
Abstract
Introduction: Screening and referral for Social and Behavioral Determinants of Health (SDOH) are increasingly recommended in clinical guidelines and consensus statements. It is important to understand barriers and facilitators to implementation of standardized SDOH screening and referral practices, as well as the scope of current existing SDOH screening.
Methods: We conducted a mixed-methods study to understand the current state of SDOH screening and to assess the barriers and facilitators to implementing a standardized SDOH screening and referral practice in Boston community health centers (CHCs) for pediatric patients. We requested all SDOH screening documents from 15 Boston CHCs and conducted provider and staff focus groups at intervention sites of an SDOH implementation pilot in Boston.
Results: All CHCs screened in some form for SDOH, but there was no agreement on which domains to screen. Participating CHCs screened for a mean of 8 SDOH domains (range, 5 to 16). Overall, 16 SDOH domains emerged. From the focus groups, 5 themes emerged: 1) provider perspectives, 2) work flow, 3) prior experience, 4) site resources and staffing, and 5) sustainability. There was little agreement among participants within each theme, as all were seen as barriers and facilitators depending on the respondent.
Discussion: This study highlights the various SDOH screening methods currently used in Boston CHCs, and the need for workflow and process individualization of SDOH screening and referral. Providers and clinical staff should be part of the discussion when implementing SDOH screening and referral procedures to ensure appropriate work flow, staff buy-in, and to maximize resources available.
- Boston
- Community Health Centers
- Community Medicine
- Focus Groups
- Healthcare Disparities
- Primary Health Care
- Public Health
- Qualitative Research
- Social Determinants of Health
- Workflow
There is increasing awareness of the role Social and Behavioral Determinants of Health (SDOH) play in health outcomes and barriers to health equity. The World Health Organization defines SDOH as the conditions in which people are born, grow, live, work and age.1 Public health practitioners have long purported the importance of addressing these social and environmental factors' impact on health2; however the implementation of SDOH screening and referral interventions in a clinical environment is a relatively new phenomenon. Efficacy trials found that SDOH screening and referral interventions increase physician awareness of SDOH prevalence3,4 while improving referrals in the targeted population.5 With nearly 70% of variation in health outcomes driven by SDOH, there is great potential that SDOH screening and referral interventions can improve health at the individual and population levels.6,7 Recently, the Centers for Medicare and Medicaid began to incentivize innovation in screening for and addressing SDOH, further increasing its implementation and adoption in medical practices.8
The Institute of Medicine's report, Crossing the Quality Chasm9, however, described the widespread inability of medicine to implement practice innovations with proven efficacy. It takes an average of 17 years to incorporate advances from clinical research into routine practice.10 Screening and referral for SDOH is in the early stages of practice implementation and evaluation.11⇓–13 There is a paucity of empirical evidence on implementation of best practices. Evidence to date suggests that providers understand the value of SDOH screening, but find that it is time intensive and poses ethical and logistic challenges, which hinder the implementation of SDOH interventions into practice.3,14⇓⇓–17 Finally, it is unclear which specific SDOH domains are being targeted by practices for screening and referral, as there is variation among screening tools.5,18⇓⇓–21
Establishing appropriate screening and referral processes for clinical staff is imperative to achieve routine SDOH screening and referral.1,8,22⇓⇓–25 To address this implementation gap regarding integrating SDOH screening and referral interventions, we performed a mixed-methods study in Boston community health centers (CHCs). The qualitative component is an implementation evaluation of the WE CARE screening and referral pilot, described elsewhere.5 Our aims were to 1) characterize any current SDOH screening and referral practices across 15 Boston CHCs, and 2) understand facilitators and barriers in the process of screening and referral implementation of a specific SDOH screening tool in a subset of these CHCs.
Methods
To address aim 1, we requested and analyzed the SDOH screening forms from 15 Boston CHCs. To address aim 2, we conducted interviews at 3 participating study sites on implementation experiences with the WE CARE SDOH screening tool.5 We interviewed CHC providers and staff, and coded those interviews for facilitators and barriers.
This study was conducted in partnership with the Center for Community Health Education Research and Service (CCHERS), a community organization representing 15 CHCs in Boston.26 The study was approved by the Boston University Medical Center and Tufts Medical Center Institutional Review Board.
Current Screening Practices in Boston CHCs
SDOH Screening Data Collection and Domain Development
From September 2017 to January 2018, the study team requested copies of any forms used to screen for SDOH at all 15 CCHERS member CHCs. We also requested data on screening form implementation 1) when during the visit patients were screened, 2) who completes the screening form, 3) types of patient visits (new patient, return patient, acute visit, other), and 4) any specific patient population being targeted for screening (adult, pediatric, prenatal, other).
Coding and Content Analysis
Content analysis was used to code the submitted screening forms into cohesive domains and dimensions. Domains of SDOH included both social and behavioral determinants of health, and were based on prior work and published national initiatives and were revised by the research team based on preliminary coding of a subset of submitted screening forms.21 We included any references to social or behavioral determinants as SDOH. Codes were separated into “domains” representing larger categories of screening questions that were comprised of “dimensions”—more specific screening questions. Content analysis is a research method that can be used to code and quantify data from documents that were not developed primarily for analytic purposes.27,28 Three coders (EB, GY, YD) used content analysis to assign SDOH domains to each screening form. All forms were reviewed by a minimum of 2 coders. There was ≥95% concordance between coders, and all differences between coders were adjudicated by all members of the coding team. A priori, any forms submitted with a medical intent rather than a screening intent were excluded from coding. Examples of such excluded documents were screening documents for Autism Spectrum Disorder or prenatal medical history. All coding documents that had a single screening intent were assigned one code, even if they consisted of multiple questions that could have each received codes. For example, the Patient Health Questionnaire (PHQ) 9 was given a single code for “depression.”
Facilitators and Barriers to SDOH Screening Implementation
SDOH Screening and Referral Implementation
Before the WE CARE screening and referral implementation, 8 CCHERS member CHCs were identified as having no formalized SDOH screening and referral process in place.5 Six agreed to participate in a cluster randomized control trial to implement and examine the effectiveness of a screening and referral protocol for SDOH during well-child visits; 3 pediatric clinics implemented the WE CARE intervention beginning in September 2015, the other 3 served as control sites.5 The WE CARE practice workflow consisted of the following: 1) distribution of a paper WE CARE screener by medical assistants; 2) medical assistants entered responses into the electronic medical record; 3) providers or practice staff printed resource information sheets for parents; and 4) if interested, parents would be referred to a patient navigator for additional assistance.
Qualitative Instrument Development and Data Collection
We visited the 3 intervention sites to gather practitioner and staff perspectives on the context, implementation, and delivery of WE CARE during the pilot implementation phase, just before it became the standard of care. The Promoting Action on Research Implementation (PARIHS) framework was used to develop and design our data collection instrument. PARIHS is a conceptual framework that helps explain why implementing evidence into practice may or may not be successful by including the relationship between the evidence, the implementation context (in this case our clinic) and facilitation.29,30
The semistructured interview guide focused on understanding participants' knowledge of current SDOH screening practices and how the WE CARE screening and referral process compared with the previous standard of care within their CHC. We asked contextual questions about how the adoption of new practices within their setting usually worked. We also explored factors that were impacted by implementation, including staff roles and responsibilities, logistical challenges, patient challenges, and the processes by which the facilitation occurred. Finally, we asked participants about the implementation process by the study team. In total, 6 focus groups were conducted between July and August 2015 at intervention sites from the original study. Each site had 2 focus groups—1 with pediatric clinicians (physicians and nurses) and 1 with medical assistants. All sessions were conducted by a single facilitator, recorded, and professionally transcribed; the software program NVivo (QSR International Pty Ltd. Version 11, 2015) was used for transcript coding and data management.31
Qualitative Analysis
To conduct the qualitative data analysis, we used grounded theory and constant comparative methods.32,33 Two team members inductively analyzed the transcripts line by line to create codes to characterize comments and passages. The transcripts were then re-evaluated to group codes into concepts. The whole research team discussed the findings and developed a cohesive coding scheme, which was iteratively refined with review and coding of subsequent transcripts. After consensus was established, each of the remaining transcripts were coded, followed by discussion of coding discrepancies and arrival at final coding decisions. The authors completed final analyses, identifying overall themes and concepts, and selecting representative quotations. We mapped the emergent themes as either facilitators or barriers to the implementation of WE CARE.
Results
CHC Participant Characteristics
We received social and behavioral screening documents from 87% (n = 13) of all CCHERS affiliated Boston CHCs, including the 3 CHCs from the SDOH screening and referral pilot who also participated in the study focus groups. Patient demographic data and clinic characteristics were available for 11 of the 13 participating CHCs (Table 1). The 3 sites participating in the focus groups were similar to the other participant sites, with a slightly higher percentage of pediatric visits (30%; range, 27% to 32%), more racial and ethnic minority patients, and a higher percentage of patients living below 200% of the Federal Poverty Level (FPL).
Demographics of Participant Community Health Centers
Boston SDOH Screening Practices
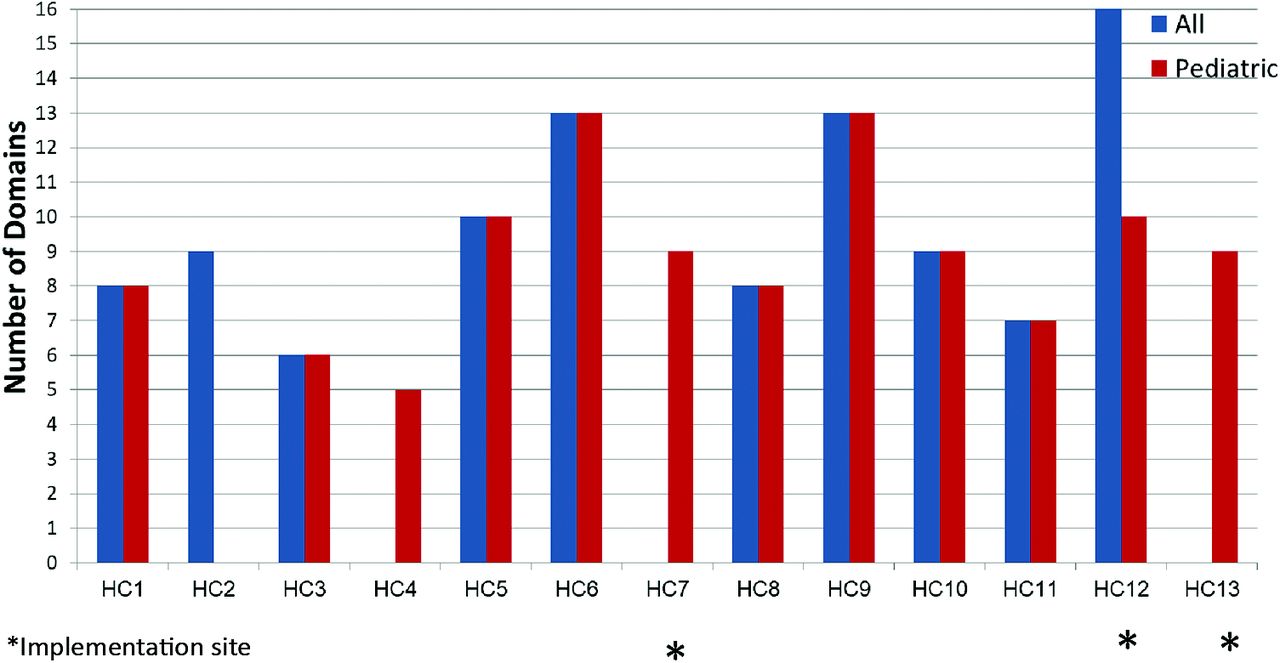
We identified 16 domains and 78 dimensions of SDOH from the screening documents submitted by participant CHCs (Table 2). Participating CHCs screened for a mean of 8 SDOH domains (range, 5 to 16). Figure 1 demonstrates the differences in the number of domains screened for in adults compared with pediatric patients in participating CHCs. Three CHCs (23%) reported only screening for SDOH in pediatric populations, with 1 (8%) participating CHC screening only for adults. Of the 9 (69%) CHCs that reported screening both children and adults during clinical visits, all but 1 screened for the same total number of domains. Of the 3 intervention sites for the WE CARE implementation and qualitative review, 2 sites reported only screening for pediatric visits, while the third screened for both adults and children (Figure 1). Figure 2 notes that not all domains were equally screened for in adult compared with pediatric visits. Mental health, health behaviors, and employment were the only domains included in the same number of pediatric and adult screening forms, while the remaining 12 domains were screened for more frequently in the adult setting. Housing was the only domain screened for in all participating CHCs.
Empirically identified SDOH Domains from Health Center Screening Documents

Number of domains screened for by each participating community health center (CHC) for pediatric visits compared with any visit.

Number of community health centers (CHCs) screening for each social & behavioral domain by adult vs. pediatric visits.
WE CARE Implementation Site Focus Group Overview and Themes
A total of 26 individuals from the 3 WE CARE pilot CHCs participated in 6 focus groups, including 9 physicians, 3 nurses, and 14 medical assistants. The focus groups ranged in size from 3 to 9 participants each. Five themes that emerged were seen as both facilitators and barriers during WE CARE implementation: 1) provider perspective on the intervention, 2) work flow, 3) prior experience, 4) site resources and staffing and 5) sustainability. There was little agreement among focus group participants within each theme, as all were seen as barriers and facilitators depending on the respondent.
Provider Perspective on the Intervention
Most providers and staff reported positive experiences with both the screening tool and the resource information sheets. Some focus group participants found the screener helpful, particularly that it was available in multiple languages, while others were concerned that the questions were asked too often of parents coming in for visits. One participant stated, “If I were a parent, I would say it is stupid. Why are you bothering me? I filled this out before… I would not even look at it. I'd throw it away.” Another felt that the screening tool allowed for important conversations to take place between the patient and provider that might not happen otherwise. “Sometimes they come in and they do not ask. Even if they are suffering, they do not ask. It is when we talk to them, we ask them a question, that is when they start to open up. With this survey right here, it is very helpful.”
Work Flow
Focus group participants diverged in their perception of level of difficulty and additional time to add WE CARE screening into clinical work flow. Several providers stated it took no additional time and felt that “… having the medical assistants do more screening than they would normally be doing, I think is a good thing.” Others felt that additional screening was too time consuming for a busy clinic, stating, “Our [Medical Assistants] will not have time to sit down with each person and do the stuff…. I do not think there's any chance, especially if it is a busy clinic.” Participants also described confusion regarding the referral processes. Some felt it was not clear when a referral was needed and to whom on the care team a patient should be referred.
Interviewee 1: “… you call the case manager on the day that [the patient navigator] is here, which is Thursdays”
Interviewer: “The case manager or the navigator?”
Interviewee 2: “[we call] the case manager… Monday through Friday. The case managers are aware of when our navigator is here and if the patients are [the right age for the study]…. But I've only had 1 patient where [the patient navigator] was here on the day that I called.”
Prior Experience
Given the demographics and socioeconomic status of the population served by the WE CARE intervention CHCs, many participants had prior experience with existing psychosocial screening and assisting patients with social services. The participants felt that this survey formalized some of the work that was already being done ad hoc in the clinic, and expressed agreement these experiences with both prior psychosocial screening as well as more general research were facilitators in the implementation of SDOH screening and referrals. All participating CHCs are also affiliated with a major academic medical center in Boston. As such, the providers and staff reported familiarity with research processes, contributing to positive provider feedback on research protocols. Providers and support staff felt that participating in research was beneficial to patients. One participant stated: “… when we participate in pilots like this? I think we like it. We find it helpful. We often incorporate it ongoing.”
Site Resources and Staffing
Despite some concerns about work flow, participants agreed that addition of a patient navigator was positive, despite the limited availability of the navigator. Some sites reported minimal interaction with the navigator, while others found the navigators helpful to identify previously underutilized community resources. Many participants reported that they felt their site had resources available to address identified needs using the screening tool, which was perceived as a facilitating factor for SDOH screening. “We have a very robust social service… When patients enroll here for care they do know that we have all these support services that they can access.” Another participant stated, “Things come up organically and people already know that this is a place where they can come to. Feel comfortable bringing up issues.” Others cited as a barrier a specific lack of resources due to system level issues and this was not something that could be overcome by implementing a screening and referral program. “… when we [send] people to the advocates… they come back and say either there was not really anything they could do. I make too much money to qualify for food stamps. The housing list is a year long.”
Sustainability of the Intervention
Focus group participants reported that they felt the ease of screening and printing out referral resource guides from the electronic medical records was a sustainable approach. Several reported that electronic access to resources via the study implementation improved their ability to offer resources to all patients, noting that before the study, there was a resource binder that was hard to find and out of date. Some participants questioned the efficacy of the intervention before being willing to implement it practice wide. There were differing levels of enthusiasm among providers for sustaining the intervention, which may reflect variations in knowledge of the study protocol and purpose. During several focus groups, when asked what participants knew about the WE CARE study, several responded “not much” or “nothing” making it difficult to comment on sustainability of the intervention.
Discussion
With increasing focus on SDOH screening and referral interventions, it is critically important to establish implementation best practices. Concerns have been raised about the time and ability of health care sites to both screen for SDOH in an empathic and ethically sound way, using patient-centered, strengths-based approaches with access to referrals and resources, while not increasing administrative tasks for already overburdened primary care providers.17,34 The focus groups were part of a larger effectiveness study of the WE CARE pilot that showed positive social outcomes for mothers screened and referred for SDOH during pediatric visits.5 We found no agreed on barriers and facilitators for what could substantially improve the implementation of screening and referral for SDOH. Yet, we found broad uptake of SDOH screening and referral practices across Boston CHCs.
The lack of agreement on facilitators and barriers to implementation points to the absence of specific structural barriers, highlighting the existence of individual styles and preferences of providers and staff and contextual factors. Differences in views expressed about the implementation process were largely between sites, rather than differences between providers and clinical staff. This important finding suggests that tailoring processes and including staff/provider buy in for implementation may overcome identified time/work flow/knowledge barriers. In our study, the implementation protocol was conceived and designed by outside researchers without specific knowledge of the culture at each participating site. In addition, each site used a different electronic medical record. To maintain fidelity to study protocol, all sites completed SDOH screening on paper, which may have limited integration and ease of implementation at the study sites. It will be important to consider involvement of clinic leadership and frontline staff to best incorporate clinical practices and ensure all providers and staff are knowledgeable and invested in study protocol and expectations.
Increased reporting of screening and referral for SDOH could be explained by several concurrent factors. First, there has been increased attention in the medical community to the importance of SDOH in the peer-reviewed literature and the lay press.11,35,36 Since the implementation of WE CARE screening began in 2015, the American Academy of Pediatrics formalized guidelines to screen for poverty-related conditions at well-child visits.37 There have also been significant policy and payment shifts toward identifying and addressing SDOH in health care, including the Accountable Health Communities model and the Massachusetts Medicaid demonstration project.38,39 In particular, we have noted that while pediatric patients make up the minority of those seeking care in our sample (Table 1), participating CHCs are largely including the same number of domains in both adult and pediatric visits (Figure 1). This signals that CHCs are screening comprehensively across patients of all ages. Three sites reported screening for SDOH in pediatric visits only. Along with broader movement in the medical field toward increasing formalized SDOH screening and referral, there may have been diffusion from our cohort of CHCs to prioritize pediatric screening.
Our findings highlight a range of SDOH domains and dimensions that are being screened for, without clear consensus for a single screening tool or agreement on particular screening questions. The most frequently screened domains included housing (n = 13), material hardship (n = 12), and mental health (n = 11), which are in alignment with national recommendations.19,21 Despite this broad agreement between Boston CHCs and national policy makers, few validated screening questions exist and therefore SDOH domain alignment does not necessarily correlate to comparable screening items. The identified diversity of SDOH domains in our data may signal differences in clinical sites' priorities for screening and referral. This may be due to onsite resource availability, specialized staff, local partnerships or other unique aspects of practice. As national guidelines and professional organizations recommend adoption of SDOH screening and referral in routine clinical practice, it will be important to enable tailoring for clinical sites to implement SDOH screening and referral practices to their strengths or perceived patient needs.
Limitations of this study include results from 1 city that might not be generalizable, yet other studies have shown similar results with regard to general acceptance of SDOH screening and referral.40 The WE CARE implementation and evaluation took place in pediatric clinics only. Processes and workflow in pediatrics might not be generalizable to all primary care settings. The implementation evaluation focused on provider feedback and experiencing, thus limiting our ability to comment on patient perspectives. Our study took place in CHCs, which may not be representative of all primary care environments. CHCs are a reasonable place to evaluate SDOH screening practices based on patient population and a mission to serve socioeconomically disadvantaged populations. CHCs often include colocated mental health or social services relevant to SDOH screening which may make CHCs unique and more likely to participate in SDOH screening compared with other primary care practices. Our data highlights the conflation by providers and staff of social determinants of health (ie, material hardship, food insecurity), behavioral determinants (ie, alcohol use, tobacco use) and mental health screening (ie, depression, stress, anxiety). While each has a distinct impact on physical health, we have included all these factors as “social and behavioral” determinants for the purposes of our analysis. We requested all SDOH screening materials used by each clinic, which was up to interpretation by the individual providing the documents and therefore might not have received everything that each site was using with respect to SDOH screening and referral. Finally, qualitative studies are hypothesis generating, and our sample may have respondent bias, but variation in responses show good representation of perspectives.
Despite not identifying successes or hurdles to SDOH screening and referral implementation, we found increased SDOH screening generally. To develop best practices in SDOH screening and referral, future work should incorporate feedback from the clinical team to improve the implementation plan, further educate site staff on study purpose and protocol, improve integration of the patient navigator into care teams, and report study outcomes to motivate further participation by providers and clinical staff. Engaging providers and patients in prioritizing SDOH screening domains to maximally benefit the patient population may encourage more provider agreement in routine SDOH screening protocols. Ongoing opportunities for provider and staff feedback will improve work flow and protocol buy in, while allowing for site specific tailoring to clinic resources and patient needs.
Acknowledgments
The authors would like to thank Elmer Freeman at the Center for Community Health and Education Services for data collection assistance.
Notes
This article was externally peer reviewed.
Funding: This research was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Grant R01MD007793. Funded by the National Institutes of Health (NIH) and by the Jonathan M. Tisch College of Civic Life at Tufts University.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/3/297.full.
- Received for publication September 17, 2018.
- Revision received December 10, 2018.
- Accepted for publication December 12, 2018.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Mobility and social deprivation on primary care utilisation among paediatric patients with asthma
- Implementation of Health-Related Social Needs Screening at Michigan Health Centers: A Qualitative Study
- Provider Impacts of Socioeconomic Risk Screening and Referral Programs: A Scoping Review
- The Most Frequently Read Articles of 2019
- Family Medicine: Data Driven Practice with Emphasis on Underserved Patients