
Abstract
Background: Team-based care facilitates efficient, evidence-based, patient-centered practice. An outpatient, integrated lactation consultant (LC) and primary care provider (PCP) model improves breastfeeding support, yet practices need assistance with implementation.
Method: Based on experience with team-based breastfeeding support at a suburban practice serving mainly well-educated and privately insured families, we constructed and piloted a 6-step needs assessment that informed implementation of the model at a federally qualified health center (FQHC). Practice assessment included baseline data collection of practice newborn volume, breastfeeding intent, breastfeeding rates, provider survey, and financial variables. Postimplementation outcome measurements included provider satisfaction and visit volume.
Results: Analysis using newborn volume, breastfeeding intent, and average insurance reimbursement enabled business calculation, which estimated additional 400 visits per year and revenue to cover staff training costs. The baseline provider survey (n = 20) assessed knowledge, practice resources, and barriers. The main barriers identified to providing lactation support were “not enough time” (80%) and patients “not receiving adequate help” (80%) with 58% noting “inadequate LC staffing at the clinic.” After team-based LC/PCP implementation, monthly lactation visit volume doubled. Provider postintervention assessment surveys (n = 20) demonstrated a positive response with providers reporting a perception of “providing better breastfeeding support” (100%) and that “patients had a positive breastfeeding support experience” (84%).
Conclusion: Team-based LC and PCP health care is a promising approach for delivering efficient, patient-centered, face-to-face counseling and support. Practice assessment informs financial feasibility and confirms provider interest in change. An integrated LC/PCP model can be implemented in a FQHC while enhancing patient breastfeeding support and provider satisfaction.
- Access to Health Care
- Breast Feeding
- Continuity of Patient Care
- Community Health Nursing
- Community Medicine
- Counseling
- Delivery of Health Care
- Health Care Disparities
- Health Promotion
- Lactation
- Needs Assessment
- Newborns
- Practice Management
- Practice-Based Research
- Preventive Medicine
- Primary Health Care
- Surveys and Questionnaires
- Women's Health
Outpatient breastfeeding support in the first week postpartum is critical in addressing common concerns such as low milk supply and pain, the 2 most common reasons for weaning.1,2 These difficulties impact breastfeeding duration, which continues to fall short of national goals.3 Health care provider support of breastfeeding mothers increases breastfeeding duration and exclusivity,4⇓⇓⇓–8 and national organizations recommend that breastfeeding counseling be part of routine pediatric care.9⇓–11 Yet, time constraints during routine visits limit primary care providers' (PCP) ability to provide all recommend care. Furthermore, PCPs receive limited training on treating breastfeeding difficulties and are often unprepared to address patient concerns.10⇓–12
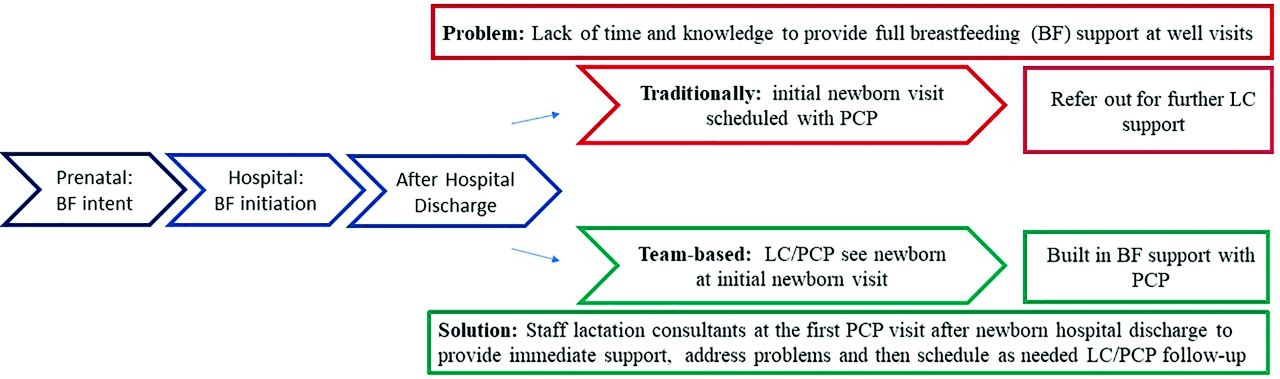
Per American Academy of Pediatrics recommendations, breastfeeding infants should see their PCP 2 to 3 days after hospital discharge to evaluate weight and jaundice.9 This visit is an ideal time to identify breastfeeding difficulties, and address concerns about pain and milk supply.2 Teaming PCP and lactation consultants (LC) at this visit remains a viable option for practices looking to provide timely, face to face support of the breastfeeding dyad (Figure 1).
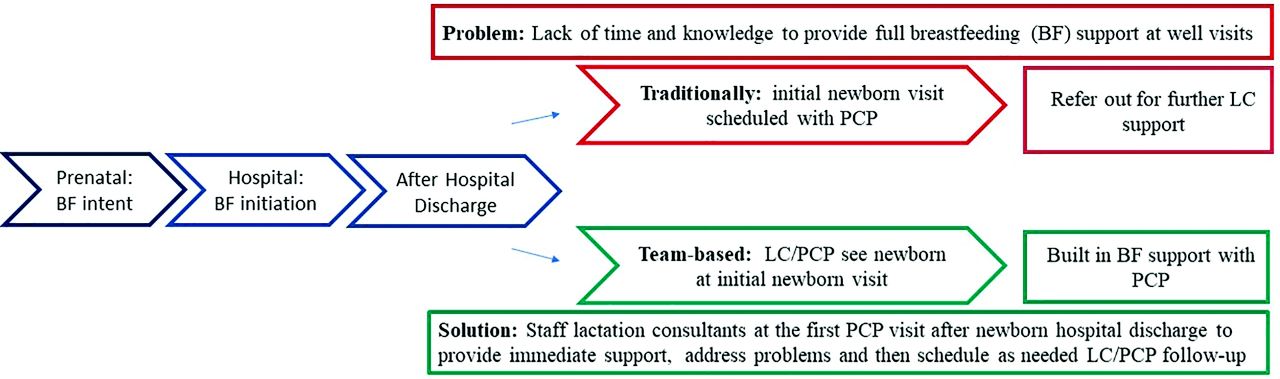
Team-based Lactation Consultant (LC)/Primary Care Provider (PCP) model of care.
Team-based care has been embraced by national medical organizations for its potential to improve patient-centered, effective, and efficient health care.13⇓–15 For breastfeeding, an outpatient team-based approach includes the PCP and LC working collaboratively to support their patient's individual breastfeeding goals during a shared visit. The team approach balances the PCP's limited time and the parental need for immediate support at the visits by using the additional training of LCs to manage breastfeeding problems.
Team-based LC/PCP care has been successfully implemented and reported in the literature for a limited number of practices.6,16⇓–18 In a randomized, nonblinded trial that included an intervention group receiving LC/PCP visits in the first week postpartum and at all well visits until weaning, Brent et al16 reported improved breastfeeding duration through 2 months compared with the control group (37% vs 9%; P = .0004) in a low-income population. At a suburban practice with high breastfeeding initiation, Witt et al6 routinely scheduled team-based visits for the initial posthospital newborn visit, following up with LC/PCP visits as needed. They found an increase in exclusive breastfeeding at 2 months (47.5% vs 58%; P = .05) and 4 months (39% vs 54%; P = .01) with a statistically significant decrease in formula use through the 9-month well visit (Odds ratio [OR], 1.12; 95%, CI, 1.02 to 1.25). In addition, postimplementation patient interviews found that mothers typically “loved the lactation support.”6 Corriveau et al18 reported a successful team-based implementation of the Academy of Breastfeeding Medicine's clinical protocol, “The Breastfeeding-Friendly Physician's Office.” Other studies, while not team-based, report on the benefits of outpatient lactation support in the primary care setting.4,5,19⇓⇓⇓–23 Despite some successes, outpatient support in the primary care setting has not been widely adopted, in part because implementing change takes planning, commitment, and expertise.
Potential collaborators often cite financial feasibility and space as common challenges to making a practice change. Given the literature on breastfeeding barriers, other expected challenges include, but are not limited to, patient or provider education, return to work, and social supports.24,25 Given studies on postnatal breastfeeding support in the primary care setting are limited,4,5 other practices may have additional barriers that need to be addressed before a wider adoption of LC integration with the initial posthospital newborn visit. To translate team-based LC/PCP care into practice and further evaluate its effectiveness in different settings, practices need assistance evaluating their specific resources and barriers.
To support these evaluations, this study was undertaken to examine the utility of gathering baseline practice information to inform implementation of team-based primary care lactation support. Our objective was to construct and pilot a pragmatic self-assessment tool for practices to assess need, evaluate financial feasibility, and assist planning for LC/PCP team-based support. We piloted the tool at a Federally Qualified Health Center (FQHC), using the data gathered from the 6-point self-assessment tool to guide the implementation of the team-based practice change.
Methods
Study Design
Our research design was a mixed-methods study. A decade of experience in team-based LC/PCP care informed the creation of the 6-point practice self-assessment tool for practice change. This was followed by an observational case study design describing pilot use of the tool to guide implementation. Finally, a postimplementation survey provided preliminary reflection on provider satisfaction and practice utilization.
Description of Intervention
Development of 6-Point Assessment Tool
The 6-point assessment tool and rationale for gathering the data are presented in Figure 2. The tool was created based on over 10 years of experience implementing and maintaining practice of team-based care in a suburban pediatric clinic with high breastfeeding initiation where both providers and patients are generally well educated on breastfeeding.6 The lead creator of the tool is a breastfeeding medicine physician and International Board Certified Lactation Consultant (IBCLC) who implemented, researched, and continues to direct team-based care at the pediatric practice. The lead creator collaborated with experienced researchers during a Practice-Based Research Methods certificate program to develop the tool.26 This process included literature review, interviews with potential stakeholders including physicians, business and practice personnel, and concluded with peer review of the tool. This clinical, research, and business collaboration identified key factors necessary to tailor the LC/PCP program to other primary care practices. The factors were then refined to clearly outline measurable practice qualities such as newborn volume, breastfeeding initiation, billing reimbursement, and provider support. Once finalized, the 6-point self-assessment tool (Figure 2) was piloted at a practice interested in expanding breastfeeding support with a demographically and socioeconomically distinct patient population from the first practice. Information gathered was organized and presented to the clinic's administration while discussing implementation of team-based LC/PCP practice change.
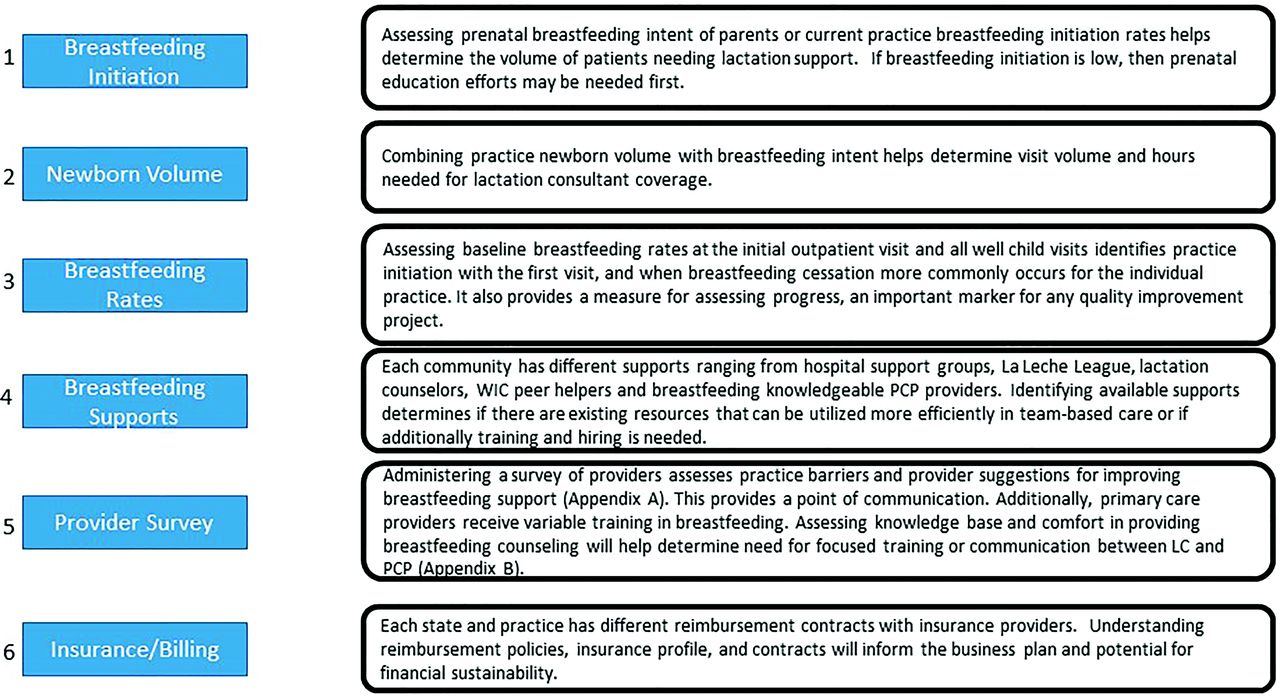
6-Point Practice Assessment tool with rationale. WIC = Special Supplemental Nutrition Program for Women, Infants, and Children; LC = Lactation Consultant; PCP = Primary Care Provider.
Setting
The pilot practice for testing the 6-point practice assessment was a federally qualified health center (FQHC) with 5 clinics at the time of the study. The largest clinic, where approximately 50% of the newborns were seen, served as the initial implementation site. We refer to this site for the remainder of the article as the initial implementation site. At the time of the practice assessment, the FQHC had a total of 10 family physicians (FPs), 8 family advanced practice nurse practioners (APRNs), and 5 certified nurse midwives (CNM); several clinicians worked at multiple sites. At the initial implementation site, there were 4 FPs, 5 APRNs, and 5 CNMs. Approximately 72% of newborns at the pilot practice received prenatal care and delivered with the CNMs. Following delivery the newborn appointment was with either a FP or APRN. While patients typically identified 1 clinic as their medical home, they could go to any of the 5 clinics for visits. One APRN, sitting for the IBCLC examination at the time of initiating practice assessment, worked 1 ½ days per week and served as the on-site breastfeeding champion for the practice change. Other than the APRN, all breastfeeding support before team-based LC/PCP support was obtained outside of the practice except for what could be done by providers briefly during visits.
Data Collection at Pilot Site
Breastfeeding rates and newborn volume: Retrospective chart review of breastfeeding rates at initial and well-child visits from October 2016 through June 2017 was completed by clinic personnel. Those patients seen only for ill visits or who transferred in after 1 month of age were excluded. Electronic medical records reports identified the number of newborn visits at the practice each month. Following practice change, the LC kept a spreadsheet recording number of LC patient visits each month.
Breastfeeding support and provider survey: A baseline anonymous survey of providers from all 5 clinics assessing existing breastfeeding supports, knowledge, and perceived barriers was conducted in July 2017 (Appendix A & B) using REDCap (Fort Lauderdale, FL) electronic data capture.27 Survey questions were created and adapted following review of previously published surveys.28,29 In July 2018, a brief survey assessing provider response to the practice change was conducted (Appendix C).
Insurance and billing: Interview of billing personnel provided insurance profile and average visit reimbursement.
Measures
Baseline practice assessment measures are breastfeeding initiation, newborn volume, breastfeeding rates, existing breastfeeding supports, provider survey, practice billing, and insurance demographics. Breastfeeding initiation, newborn volume, and breastfeeding rates were assessed from initial visit, and each well-child note (2 week, 2 month, 4 month, 6 month, 9 month, and 12 month). Feeding variables recorded were exclusive breastfeeding, any breastfeeding, or formula feeding. If the child did not have a well visit, then the feeding status was recorded as unknown. The provider survey included questions on demographics along with provider breastfeeding experience and education, confidence in providing breastfeeding counseling to patients, practice barriers to breastfeeding, and suggestions on improving breastfeeding support. The questions assessing provider confidence in providing breastfeeding counseling had 5 choices (not at all confident, not very confident, fairly confident, confident and very confident). Open-ended questions included, “If your patients are having breastfeeding difficulties beyond what you can address in the office visit, what do you do?” and “What would help you provide better breastfeeding support to your patients?” See Appendix A and Appendix B for specific survey questions and variables. Some survey questions were adapted from previously published surveys.28,29 To gather insurance and billing information, billing personnel reported percent of uninsured, public, and private insurance seen at the practice and provided average reimbursement for Current Procedural Terminology (CPT) well-child care (WCC) (99381;99391), and ill visit codes (99211 to 99215; 99201 to 99205) for public and private insurance.
Analysis
Following completion of chart review and surveys, descriptive statistical analysis using IBM SPSS statistics version 26 (Armonk, NY) was performed. In the fall of 2017, a financial analysis was completed for the pilot practice. Variables collected from the needs assessment to generate the business plan included average insurance reimbursement for public and private insurance, percent public and private insurance, newborn volume, and breastfeeding initiation rate. A standard financial analysis with categories including volume, gross revenue, net revenue, expenses and contribution to overhead was formulated in Excel. Visit volume was calculated by multiplying newborn volume and percent practice breastfeeding initiation from the baseline assessment. Average insurance reimbursements from the 2 CPT codes with the most frequent projected use for team-based visits at the pilot practice, 99203 and 99214, were used along with visit volume to calculate anticipated net revenue from the practice change. Based on the lead researcher's prior study, the financial analysis assumed an LC visit frequency of 1.5 per newborn with 30% of mothers being seen as patients for difficulties such as pain, cracked nipples, and engorgement. We assumed 2 hours per newborn encounter to cover patient visits, charting, and follow-up phone calls when calculating LC staff expenses. To calculate wage costs, we used hourly salary for RN and APRN/IBCLC currently on staff and assumed RN would participate in 75% of team-based visits and APRN/IBCLC in 25%. Other calculated expenses included travel and training for the RN to become a certified lactation counselor (CLC). The additional cost of training the RN to become an IBCLC was projected as an expense in future years.
The study procedures were approved by the Institutional Review Board of Case Western Reserve University.
Results
Use of Needs Assessment Data to Translate Team-Based LC/PCP Care into Practice
Our first step was to examine preimplementation 6-point practice assessment data gathered from the pilot practice to inform feasibility and a strategy for implementation of a team-based lactation support program. These data showed annual newborn volume (350 vs 295) and breastfeeding initiation rates (82% vs 85%) at the FQHC were similar to the primary researcher's original practice for team-based LC/PCP care.6 Breastfeeding duration at the pilot practice was 54% at 2 months, 46% at 4 months, 36.5% at 6 months, and 27% at 1 year. While breastfeeding initiation was high (82%) a large number of patients weaned by the 2-month well visit, which identified room for improvement. Characteristics of the patients receiving care at the pilot site are described in Table 1.
Patient Characteristics
To better identify provider support, knowledge and practice barriers, a provider survey was conducted in July 2017 (Appendix A and Appendix B) of providers at all 5 clinics. The survey had an 87% response rate (n = 20). Only 12% of providers were very confident in managing common breastfeeding problems, with only 6% stating their medical training prepared them very well to support breastfeeding mothers. Seventy-four percent of providers identified “there were barriers to discussing breastfeeding with their patients” with the most common barrier being “not enough time during visits” (80%). Fifty-eight percent thought there was “inadequate LC staffing at the clinic” and 80% thought that “mothers were not receiving the help they needed.” The survey found that 50% of providers referred to a LC if their patient was having breastfeeding difficulties beyond what the provider could handle at the office visit. As the APRN/IBCLC had limited availability (1.5 days per week) to see breastfeeding patients, they typically were referred outside of the practice for further assistance. The provider survey, along with knowledge of breastfeeding intention (82% initiation), confirmed that patients at the pilot practice want to breastfeed. However, despite a desire to improve breastfeeding support, providers faced challenges providing adequate breastfeeding support given barriers such as lack of time. With this knowledge, and continued discussion on the feasibility of providing routine team-based LC/PCP care for all patients, in the fall of 2017, the practice began having an infant's initial visit to the practice scheduled at the initial implementation site with the APRN/IBCLC as availability allowed.
To further inform the financial feasibility of routinely implementing team-based LC/PCP care for patients, we used baseline data on breastfeeding initiation, newborn volume, average insurance reimbursement, along with average LC visits per newborn from our previous study at a pediatric practice6 to determine visit volume and potential income. From these calculations we estimated there would be approximately 400 additional lactation-related visits per year that would cover practice overhead and staff training while providing increased revenue to the practice. The financial analysis, combined with the survey identifying PCP interest to improve breastfeeding support, garnered administrative support to routinely offer LC/PCP team-based care for the infant's first outpatient visit at the initial implementation site.
To provide team-based care, the pilot practice needed to either train existing staff or hire a LC. To minimize expenses and further the knowledge of a breastfeeding supportive registered nurse (RN) already part of the community, the practice decided to train rather than hire additional staff. The RN completed a 1-week, 45-hour, lactation-specific education class to become a Certified Lactation Counselor (CLC) followed by continued mentorship with the APRN/IBCLC on staff with the goal of becoming an IBCLC. In contrast to the CLC, an IBCLC requires 90 hours of lactation-specific education and 500 to 1000 lactation specific clinical hours depending on which pathway is chosen for certification.
In the spring of 2018, approximately 1 year after initiating the needs assessment, the practice began routinely scheduling breastfeeding newborns' first visit to the practice with both a LC and PCP at the initial implementation site whenever possible; the RN/LC was available at the initial implementation site 4 out of 5 days. A typical team-based visit was scheduled for 40 minutes with the RN/LC present for the entire visit, and the PCP joining for approximately 10 minutes to examine the infant and coordinate plan of care. The remaining 30 minutes was dedicated to lactation support including addressing latch, decreasing maternal pain, and providing breastfeeding anticipatory guidance. Each team member documented their portion of the visit in the electronic medical record. The LC documentation included history of infant feeding, output, weight, and maternal pain along with observation of breastfeeding, instruction on latch and other breastfeeding guidance given. Common topics covered included engorgement, latching, breastfeeding benefits, hand expression, and milk-storage guidelines.
In the first month of implementation, 31% of the breastfeeding newborns had a LC at their first office visit, and by the fourth month, 88% of breastfeeding infants were receiving the same support (Table 2). Because the clinic was a family practice, mothers were already patients, so a system was in place for further evaluation of maternal difficulties such as engorgement, cracked nipples, and low milk supply. Therefore, more patient encounters occurred at the practice then originally projected. With this additional volume, 6 months after implementation, 367 LC visits had occurred, exceeding the business plan projection of 400 visits per year and ensuring financial sustainability. This additional volume contrasts with a typical pediatric practice where mothers are referred elsewhere unless a provider receives additional training to provide breastfeeding medicine care for the mother.
Volume of LC/PCP* Visits First 4 Months after Team-based Practice Change
A survey was administered 4 months after implementation to further evaluate provider impression of the practice change. The survey had a 77% response rate (n = 20) for general questions including if providers “felt they provided better breastfeeding support” (100%) and “felt that their patients were breastfeeding longer” (100%). While patients were not systematically surveyed, of those providers who asked their patients, 84% noted, “their patients had a positive breastfeeding support experience” and 85% “felt they had adequate support and access to lactation when needed.” The providers who were directly involved in the team-based visits (n = 17) were given the opportunity to answer optional multiple-choice questions providing feedback about what they liked in the visits and what could be improved about the visits. Of the providers who chose to specify aspects of the visits they liked (n = 11), 100% responded, “Breastfeeding support available for patient that NP/MD previously did not have time to provide” (n = 11) and 73% liked “on-site lactation support” (n = 8) and “having the LC join an already-scheduled visit so the patient does not need an extra visit” (n = 8). Of the providers who chose to provide suggestions about improving the visit (n = 11), 82% and 91% expressed a desire for “LC support expanded to time LC is currently not available” (n = 9) and “LC support at other practice sites” (n = 10), respectively; and 73% suggested, “Better coordination of providers involved in the visit” (n = 8). The post-LC/PCP implementation provider survey reinforced the positive impact of the program on providers' ability to support their breastfeeding patients. Due to the success of the program at the initial implementation site, the pilot practice plans to expand on-site lactation support to another satellite clinic.
Discussion
The baseline needs assessment tool provides a framework for evaluating the feasibility of implementing LC/PCP team-based care. For the pilot practice, the assessment confirmed patient and provider interest, identified practice barriers, and provided information for a financial discussion. The success of launching an outpatient, integrated LC/PCP model in a FQHC with a lower baseline breastfeeding duration and more diverse socioeconomic population than the researcher's original suburban, educated practice6 is encouraging. It demonstrates the feasibility of introducing team-based care into heterogenous practice environments and reinforces the need for continued evaluation of mechanisms to transform outpatient breastfeeding support into practice.
As with any intervention, sustainability is important; financial sustainability may limit a practice's ability to engage in change. Generating a financial analysis helps practices make an informed financial decision. For the pilot practice, the analysis demonstrated financial benefit. While a formal financial study was not performed, and is a study limitation, the increased revenue in additional visits covered the main expenditures (CLC training) for the pilot practice. With FPs on staff, the pilot practice could combine treatment of baby with mother as needed for difficulties such as cracked nipples, engorgement, or mastitis. This provider flexibility increased the volume of visits from those originally projected, thus increasing income. Sites wishing to implement a LC/PCP team approach benefit from determining practice volume and insurance reimbursement to assist with financial assessment. More detailed research on cost analysis would be beneficial as there is limited reporting in the literature.17
In addition, each practice needs to evaluate appropriate staff training. Previous studies have reported success with IBCLC's in the outpatient clinic.4,6,16⇓⇓–19,21⇓⇓–24 Training an existing staff member provided timely resources without incurring additional salary costs. In choosing provider training, a practice may opt for CLC or IBCLC training. CLC training provides quicker accessibility while an IBCLC brings deeper knowledge to address more complicated breastfeeding issues. For the pilot practice, the goal remains for the RN/CLC to receive further breastfeeding training to become an IBCLC. Future studies could evaluate relative effectiveness of LC supports.
The provider survey helps practices decide where to focus education and resources. For this pilot survey, providers noted a desire to improve breastfeeding support yet were limited by expertise and time. The researcher's original practice and the pilot practice already had a PCP breastfeeding champion on staff as a resource. Another clinic may identify that medical providers are inconsistently supportive of breastfeeding and may need to focus on medical provider education first. An alternate strategy may start with a medical provider breastfeeding champion providing the support and then adding team-based LC once volume increases. The needs assessment helps generate communication and evaluation of interest and resources for creating team-based breastfeeding support. Adaptation to the individual site is important and further study can analyze individual steps in detail.
The ability to translate clinical practice into different settings is critical to change. The 6-point needs assessment helped evaluate feasibility and guided implementation of team-based breastfeeding support at a FQHC. The need for further analysis on breastfeeding duration rates and patient feedback on the program remains a study limitation and an area for future study. However, our follow-up survey confirms the medical providers view it as a positive change. The assessment tool was created based on experience at a LC/PCP program at a suburban practice, yet it helped implement team-based LC/PCP care at a FQHC with a more diverse patient population. Given breastfeeding rates are lower in African American and socioeconomically disadvantaged communities, it is important to identify methods to address health care disparities. National organizations identify as a priority increased access to professional breastfeeding support after hospital discharge.30 Identifying methods to increase face to face breastfeeding counseling, such as team-based LC/PCP care, within the primary care home is a critical step to addressing these health care disparities.
Conclusion
A cardinal goal of primary care is to support patients with preventive measures. Breastfeeding team-based care with a shared appointment model provides ongoing preventive health care for mothers and their infants. Best practices identify that PCP support is critical to breastfeeding duration and patients need support and guidance to overcome breastfeeding challenges. Recognizing that PCPs have limited time and that patients benefit from face-to-face immediate breastfeeding knowledgeable support, LC/PCP team-based care provides optimal patient-centered medical care to the breastfeeding dyad. This project confirms the feasibility and positive impact of implementing the team lactation support model in different practice environments. Measures, such as the 6-point baseline practice assessment, help translate this model into practice and remain critical to improving access for all breastfeeding dyads to receive ongoing health care provider breastfeeding support to achieve their breastfeeding goals.
Acknowledgments
The authors thank Neighborhood Family Practice for their collaboration. Senders Pediatrics and the lactation consultant team at Breastfeeding Medicine of Northeast Ohio for embracing team-based lactation care over a decade ago and for ongoing efforts to improve lactation support. The many colleagues who provided invaluable feedback during the Certificate Program in Practice-Based Research Methods 2016 to 2017 (sponsored by AHRQ R13 HS024824). The authors also thank Kay Hawn, DNP, MBA for her business analysis consultation; and Tom Hawn, MD, PhD for his research guidance.
Appendix
Provider Survey on Barriers and Ideas for Improvement
Provider Breastfeeding Counseling/Training/Experience
Post-Implementation LC/PCP Team-Based Care Survey
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
Prior Publications: Abstract 90: Optimizing breastfeeding support in primary care clinics. The The Academy of Breastfeeding Medicine, 23rd Annual International Meeting, November 14–17, 2018, San Francisco, CA.
To see this article online, please go to: http://jabfm.org/content/32/6/818.full.
- Received for publication March 30, 2019.
- Revision received June 16, 2019.
- Accepted for publication June 19, 2019.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Keywords
- Access to Health Care
- Breast Feeding
- Continuity of Patient Care
- Community Health Nursing
- Community Medicine
- Counseling
- Delivery of Health Care
- Health Care Disparities
- Health Promotion
- Lactation
- Needs Assessment
- Newborns
- Practice Management
- Practice-Based Research
- Preventive Medicine
- Primary Health Care
- Surveys and Questionnaires
- Women's Health