kind=link}