
Abstract
Introduction: Greater occipital nerve (GON) blocks are frequently used to treat migraine headaches, although a paucity of supporting clinical evidence exists. The objective of this study was to assess the efficacy of GON block in acute treatment of migraine headache, with a focus on pain relief.
Methods: This retrospective cohort study was undertaken between January 2009 and August 2014 and included patients who underwent at least 1 GON block and attended at least 1 follow-up appointment. Change in the 11-point numeric pain rating scale (NPRS) was used to assess the response to GON block. Response was defined as “minimal” (<30% NPRS point reduction), “moderate” (31–50% NPRS point reduction), or “significant” (>50% NPRS point reduction).
Results: A total of 562 patients met inclusion criteria; 423 were women (75%). Mean age was 58.6 ± 16.7 years. Of these 562, 459 patients (82%) rated their response to GON block as moderate or significant. No statistically significant relationship existed between previous treatment regimens and response to GON block. GON block was equally effective across the different age and sex groups.
Conclusions: Greater occipital block seems to be an effective option for acute management of migraine headache, with promising reductions in pain scores.
Treatment of migraine headache is an evolving area of interest among headache specialists. A variety of medications with a spectrum of action are used in both acute and prophylactic management. Guidelines from the American Academy of Neurology and the American Headache Society (2012) are available to help direct care.1 Rescue medications for acute migraine typically consist of nonsteroidal anti-inflammatory medications, acetaminophen, and triptans; early administration yields the most promising symptom improvement. Preventive medication classes include antiepileptics, antihypertensives, and antidepressants, along with nonpharmacologic therapies such as acupuncture and physical therapy.2 Despite all these available treatments, many patients continue to experience poor symptom control.
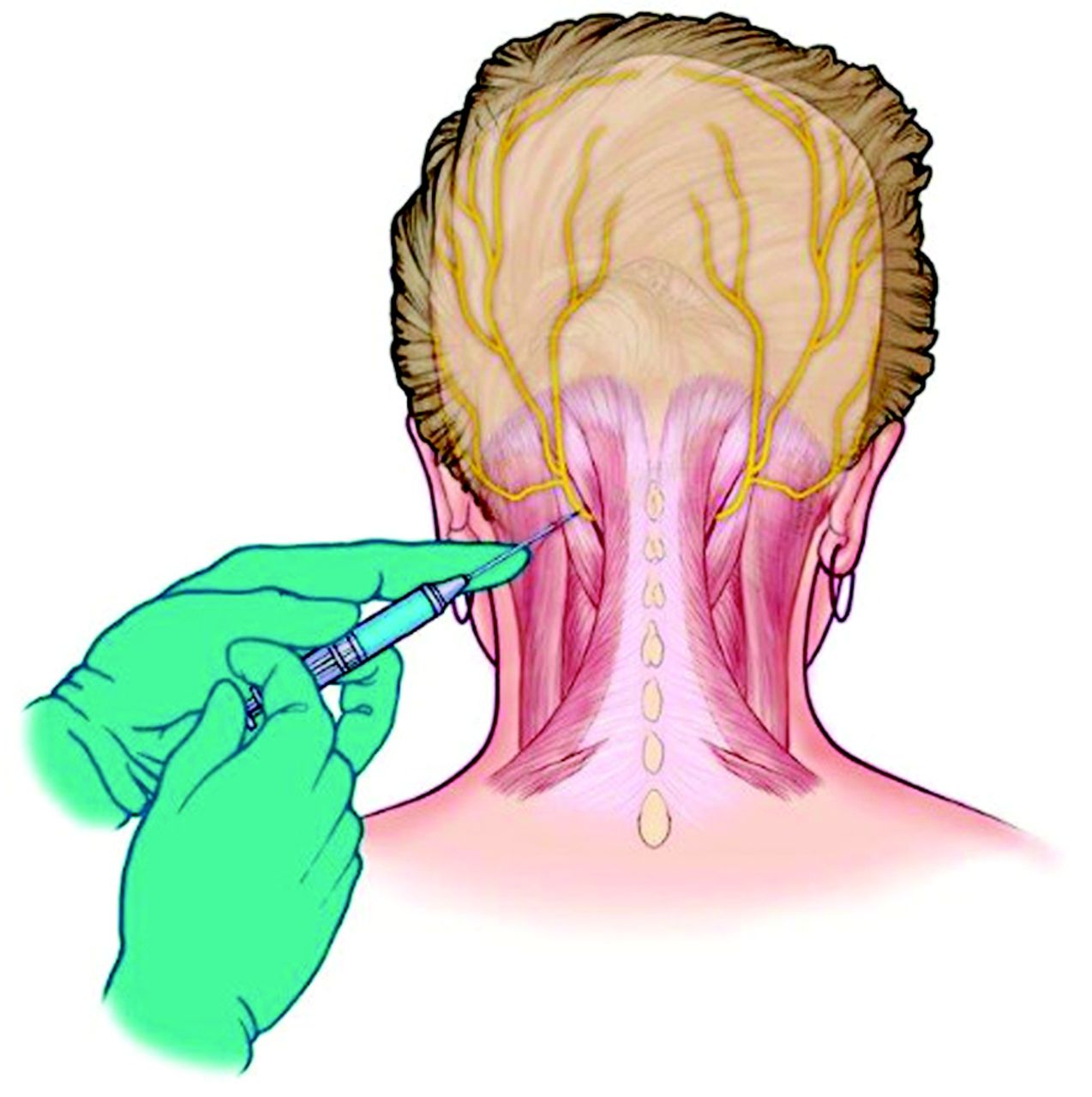
The International Classification of Headache disorders, third edition (ICHD-3; beta version)3 divides migraine into 2 major subtypes: with and without aura. Studies suggest that a peripheral mechanism may contribute to the symptoms of migraine—a theory that the literature reinforces through demonstrations of improvement in migraine headaches following injection of the botulinum A toxin.4,5 The greater occipital nerve (GON) originates in the dorsal ramus of the C2 as well as the C3 segments of the spinal cord and comprises sensory fibers alone. Its sensory distribution pathway includes the posterior part of the head and extends anteriorly toward the vertex, becoming superficial at the inferolateral aspect of the occipital protuberance. It is thought that sensory input from the GON and the ophthalmic branch of the trigeminal nerve converges into the trigeminal nucleus caudalis, which is hypothesized to be the reason why occipital neuralgia is sometimes associated with migraine headache symptomatology.6 GON block decreases afferent input to the trigeminal nucleus caudalis, resulting in central pain modulation and reducing neuronal hyperexcitability at the level of second-order neurons.7 The procedure to inject the GON is demonstrated in Figure 1; this involves inserting a needle into the inferolateral aspect of the occipital protuberance and injecting a combination of local anesthetic and a corticosteroid.
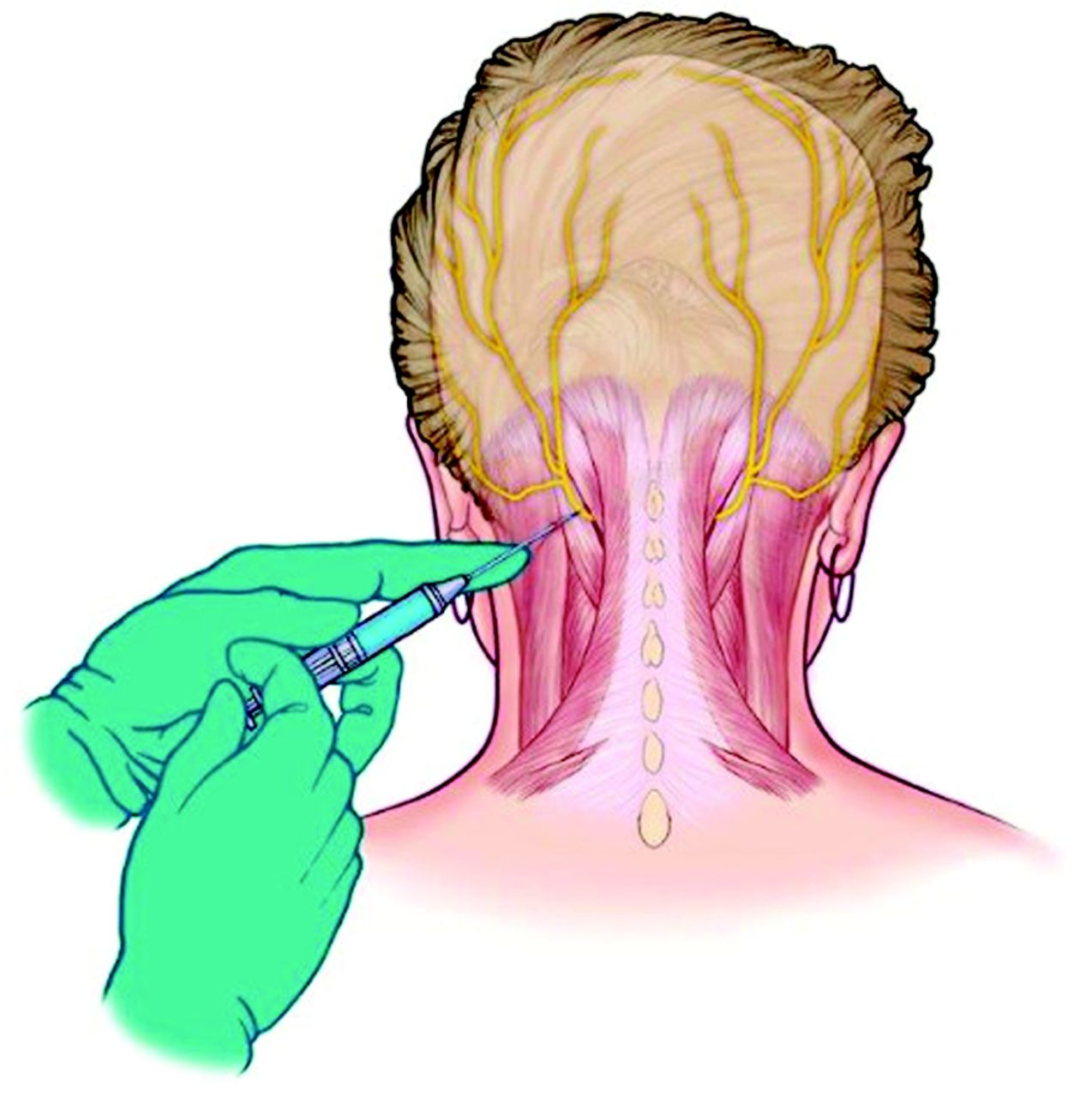
Illustration demonstrating the occipital nerve block procedure.
No current guidelines include GON block in the management of migraine headache1,8, although many studies have researched this, with variable results and conclusions.7,9⇓⇓⇓⇓⇓⇓⇓⇓⇓–19 Four randomized, placebo-controlled trials examining the use of GON block in the treatment of migraine show equivocal results.16⇓⇓–19 The most recent of these studies showed promise.19 We undertook this retrospective cohort study to assess the efficacy of GON block in the acute treatment of migraine headache, having anecdotally experienced good results in our clinical practice.
Methods
Study Design
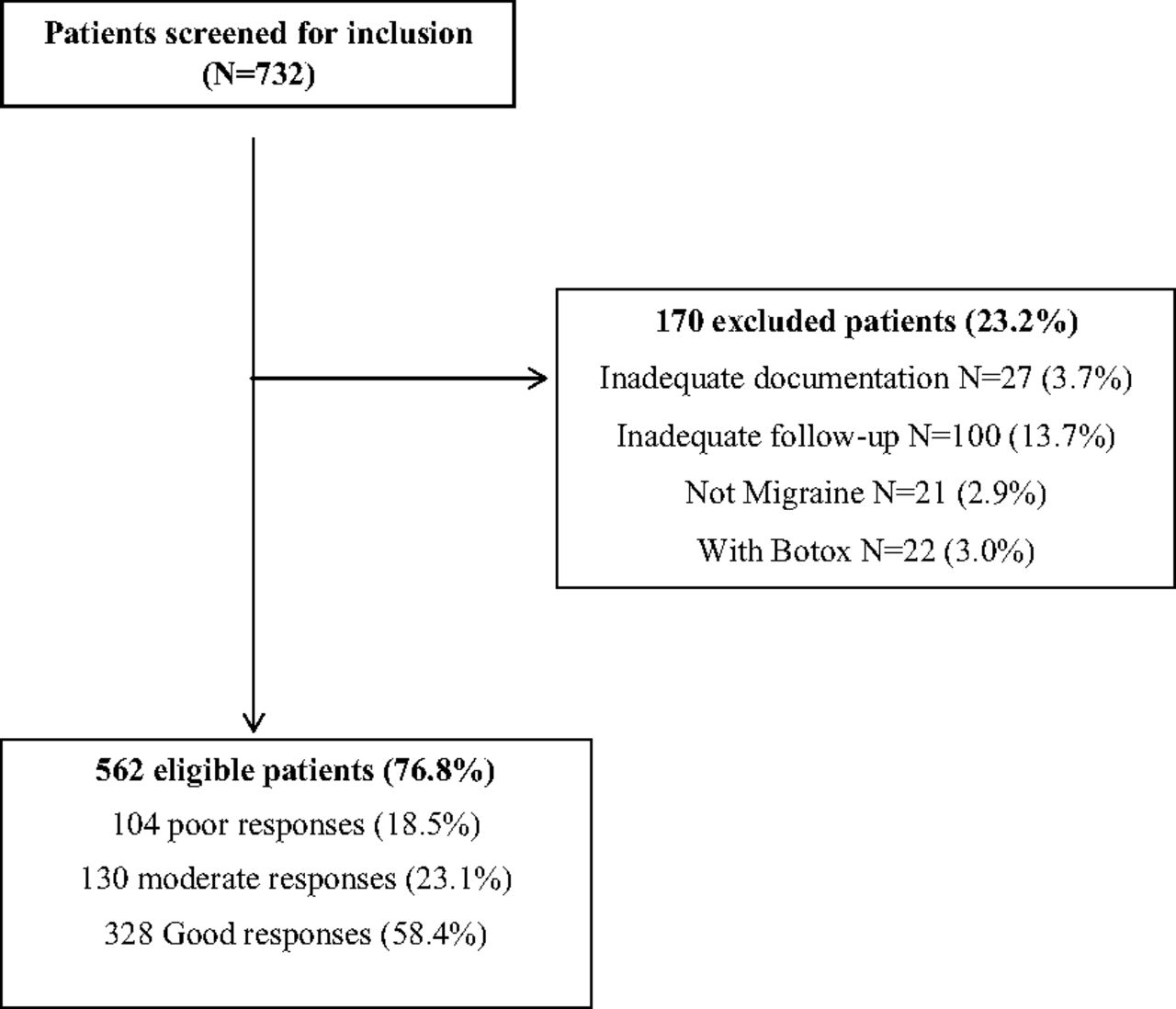
This retrospective cohort study was undertaken at the Mayo Clinic in Arizona. An ethical exemption review was obtained from the Mayo Clinic Institutional Review Board before the study commenced. Patients were identified through a search of the electronic medical record (EMR), and we isolated those who had a GON block procedure performed between January 2009 and August 2014. The records included patients treated at the main hospital campus (neurology and pain clinics) in addition to 4 outpatient primary care practices. In total, 732 patients were identified. Inclusion criteria were (1) age 18 to 100 years; (2) migraine headache as defined by the ICHD-3 (beta); (3) received at least 1 GON block; and (4) attended at least 1 follow-up clinic visit. Exclusion criteria were (1) inadequate documentation regarding follow-up and treatment response, (2) concurrent administration of botulinum toxin injection, and (3) headache did not meet diagnostic criteria. All patients included had a diagnosis of migraine (with or without aura) based on the ICHD-3 (beta) guidelines (Figure 2).3

Study flow diagram.
Data Collection
We performed a detailed chart review. We used methodologic strategies as outlined by Gilbert et al20 and Kaji et al21 to help ensure reliability of data abstraction. One researcher (SMA) was assigned the role of chart abstractor, with an aim to minimize interperson variability in data interpretation and documentation. Before starting the data collection phase, the research team held a meeting to clearly delineate the variables that were to be collected and to develop a standardized form into which the data were inserted. Patient demographics including age, sex, referral source, and the department performing the procedure were collected. Procedures were performed by trained groups within the departments of neurology, pain medicine, and primary care. We documented previous treatment regimens (medication-based and non–medication-based), total number of GON blocks, medication types and doses used, changes in pain scores, and side effects. Several scheduled interim meetings were held to ensure that the quality of the research objective and data collection was being met. A second researcher (MM) repeated the chart review on a subset of patients (n = 50) to ensure a reliable data collection technique without significant interperson variability.
Pain Scores
All patients met criteria for diagnosis of migraine headache based on the ICHD-3 (beta) guidelines, and the majority (91% of the cohort; n = 500) were in acute pain at the time of their occipital nerve block. The remaining patients had onset of acute migraine-related pain within the 3 days before the procedure. This delay was related to referral and appointment waiting times to see the appropriate specialist. Patients rated their headache-related pain (episodic) before and after the procedure using the 11-point Numeric Pain Rating Scale (NPRS), which ranges from 0 (pain free) to 10 (worst pain imaginable).22,23 Pain scores were collected during that same visit immediately before the occipital nerve block procedure. Pain scores were collected again during a follow-up visit, the timing of which ranged between 1 and 4 weeks after the procedure. Change is baseline pain reflected an alteration in pain associated with migraine attacks. Improvement was quantified based on the percentage change from baseline pain score, allowing us to define responses as “minimal” (<30% NPRS point reduction); “moderate” (31–50% NPRS point reduction), or “significant” (>50% NPRS point reduction). These categories are derived from several analytic studies that determined a data-derived value of change in the NPRS that best represents a clinically significant improvement in symptoms.24,25 These studies, measured using a standard 7-point patient global impression of change, demonstrated a reduction of 2 points, or 30%, as clinically important.24,26
Data Analysis
Basic descriptive statistics, frequency (percentage) for categorical data, and mean ± standard deviation for continuous data were tabulated for patient demographic characteristics. The Pearson χ2 test and Fisher exact test were used to compare GON block responses among patients with different characteristics. Univariate and multivariate logistic models and Forrest plots were used to determine and display predictors for good responders. To calculate the number needed to treat (NNT), we compared the 2 groups, that is, the event rate in the “treatment group” versus that in the “control group,” where the treatment group had ≥2 GON blocks. P values <.05 were treated as statistically significant. All analyses were performed using either SAS software version 9.4 (SAS Institute, Inc., Cary, NC) or SPSS version 22.0.0.0 (IBM Corp., Chicago, IL).
Results
Baseline Patient Demographics
We assessed 732 patients for inclusion within this study; of these, 562 patients (76.8%) met inclusion criteria. We excluded from analysis 170 patients (23.2%): 21 patients did not meet criteria for migraine diagnosis based on the ICHD-3 (beta) guidelines; 100 did not attend a follow-up visit; 27 did not have adequate documentation of treatment response in the EMR; and 22 patients received botulinum toxin injections during the same encounter. Demographic and clinical characteristics are outlined in Table 1. A total of 319 patients (56.7%) had >1 GON block, with the average number being 2.34. The neurology department performed 61% of the procedures, primary care performed 22%, and pain medicine and neurosurgery performed the remainder. A combination of steroid and local anesthetic was used in 99.3% of patients; 0.7% received local anesthetic alone.
Baseline Patient Demographics and Clinical Characteristics
Clinical Efficacy
Of the cohort who received GON block, 82% quantified their response to treatment as moderate or significant, indicating a reduction in their baseline pain score of ≥30%. A total of 328 patients (58%) had a significant response, indicating a reduction in baseline pain score of ≥50%. The data set was analyzed to compare treatment responses between the groups, and a multivariate logistic model was used to assess for response predictors.
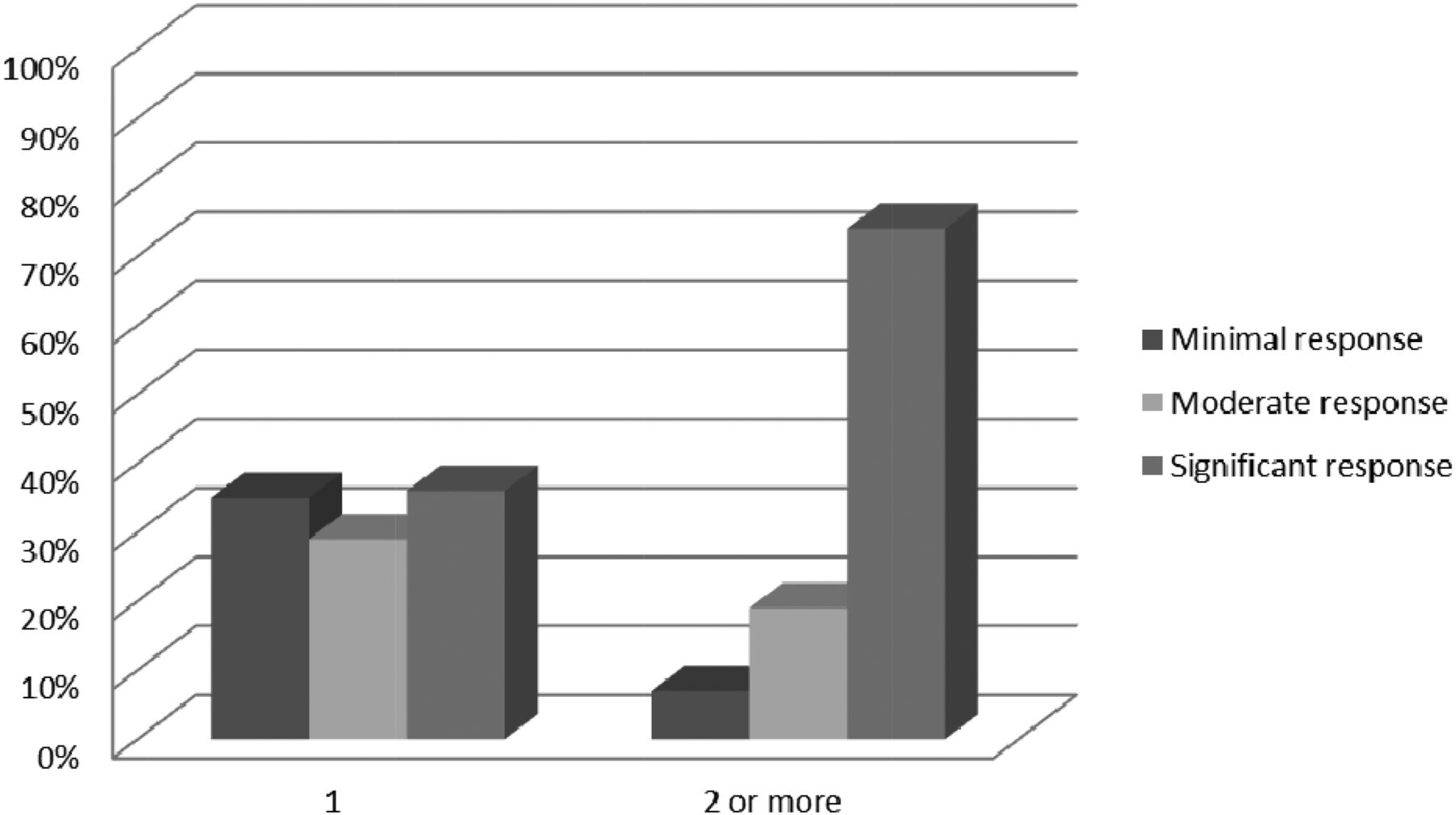
As shown in Table 2, 61% of patients aged <65 years had a significant response to treatment compared with 54% of patients aged ≥65 years (P = .03). Among patients who underwent ≥2 GON blocks, 74% had a significant response, compared with 36% of patients who underwent 1 GOB block alone (P < .001), as shown in Figure 3.
Treatment Response Across the Different Patient Categories

Response rates across the different numbered categories for greater occipital nerve block.
Across the different age categories, patients who underwent ≥2 GON block procedures responded equally well, with an odds ratio of 4.9 to 5.0 (P < .001). Outcomes did not differ based on anesthetic concentration or volume of administration across the different patient groups. Average volumes of administration for the different anesthetic concentrations (doses) is listed in Table 3.
Concentration and Volume of Anesthetic Used
We divided patients based on previous treatment regimens, different medication combinations, and department performing the procedure and found no statistically significant difference in response across the groups.
Number Needed to Treat
No control group was used in this study, given its retrospective design. We were, however, able to compare response rates in those patients treated with 1 GON block with those treated with ≥2 GON blocks. In this case, the NNT was calculated at 2.6.
Safety
Details of the GON block procedure were outlined in a procedural note contained within the EMR. These were reviewed to assess for adverse procedural reactions or complications. Few adverse reactions were reported in the period immediately following the procedure: 10 patients developed vasovagal symptoms that responded to conservative treatment measures, and 25 patients described “burning” at the injection site. No reports of lasting complications or side effects were found within the follow-up visit documentation.
Discussion
The findings from this large, retrospective cohort study suggest that GON block is an effective treatment for acute management of migraine headache. A large percentage of our cohort reported a reduction in both episodic migraine related pain of >30% (from their baseline NPRS value) following treatment with GON block. These results were consistent regardless of sex, age, prior treatments, single or multiple GON blocks, or specialty performing the procedure. A significant correlation was found between receiving ≥2 GON blocks and reduction in pain score (P < .001). In fact, when we compared the rate of response in patients who received 1 GON block with those who received ≥2, the NNT was calculated as 2.6. We hypothesize that repeated peripheral nerve blockade and associated central neuromodulation may increase pain thresholds and thereby improve desensitization. This may have been of particular importance in this older patient cohort. It is important to consider that those patients who obtained good results with 1 procedure are more likely to return for repeated procedures. Another consideration was the duration of time between repeated GON blocks; a short window of time could account for better results. We were unable to obtain this information from the EMR and, as such, cannot account for this as a possible confounder.
No relationship was found between previous treatment regimens (medications, physical therapy, botulinum toxin, acupuncture, or a combination of therapies) and response to GON block (P = .52), suggesting that efficacy of the procedure is not affected by the treatment history. Treatment response was similar across the different age and sex groups. It is worth noting that the mean age of this study population was older than patients in typical migraine studies, which may have had a positive effect on our results as a result of possible cervicogenic triggers/components that may also be addressed with GON blockade.
The majority of the literature pertaining to the use of GON block in the treatment of migraine headache comes from observational studies,8,11⇓–13 most of which showed improvement in headache symptoms, intensity, and frequency. Some studies looked at the efficacy of GON block in the treatment of other headache syndromes, including cluster headache, chronic daily headache, and cervicogenic headache, along with separate pathologies including trigeminal neuralgia and post–dural puncture headache.27 The first double-blind, randomized controlled trial was performed by Piovesan et al16 in 2001; they included 37 patients and compared GON block to placebo as preventive management of migraine, and in a crossover design performed a sham procedure or GON block. Although they found no difference in the number or duration of migraine episodes between the procedures, the group that received GON block experienced a significant reduction in migraine intensity during the 60-day follow-up period. Ashkenazi and Young10 performed a prospective, noncontrolled study to look at the effect of GON block on head pain and allodynia in a cohort of 19 patients with migraine. Both local anesthetic and steroids were used. They noted a significant improvement after the procedure, with 90% of the group documenting relief from head pain. The most recent randomized controlled trial was published in 2016 by Cuadrado et al19 and included 36 patients with chronic migraine treated with bilateral GON block with bupivacaine (n = 18) or a sham procedure with normal saline (n = 18). Anesthetic block was superior to placebo in reducing the frequency of headaches during the week after injection, along with an increase in pressure pain thresholds in various territories.
Prior studies have suggested that different GON block treatment regimens should be compared in order to assess what effect, if any, the addition of steroid or different doses/types of local anesthetics would have on efficacy results. We found no difference in response despite the use of various combinations and doses of local anesthetic. As previously mentioned, only 4 patients within our cohort did not receive corticosteroid as part of their GON block, and therefore we are unable to comment on treatment response using anesthetic alone. We also are unable to draw any comparisons between the 2 procedural strategies.
The scope of this study was to assess, in a retrospective manner, the response to treatment with GON block in a cohort of patients with episodic migraine headache. Change in baseline pain scores reflected a spectrum of pain relief for these patients, including relief of short-term pain, pain from acute attacks, and continuous pain. The use of a validated pain score allowed us to quantify response to treatment in a way that can be interpreted and applied clinically. This study has some limitations we would like to highlight. We were limited by the retrospective design, which precluded us from using a control group. We need to consider the confounding effect that the placebo response may have on our results and mention that innate selection bias existed because of the retrospective design and inclusion criteria. Furthermore, we were unable to divide patients based on the goal of treatment, be it acute or prophylactic management, and as such we did not perform subgroup analysis based on these criteria. We believe the major strength of our study is derived from its large sample size, which, to our knowledge, greatly exceeds that of any previously published article on this topic. We believe this adds power and applicability to our findings, despite the retrospective design.
The suggested biological mechanism by which GON block works to treat the symptoms of migraine relates to modulation of afferent signals to the trigeminal nucleus caudalis, which bridges the gap between sensory regions of the ophthalmic branch of the trigeminal nerve and the greater occipital nerve. Injecting this region with local anesthetic and corticosteroids decreases sensory input to the trigeminal nucleus caudalis. Overall, our findings are very positive in terms of the efficacy of GON block as a treatment option for migraine headache. Our figures for response reflect closely some of the studies mentioned earlier, including Caputi and Firetto,12 who described headache improvement in 85% of their cohort, and Ashkenazi and Young,10 who documented decrease in head pain in 90% of their patients after GON block. Both of these studies had much smaller sample sizes: 27 and 19 patients, respectively.
Conclusion
In a large, retrospective cohort study of patients with migraine headache, GON block used as the sole treatment strategy or as an adjunct to other therapeutic modalities resulted in high rates of clinical response. Large placebo-controlled clinical trials are needed to confirm our findings, along with those from several smaller observational studies and randomized trials. Further data would help to solidify the use of GON block in the treatment of migraine headache and potentially assist with its inclusion within future treatment guidelines Figure 2.
Acknowledgments
The authors acknowledge JoAnn McBroom for her assistance with formatting this manuscript in preparation for publication.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: AJS has received consulting fees from Amgen and eNeura.
To see this article online, please go to: http://jabfm.org/content/31/2/211.full.
- Received for publication May 6, 2017.
- Revision received October 12, 2017.
- Accepted for publication October 17, 2017.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prevalence of Occipital Neuralgia at a Community Hospital-based Headache Clinic
- Peripheral nerve blocks for headache disorders
- The Most Frequently Read Articles of 2019
- Content Usage and the Most Frequently Read Articles of 2018
- Real-Life Observational Studies Provide Actionable Data for Family Medicine