
Abstract
Background: Dartmouth Geisel Migrant Health (DGMH) is a medical student group that provides on-site health services for Spanish-speaking dairy workers in rural Vermont and New Hampshire in conjunction with a federally qualified health center (FQHC).
Study Objective: This project was undertaken to evaluate and improve the services provided by DGMH and the FQHC and to refine understanding of the target population.
Methods: We surveyed 25 workers at 6 collaborating dairy farms to identify health priorities and concerns and perceived barriers and facilitators to health care for these workers. Surveys were administered over 2 weeks in July 2015. Interpreter-mediated appointment and sliding-fee-scale data from a period 7 months that spanned survey administration were also assessed.
Results: Diabetes and hypertension were the most common health concerns. Thirty-two percent of participants reported 10 or more days of depressed mood in the past month. Insurance and language were the most common barriers to health care and employers and on-site clinics were the most common facilitators. Appointments most often addressed women's health, gastrointestinal problems, health maintenance, diabetes, and back pain. Thirty FQHC sliding-fee-scale applications were completed by workers.
Conclusions: These Spanish-speaking dairy-farm workers have many health concerns and perceive substantial barriers to health care. Collaboration between medical students, a rural FQHC, and farm employers provides important services that facilitate health care access among this population.
The United States dairy industry relies on Latino immigrants, with 67.4% of large dairy farms in New York, Pennsylvania, and Vermont employing Spanish-speaking workers.1 These laborers work long hours,1 report physical and linguistic isolation, and many experience stress regarding immigration status.2 Because dairy work is year round, these laborers are ineligible for federally funded health care at migrant health centers.3 These realities make Spanish-speaking dairy workers a highly vulnerable population in the rural northeastern United States.
In conjunction with a federally qualified health center (FQHC), Dartmouth Geisel School of Medicine students formed Dartmouth Geisel Migrant Health (DGMH) in 2010 to offer free, on-site, screening/referral clinics for Spanish-speaking dairy workers in Vermont and New Hampshire. Today, the program also provides interpreter services and care coordination and serves approximately 60 workers on 6 farms.
Project goals were to improve services for and refine understanding of this population. We sought to identify health priorities and concerns and perceived barriers and facilitators to care. We also assessed how interpreter and sliding-fee-scale services compared with population goals.
Methods
Twenty-five Spanish-speaking dairy workers receiving FQHC/DGMH health care took a 28-item survey. Surveys were administered verbally in Spanish on 6 farms; 4 in Orange County, Vermont and 2 in Grafton County, New Hampshire. Farms visits were staggered and repeated over 2 weeks to include all shift workers. The number and type of interpreter-mediated medical appointments facilitated by DGMH and the FQHC was recorded over 7 months (spanning survey administration) as was the number of sliding fee scale applications for these workers. The Dartmouth College Committee for the Protection of Human Subjects approved this project.
Results
Seventeen of 25 participants worked in Vermont and 8/25 in New Hampshire. All respondents were from Southern Mexico, 23/25 were male and average age was 30.6 years (SD = 9.4 y). Workers supported 1 to 12 people in Mexico (mean = 4.9; SD = 2.4). Most participants had worked in agriculture (any country) for more than 3 years (17/25) and 11/25 had worked their current job for more than 3 years. Average workweek was 67.9 hours (SD = 8.8).
Of 13 health concerns assessed (Figure 1), diabetes (14/25) and hypertension (13/25) were most common, followed by weight and eye/vision problems (12/25 each). Depression concerned 11/25 of workers. Of 22 participants willing to discuss mental health, 15 reported 0–3 days of stress, sadness, or lack of hope in the past month; however, 7/22 experienced 10 or more days.
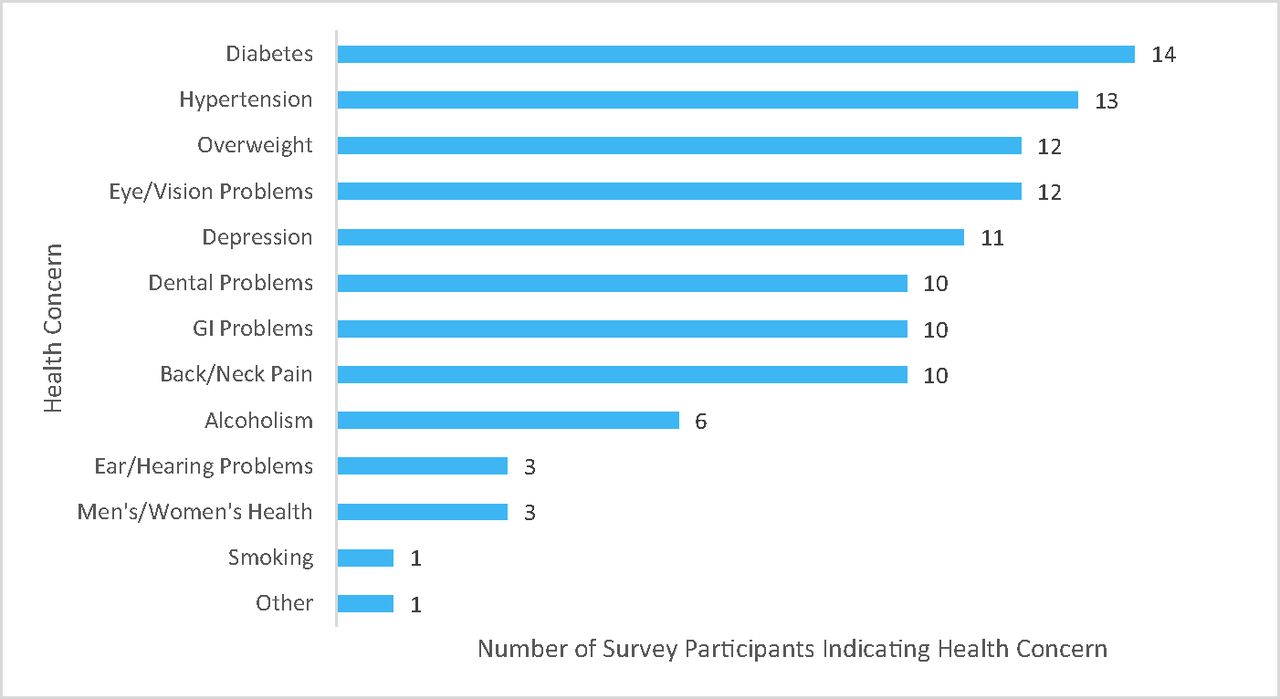
Health concerns indicated by survey participants (n = 25).
Lack of insurance (14/25) and communication issues (13/25) were the most common barriers to health care; employers and on-site clinics were the most frequent facilitators (19/25).
Over 7 months spanning survey administration, 31 interpreter-mediated health care appointments occurred. Topics addressed included: women's health (8/31), gastrointestinal problems (8/31), health maintenance (5/31), diabetes (4/31), and back pain (2/31). During that time, workers completed 30 sliding-fee-scale applications.
Discussion
The main barriers to health care for this group of Spanish-speaking dairy workers in rural Vermont and New Hampshire workers were lack of insurance and communication issues. DGMH combats these barriers by helping workers navigate the FQHC sliding fee scale and providing medical interpreting. A variety of health conditions concerned participants and many of these are being addressed at FQHC appointments.
Of note, this population was more concerned about chronic health conditions than similar workers in other parts of the United States.4 The stability of this population compared with most Spanish-speaking agricultural workers5 presents the opportunity to address concerns that are undiagnosed or underreported elsewhere.4
Spanish-speaking dairy workers in rural Vermont and New Hampshire experience substantial barriers to health care and have many health concerns. An innovative collaboration between medical students, an FQHC, and dairy farms improves access to health care and is perceived as valuable by this population.
Acknowledgments
The authors thank the farm workers for their participation and the farm owners for opening their gates to the project. Special thanks to Little Rivers Health care for their continued dedication to improving the health of migrant and Spanish-speaking farm workers and for their support of Dartmouth Geisel Migrant Health.
Notes
This article was externally peer reviewed.
Funding: Funding was secured through the Dartmouth Geisel School of Medicine. The project was supported by the Department of Community & Family Medicine, the Dartmouth Primary Care Cooperative Research Network, and the Dartmouth Geisel School of Medicine Rural Health Scholars program.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/30/1/91.full.
- Received for publication May 26, 2016.
- Revision received September 21, 2016.
- Accepted for publication September 28, 2016.




{kind=link}