
Abstract
Background: Hospital readmissions contribute to high health care costs and are an indicator of poor performance. Reducing readmissions through reconnecting patients to primary care after hospitalization is a solution that is particularly relevant to complex patients with behavioral health conditions. We therefore aimed to examine the rate of follow-up visits among patients with behavioral health conditions and to assess the impact of this visit on the subsequent rate of readmission.
Methods: In this retrospective, observational study, we analyzed data from low-income uninsured adults with behavioral health conditions (n = 1905) enrolled in a health care coverage program implemented by a California County from 2012 to 2013. We used administrative encounter and eligibility data and 2 logistic regression models to predict the (1) likelihood of a timely follow-up outpatient visit and (2) likelihood of a readmission given a timely outpatient visit. Our outcomes were to calculate the marginal effects of an outpatient visit within 15 days and a readmission within 30 days of the index admission.
Results: The 15-day follow-up visit rate was 42% and readmission rate was 13%. Higher severity of illness (2.5%; P = .004; 95% CI, 0.01–0.04) and prior visits to providers (5.8%; P = .000; 95% CI, 0.04–0.08) increased the probability of a follow-up visit within 15 days. Follow-up visits (−2.5%; P = .021; 95% CI, −0.05-0.00) and a shorter index admission (0.5%; P = .039; 95% CI, 0.00–0.01) also reduced the risk of 30-day readmissions.
Conclusion: The findings provide evidence that timely linking of behavioral health patients to outpatient care after hospitalization is an effective care transition strategy, as it is likely to reduce readmission rates.
- Behavioral Medicine
- California
- Health Care Use
- Hospitalization
- Logistic Regression
- Medically Uninsured
- Outpatients
- Patient Readmission
- Retrospective Studies
Hospital readmissions lead to potentially avoidable health care expenditures and are increasingly tied to financial penalties for poor performance.1 Hospitals with excessive readmission rates among Medicare beneficiaries for 3 specific conditions (heart attack, pneumonia, and heart failure) have been penalized by as much as 3% of the hospital's total Medicare payments in the following year.2 Evidence is somewhat mixed as to the proportion of hospital readmissions that are avoidable.3⇓–5 Yet, some have argued that readmissions can be viewed as an indicator of poor quality care, inadequate planning and coordination, and failures of communication.2
Given the introduction of financial disincentives for readmissions in the Medicare program, there is a growing body of research assessing approaches to prevent readmissions.6 Several studies have found that early outpatient follow-up after a hospital admission can reduce the odds of readmission.1,6,7 The definition of “early” or “timely” outpatient follow-up in these studies ranged from 1 to 4 weeks postdischarge from the initial hospitalization or the “index event.” However, emerging research on the impact of early outpatient follow-up and other types of interventions to reduce readmissions has largely focused on Medicare beneficiaries and is in most cases limited to the specific conditions for which the Centers for Medicare and Medicaid Services has instituted penalties.6,8,9
The increasing national focus on the Triple Aim of better care, better health, and lower costs followed by the move toward value-based payment led to efforts to identify populations with higher rates of emergency department visits and hospitalizations or “acute care services.” Health care costs in the United States are highly skewed, with a small number of individuals accounting for a disproportionately large share of total expenditures.10,11 In the Medicaid program, high-cost patients frequently have mental health conditions and substance use problems and have costs that are substantially higher than those with other chronic medical conditions alone.12 Thus, patients with behavioral health conditions are prime candidates for care improvement and cost reduction efforts, and it is essential to identify the best strategies that can achieve these outcomes.13,14 Improving outcomes for adults with behavioral health conditions is specially challenging, as they are often viewed as difficult to engage in interventions designed to improve patient experience and outcomes.15 The interventions to reduce readmissions are focused on managing the postadmission transition of patients back to the community-based care.
The existing literature on care transition of mental health patients indicates primary care provider follow-up as 1 of the basic principles of successful transition.16⇓–18 Care transition efforts have been shown to reduce readmission among older adults, but the evidence of the impact in outpatient follow-up by the primary care provider for low-income populations is sparse.17
This study examines whether outpatient follow-up visits posthospitalization can prevent readmissions among adults with behavioral health conditions eligible for Medicaid. We sought to determine whether rates of 30-day readmissions were lower for patients who received timely outpatient follow-up care after their index hospital admission versus those who did not receive follow-up. We focused on adults with behavioral health conditions, who may be viewed as particularly challenging to engage, have limited self-management ability, have more complicated medication regimens, and most likely to benefit from organized and coordinated systems of care.12,15 We examined all-cause readmissions rather than inpatient psychiatric readmissions because psychiatric hospitalizations are less common and mostly concentrated among severely mentally ill patients.19 In addition, these patients have comparable or higher levels of medical comorbidity than those without behavioral health conditions.20
Study Data and Methods
Data and Sample
We used data from the Low Income Health Program (LIHP), implemented under California's “Bridge to Reform” via a Section 1115 Medicaid waiver to expand coverage to low-income uninsured adults from July 2011 to December 31, 2013. LIHP was implemented by 53 California counties that established a safety-net-based provider network and provided a defined package of covered benefits. Counties enrolled adults under age 65, who were county residents, were uninsured and not eligible for Medicaid or other public programs, had income up to 139% of the federal poverty level (or 134% without income disregards), and were US citizens or legal permanent residents who had lived in the United States for at least 5 years. In effect, LIHP enrollees were eligible for Medicaid expansion by January 1, 2014 and were transitioned into the California Medicaid program under the provisions of the Affordable Care Act (ACA). We focused on residents of San Diego County because almost 30% of nearly 73,000 LIHP enrollees had 1 or more behavioral health conditions and the county undertook efforts to enhance quality of care and improve coordination of services for these patients.
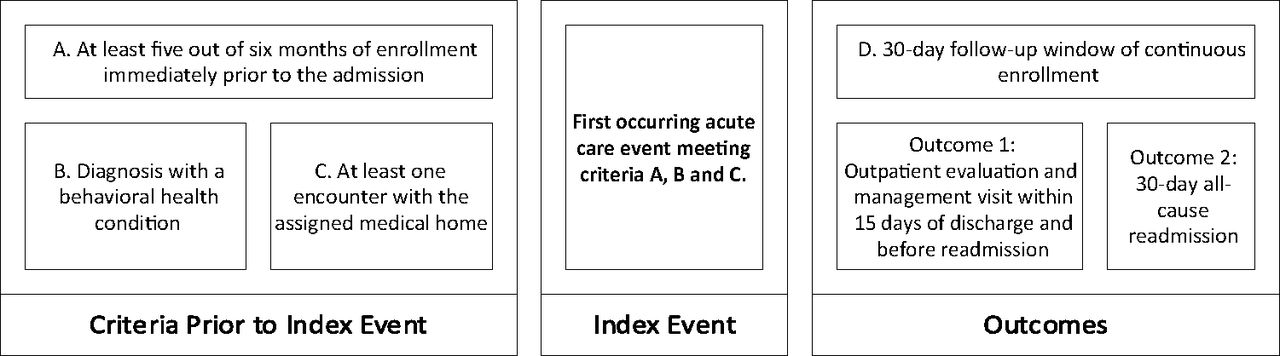
We used 2 calendar years of administrative encounter and eligibility data from 2012 through 2013. We excluded patients who did not have at least 1 inpatient admission. We then identified the earliest admission that met the following criteria: (A) had been enrolled in LIHP for a minimum of 5 out of the 6 months immediately before the admission, (B) had a known diagnosis of a behavioral health condition (mental health or substance use) according to their claims history before the admission, and (C) had an evidenced relationship (at least 1 encounter) with their assigned medical home that followed the diagnosis with a behavioral health condition but predated the inpatient admission (Figure 1). To assess outcomes, we required that individuals (D) had continuous LIHP enrollment for at least 30 days following the date of discharge from the index event to ensure that we were able to capture all use that occurred during the follow-up period of interest. Those who were disenrolled from the program (or died) during the 30-day follow-up period were excluded from the analysis. This method identified a single “index” event for each individual, in a cohort with a diagnosed behavioral health condition and an established primary care relationship at the time of the index event. Individuals with several inpatient admissions were selected into the study dataset once, on the date of the first inpatient admission for which all criteria were met. Those who had inpatient admissions but did not meet the above criteria were excluded. These criteria yielded an initial sample size of 1937 individuals.

Criteria for inclusion in the sample and sequence of care use.
We further reduced the sample by excluding patients who were treated at hospitals that had fewer than 5 attributed index events because we planned to adjust for clustering of patients within hospitals. This led to exclusion of 15 hospitals out of 30 in the sample. Of the hospitals excluded, 12 only had 1 admission, 2 had 2 admissions, and 1 hospital had 3 admissions. Most of the hospitals excluded were outside of San Diego County. We also excluded patients who had both medical or both surgical index hospitalizations and readmissions because those events were more likely to be unrelated and less likely to be avoidable. These 2 considerations lead to further exclusion of 32 patients for a final sample size of 1905 individuals.
Methods
We defined 2 outcomes of interest within the 30-day period following the date of discharge from the index event (Figure 1). First, we defined outpatient follow-up as the earliest outpatient evaluation and management (E&M) encounter that occurred within 15 days of discharge. E&M encounters were defined using current procedural technology (CPT) codes. We stopped querying the encounter data for 15-day outpatient follow-up visits on the 15th day following discharge from the index event, or on the date of the readmission, whichever came first. Thus, individuals who were readmitted within the first 15 days following the index event may have had outpatient care within the 15-day window; however, this outpatient care was not counted if it occurred after the readmission.
Second, we defined 30-day readmission as the earliest all-cause admission to any hospital within 30 days of discharge from the index event. We identified a 30-day readmission as any inpatient encounter at least 1 day after the date of discharge from the index event and with a length of stay of at least 2 days (ie, including an overnight stay). We excluded any inpatient stays that did not include an overnight stay because we believed these were likely to represent planned visits for specific procedures or follow-up treatment. For patients who had several inpatient admissions within the 30-day window, we selected the first readmission as the outcome of interest. For both the index inpatient admission and the 30-day readmission, we excluded encounters with any billing code indicating a trauma-related service.
We used available data to adjust our analyses for confounding factors, including sex, age, race/ethnicity, and the total number of months of enrollment in the LIHP before the date of admission for the index event. We also included a risk score measuring predicted future expenditures, the Chronic Illness and Disability Payment System (CDPS)21 based on the 6-month claims history for each individual before the index admission. We included indicators for substance abuse, depression, schizophrenia, and bipolar disorders. We adjusted for the length of stay of the index admission by using a quadratic term because we anticipated a nonlinear relationship with the outcome variables. We also adjusted for whether the event included surgical services, the number of E&M visits, and emergency department visits each patient had in the 6 months before the index admission. More details regarding the composition of some measures can be found in the Technical Appendix.
We used Stata version 13 for analysis.22 We conducted 2 separate logistic regressions. The first assessed the likelihood of an outpatient follow-up visit given patient and index event characteristics. The second assessed the likelihood of a 30-day readmission given receipt of an outpatient follow-up visit, controlling for patient and index event characteristics. We controlled for clustering of patients in hospitals and variations in approaches to discharge planning or connections to local primary care providers by using cluster-robust standard errors.
We conducted several sensitivity analyses to assure that our results were robust under various assumptions. We tested a random effect model treating hospital as a random intercept. We also tested models in which the definition of timely outpatient follow-up was changed to 7 days rather than 15 days following the index event. We tested models in which we only recognized 15-day outpatient follow-up visits as those that occurred at the patient's assigned primary care provider (thus excluding from the follow-up measure visits to specialists or other provider types). We further developed a structural equation model that simultaneously measured the 15-day follow-up visits and 30-day readmission, as well as a Poisson regression that included the 30-day time period for readmissions as an exposure variable. There were no substantial differences in analysis results. We only presented the results of logistic regression with cluster-adjusted robust standard errors because it has the fewest assumptions and is, therefore, most robust. We calculated the predicted probabilities and subsequent marginal effects using the Margins command in STATA (Technical Appendix) and presented the marginal effects in tables for ease of interpretation. Only results with significant p values below 0.05 are discussed.
Results
The unadjusted sample characteristics are displayed in Table 1 stratified by 30-day readmissions following the index event and in the study population overall. Overall, 42% of the sample received an outpatient follow-up visit within 15 days of discharge from the index event and before any readmission. The average number of days to follow-up was 6.5 and the median was 6 days. The average number of days to readmission was 13 and the median was 12 days (data not shown in tables). The first and third quartiles for follow-up visits were 3 days and 10 days, respectively. The first and third quartile for readmission were 6 days and 20 days, respectively (data not shown in tables). The proportion with outpatient follow-up was higher in those who were not readmitted (43% vs 37%) in simple bivariate analysis. Those who were readmitted also had higher mean number of E&M (0.70 vs 0.65) and emergency department visits (0.50 vs 0.34) in the 6 months before their index admission. The majority (67%) of patients had a medical index admission versus a surgical admission and were enrolled for about 13 months. Measures of severity show that those with a 30-day readmission also had a higher severity score (2.14 vs 1.89) and a longer length of stay during the index admission (5.58 vs 4.51) when compared with those without a readmission. Most were age 45 or older (41%) and white (49%).
Sample Characteristics of the Uninsured Adults with Mental Health Conditions Who Were Enrolled in the Low-Income Health Program in San Diego County from 2012 to 2013, Based on Enrollment and Claims Data
Table 2 presents the marginal effects for both 15-day follow-up and 30-day readmissions based on the multivariate analyses. The multivariate models are presented in the Appendix A and B. The marginal effects show that an additional E&M visit significantly increased the probability of a follow-up visit after index admission by 5.8% (95% CI, 0.04–0.08). Longer enrollment (0.3%; 95% CI, 0.00–0.01), severity as indicated by an additional day of stay for the index admission (1.2%; 95% CI, 0.00–0.02), and an extra point in the risk score (2.5%; 95% CI, 0.01–0.04) also increased the probability of a follow-up visit. Being older (16.5%; 95% CI, 0.12–0.21) increased the probability of visits than being 18 to 34 years of age. However, being African American (−10.8%; 95% CI, −0.19 to −0.03) or being diagnosed with substance abuse (−8.9%; 95% CI, −0.12 to −0.06) decreased the probability of such a visit more than whites and those without substance abuse, respectively.
Marginal Effects from the Logistic Regression Models of Follow-Up Visits and Readmissions among the Uninsured Adults with Mental Health Conditions Who Were Enrolled in the Low-Income Health Program in San Diego County from 2012 to 2013, Based on Enrollment and Claims Data
The marginal effect on 30-day readmissions was higher given more emergency department visits before the index admission (3.2%, 95% CI, 0.01–0.05), but a 15-day outpatient follow-up visit (−2.5%; 95% CI, −0.05–0.00) and an extra month of enrollment reduced this probability (−0.4%; 95% CI, −0.01–0.00). Higher risk status (1.6%; 95% CI, 0.01–0.02), a longer length of stay of index admission (0.5%; 95% CI, 0.00–0.01), and being diagnosed with substance abuse (4.9%; 95% CI, 0.01–0.09) increased the probability of readmissions. In addition, being African American (−3.0%; 95% CI, −0.06–0.00) or Asian American (−6.5%; 95% CI, −0.12 to −0.01) reduced this probability compared with being white.
Discussion
Our findings indicated that 15-day follow-up visits in patients with behavioral health conditions were more likely for patients with higher severity and for those with better connection to care, as indicated by more E&M visits before index admission and longer enrollment in the program. Such follow-up has been associated, in turn, to lower probability of 30-day readmissions, and readmissions were also more likely for patients with higher severity and other potential problems that led to more emergency department visits before index admission. Better connection to care as indicated by longer enrollment in the program could also be linked to reduced probability of readmissions.
Our findings provide support for the benefits of being connected to outpatient providers, as they allow for more E&M visits and timely follow-up postadmission. Other research has shown that overall use of acute care services among low-income childless adults is responsive to better continuity with a usual source of primary care23 and that although there may be some pent-up demand for care that drives high initial use, this pattern rapidly levels out.24 Our findings may reflect patient activation and propensity to seek care.25 But these results may also reflect better accessibility of outpatient care with coverage, better efforts by hospitals to transition patients to community providers postdischarge, or proactive primary care providers who reach out to newly discharged patients.26 We lacked data to directly assess these behaviors, but an evaluation of the San Diego LIHP program indicated significant effort to manage patients with mental health conditions.27
The marginal effect of readmissions given 15-day follow-up visits in our results is similar to marginal effect of −2.8% fewer readmissions of Medicaid patients nationally with a 7-day follow-up visit.28 The magnitude of this reduction may not be large, but the estimated average costs per hospitalization are estimated at $10,400 in 2012, and small reductions can lead to meaningful and significant reductions in expenditures.23,29
Limitations
Our study has limitations. Our data are from a unique program implemented in 1 county in California, and our findings may not be generalizable to other areas in the United States. However, the LIHP program was California's effort to emulate the eligibility criteria and benefits provided under Medicaid and in anticipation of the ACA implementation. Therefore, the data represent low-income childless adults who were the primary users of the safety-net services provided by counties nationally and were either transitioned to Medicaid in expansion states or remained largely uninsured in nonexpansion states. Moreover, the county-organized program was implemented similarly to an insurance program with a provider network and performed activities such as use management and provided support services for enrollees. The focus on a single county also reduced likely market and policy variations that could impact use patterns.
Our data did not contain information about the discharge status of patients after the index event, including death or discharge to a skilled nursing facility, that would systematically alter the predicted probability of outpatient follow-up or readmission. However, discharge to places other than the patient's home or death were likely to be relatively rare in this population due to its age and given that the enrollees were not eligible for Medicare or Medicaid due to being disabled, qualified for hospice, or other similarly serious conditions.
Our ability to adjust for severity or length of illness was limited because we lacked detailed patient records and had to rely solely on the encounter data. However, this limitation applies equally to those with and without a readmission and the bias of the analysis is unclear. We also lacked data on other factors that might promote follow-up visits and prevent readmissions, such as patients' level of engagement in their own care, self-management skills, social support, or connectedness to their primary care or other outpatient providers. These are common problems with studies using administrative data. At a minimum, our findings provide support for a clear link between the importance of ambulatory care follow-up for patients with mental health conditions as a mechanism to reduce repeat admissions. And these results are likely to be replicable in Medicaid programs and the populations that gained coverage under the ACA.
Conclusion
Follow-up visits are part of an overall strategy of concurrent interventions, such as patient education and medication reconciliation, to reduce readmission, making it difficult to identify the comparative effect of various interventions on readmission.26 Nevertheless, our findings highlight the value of follow-up visits soon after discharge, particularly for low-income patients with mental health or substance use conditions in Medicaid or other coverage/safety net programs. Our data indicate that reductions in readmission with follow-up visits are potentially effective even among patients with higher use of acute care or higher severity. Reductions in readmissions are likely to reduce costs and improve patient outcomes.
The significant findings indicating lower probability of follow-up visits and readmissions, independent of other characteristics examined in the study, are noteworthy. These findings highlight the existence of disparities in important indicators of receipt of care that improve outcomes, even within a coverage program, and the need for further intervention to reduce such disparities.
Achieving similar results in this study in other settings and for similarly high need populations is possible with developing infrastructure and promoting care processes similar to LIHP in coverage programs within the safety net. Such infrastructure includes establishing safety-net-based provider networks and opportunities for sharing data. Care processes include assigning patients to primary care providers to promote continuity of care and promoting care transitions to connect newly discharged patients to community providers.
Most importantly, similar results are better achieved with long-term coverage, as enrollment over time creates better linkage with outpatient providers and improves patients' ability to navigate the health care system.30 Achieving these benefits for patients with mental health and substance use conditions are essential in efforts to reduce readmissions because these patients frequently have high levels of severity, more challenges obtaining needed care, and are frequent users of emergency departments.14 The LIHP enrollees transitioned to Medicaid and within Medicaid, beneficiaries with behavioral health conditions have substantially higher per member spending than those without such conditions.31 Current efforts to promote integration of physical and mental health are examples of innovative efforts around the nation to improve quality and outcomes for these individuals.32
Technical Appendix
Timely Outpatient Follow-Up after Hospitalization Is Associated with Lower Readmission Rates in the Medicaid Expansion Population with Behavioral Health Conditions
This technical appendix provides supplemental information to complement the methods and results sections of the main manuscript.
Details of variable creation
We used the following Current Procedure Terminology (CPT) codes to identify evaluation and management visits: 99201 to 99215, 99241 to 99245, 99354 to 99357, 99381 to 99391.
We used CPTs between 10021 and 69990 to identify surgical procedures. The rest were considered as medical procedures.
We used the following ICD-9 codes to identify patients with substance abuse: 303.X, 304.X, 305.X.
Full results of multivariate models
The full results of the multivariate logistic regression models are presented below. The first model assessed the odds of outpatient follow-up within 15 days of the index event date of discharge (Appendix A). The second model focused on the odds of readmission within 30 days, with the primary independent variable of interest as completion of the 15-day outpatient follow-up (Appendix B).
Calculation of Marginal Effects:
The marginal effects are calculated using the following Margins command in STATA: margins. dydx (*) fault/default;;;0;
Multivariate Logistic Regression Results for Odds of an Outpatient Follow-Up Visits within 15 days of Discharge from the Index Hospitalization of the Uninsured Adults with Mental Health Conditions Who Were Enrolled in the Low-Income Health Program in San Diego County from 2012 to 2013, Based on Enrollment and Claims Data
Multivariate Logistic Regression Results for Odds of All-Cause 30-Day Readmission, Regressed on Receipt of Timely Outpatient Follow-Up of the Uninsured Adults with Mental Health Conditions Who Were Enrolled in the Low-Income Health Program in San Diego County from 2012 to 2013, Based on Enrollment and Claims Data
Notes
This article was externally peer reviewed.
Funding: Funds received for original study from the California Department of Health Care Services (contract 12–15909) and the Blue Shield of California Foundation.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/3/353.full.
- Received for publication August 22, 2018.
- Revision received December 13, 2018.
- Accepted for publication December 30, 2018.




{kind=link}