
Abstract
Background: Ambulatory visits to dermatologists and primary care physicians (PCPs) may improve melanoma outcomes through early detection. We sought to measure the effect of dermatologist and PCP visits on melanoma stage at diagnosis and mortality.
Methods: We used data from the database linking Surveillance Epidemiology and End Results (SEER) and Medicare data (1994 to 2005) to examine patterns of dermatologist and PCP ambulatory visits before diagnosis for 18,884 Medicare beneficiaries with invasive melanoma or unknown stage at diagnosis. Visits were assessed during the 2-year time interval before the month of diagnosis. We examined whether dermatologist and PCP visits were associated with diagnosis of thinner melanomas (defined as local stage tumors having Breslow thickness <1 mm) and lower melanoma mortality.
Results: Medicare beneficiaries visiting both a dermatologist and PCP before diagnosis had greater odds of diagnosis of a thin melanoma (adjusted odds ratio, 1.26; 95% confidence interval, 1.12–1.41) and lower melanoma mortality (adjusted hazard ratio 0.66, 95% confidence interval, 0.57–0.76) compared with those without such visits. The mortality findings were attenuated once stage at diagnosis was adjusted for in the multivariable model.
Conclusion: Improved melanoma outcomes among Medicare beneficiaries may depend on adequate access and use of dermatologist and PCP services.
There were more than 70,000 new cases of melanoma diagnosed in 2011, with almost 9,000 deaths.1 Both the incidence and mortality of melanoma have continually increased for the past 30 years.1 The prognosis of melanoma is highly dependent on the stage at which it is diagnosed. Thin lesions (Breslow thickness <1 mm) have 10-year survival rates approaching 90%, whereas 10-year survival for people with metastatic disease is <20%.2
Physicians may affect stage at diagnosis by providing skin screenings and by promptly evaluating lesions discovered by patients.3⇓–5 Studies have found that melanomas detected by dermatologists are thinner than those identified by patients.6,7 Other studies have shown that geographic areas having greater numbers of dermatologists and primary care physicians have detection of melanoma at an earlier stage.8⇓–10 Despite this, no studies to date have demonstrated reduced mortality from skin screenings, and the US Preventive Services Task Force concluded that there is currently insufficient evidence to recommend routine skin screening.11
Previous studies examining the effects of physician services have had important limitations. Studies linking increasing physician supply to improved melanoma outcomes are subject to ecological fallacy: it is not possible to determine whether individuals with better outcomes in these studies are the same individuals who received more care from physicians. Studies linking physician supply to specific health outcomes may be confounded by socioeconomic status, which often is correlated with physician supply. In addition, studies examining physician services often fail to be population based.3,6,7
Understanding the affect of physician services on melanoma outcomes is important as our health care system evolves. The supply of primary care physicians as a percentage of the US physician workforce is in steep decline.12 Some have questioned whether the supply of dermatologists is adequate to meet demand.13,14 Some studies suggest that patients may face delays obtaining dermatologic care,15 which could result in poor melanoma outcomes.16
We used data from the Surveillance, Epidemiology and End Results program (SEER)–Medicare linked database to examine patterns of physician ambulatory care before diagnosis and its effect on melanoma outcomes. We hypothesized that patients receiving dermatologic care before diagnosis would have an earlier stage at diagnosis and improved melanoma survival. We also hypothesized that primary care visits before diagnosis would similarly be associated with improved melanoma outcomes.
Methods
Study Sample
This study used a retrospective cohort design to assess physician services and melanoma outcomes using the 2008 SEER-Medicare linked dataset. Patients diagnosed with their first cancer as melanoma within the SEER program between April 1994 and December 2005 represented the cohort of interest (n = 81,505). Those previously diagnosed with cancers (other than nonmelanoma skin cancers) were excluded. We also excluded patients who were diagnosed with other cancers within a year after their diagnosis of primary melanoma (n = 8267). Most people qualify for Medicare at age 65, and to help ensure that subjects had at least 24 months of Medicare claims before their cancer diagnosis we excluded subjects diagnosed with melanoma before age 67 (n = 24,809). Because of clinical complexity, we excluded people who were eligible for Medicare because of end-stage renal disease (n = 22). Consistent with other SEER studies,17 we also excluded melanoma cases in which the diagnosis was based solely on death certificates or made at autopsy (n = 182). Since we examined Medicare claims of patients in the 24-month period before the month of diagnosis, we further excluded subjects enrolled in a Medicare health maintenance organization within the 24 months before their cancer diagnosis (n = 13,956) because these subjects have no claims history during the period of their enrollment in the health maintenance organization. We also excluded subjects who did not have continuous Medicare Part A and Part B coverage during the 24 months before diagnosis (n = 2894). Finally, because the malignant potential of in situ melanomas is uncertain, we excluded people with in situ lesions (n = 12,491), leading to our final analytic sample (n = 18,884). This study was approved by the appropriate institutional review boards.
Ambulatory Care Visits
There is significant empiric evidence that preventive care in general, and cancer screening in particular, is overwhelmingly delivered in the ambulatory setting.18⇓⇓⇓⇓⇓⇓⇓–26 We therefore examined Medicare claims (National Claims History database) for the following ambulatory-based evaluation and management services representing physician office visits: 99201 to 99205, 99211 to 99215, 99354 to 99359 (patient office visits); 99241 to 99245, 99271 to 99275 (outpatient consultations); 99301 to 99303, 99311 to 99313, 99315 to 99316, 99312 to 99323, 99331 to 99333 (nursing/boarding facility visits); 99341 to 99345, 99347 to 99350 (home visits); 99387, 99397, 99401 to 99402, 99411, 99412, 99420, 99429 (preventive care visits) 99450, 99455, and 99456 (Disability evaluations).
Similar to prior research, we identified the physician specialty associated with each claim using the Health Care Financing Administration Medicare provider specialty field found among claims in the National Claims History database.27,28 We defined primary care providers as those having the following specialties: general practice, family medicine, primary care internal medicine, geriatric medicine, and obstetrics/gynecology (OB/GYN). We classified OB/GYN as primary care because 64.3% of visits to such physicians by older women are for routine follow-up or preventive care.29 Because there may be controversy regarding the primary care role of OB/GYN for older women, we repeated our analysis excluding OB/GYN from our definition of primary care.
For each subject, we determined whether there was an ambulatory claim for either a primary care physician (PCP) or dermatologist during a 24-month period before the month of melanoma diagnosis. Our measures of dermatologist and PCP visits were intended to reflect regular ongoing care rather than care specifically associated with diagnosing melanoma. On the basis of the claims history, each subject was placed into 1 of 4 mutually exclusive categories: previous visit to PCP, previous visit to dermatologist, previous visits to both PCP and dermatology, and no previous visits to either PCP or dermatology.
Thin Melanoma Diagnosis and Mortality
We examined the likelihood that subjects were diagnosed with thin melanomas. We classified thin melanomas as localized lesions with Breslow thickness <1 mm. Subjects classified as having non–thin melanomas included those with regional disease (regional lymph nodes or satellite nodules) or distant metastatic disease at diagnosis. The non–thin melanomas classification also included those having localized lesions at a depth that was intermediate (Breslow thickness 1–2 mm) or thick (Breslow thickness >2 mm) because of their less favorable prognosis.30⇓–32
The SEER registry also provided data on vital status for all subjects through 2005. Date and underlying cause of death were obtained through linkages with state vital statistics. Survival was measured from date of diagnosis to date of death or last known follow-up (December 31, 2005). For assessment of melanoma mortality, those people who died of causes other than melanoma or who were alive on December 31, 2005, were censored. The median follow-up time (time from diagnosis till death or last follow-up) was 31 months.
Statistical Analysis
We examined the relationship between previous PCP and dermatologist visits and diagnosis of thin melanomas using multivariable logistic regression. Patients with missing stage at diagnosis were excluded from this analysis (n = 982). We examined the odds of thin melanoma diagnosis (and 95% confidence intervals [CIs]) for the 4 categories of previous PCP and dermatologist visits: neither PCP nor dermatologist, PCP only, dermatologist only, and both PCP and dermatologist. The following variables were used as potential confounders in multivariable models: age at diagnosis, sex, race/ethnicity (derived from SEER variables), marital status at diagnosis, census-derived measures of median household income at the zip code level (categorized by quintiles within each registry), educational attainment at the zip code level (percentage of people with less than a high school education, categorized by quintiles within each registry), year of diagnosis, metropolitan statistical area, SEER geographic registry, Charlson comorbidity index33,34 (determined from both inpatient and outpatient claims), prior influenza vaccination (as a marker of preventive behaviors),35,36 and histologic category.
The relationship between PCP/dermatologist visits and melanoma mortality was analyzed using Kaplan-Meier survival curves and Cox proportional regression models adjusting for the potential confounding factors described above. The proportional hazards assumption was checked by the graphical and numerical method developed by Lin et al.37 In our analysis of mortality, we controlled for differences in treatment modalities recorded in SEER, including surgery (surgery with wide excision [>1.0 cm], surgery without wide excision or with unknown margins, none or unknown surgery), receiving lymph node resection (including sentinel lymph node), and receiving radiation therapy. To determine whether observed associations between physician visits and lower melanoma mortality were explained primarily by earlier stage at diagnosis, multivariable Cox models were first performed, excluding stage at diagnosis and then repeated with stage. The degree to which the hazard ratios differ between these 2 models is an indication of how much of the mortality differences are the result of earlier stage at diagnosis. All analyses were performed using SAS software version 9.3 (SAS Institute Inc., Cary, NC) or R software version 2.15.0 (available from http://www.r-project.org/).
Results
Diagnosis of Thin Melanoma
The mean age of the sample subjects was 76.9 years (standard deviation, 6.6 years) and 11,283 of 18,884 subjects (59.7%) were men (Table 1). Almost half of the subjects had melanoma diagnosed as invasive but thin lesions. Most subjects diagnosed with melanoma had claims for previous visits with a PCP, either alone or in conjunction with a dermatologist. For 2419 of the 18,884 subjects (12.8%), however, there was no claim for PCP or dermatologist services in the 24-month period before diagnosis. Of those who had a prior visit with a PCP (n = 15,471), 5920 (38.3%) had a dermatology visit. Of those who did not have a prior visit with a PCP (n = 3413), 994 (29.1%) had a dermatology visit (P = <.0001, χ2 test, for differences in dermatology visits by PCP visit).
Subjects having both a PCP and dermatologist visit, or just a PCP visit, in the 24-month period before diagnosis were more likely to have a diagnosis of thin melanoma compared with subjects without any visits (Table 2). When adjusting for potential confounders, those having both PCP and dermatologist visits before diagnosis had 26% greater odds of a thin melanoma diagnosis. Other predictors of thin melanoma diagnosis included younger age, more recent time of diagnosis, lower comorbid illness burden, prior influenza vaccination, white race (black race, Hispanic ethnicity, and Asian/American Indian/Pacific Islander were less likely to have early stage diagnosis), being married, and living in a zip code with higher educational attainment. Excluding OB/GYN from our definition of PCP visits had no effect on our findings. There was no difference in the odds of thin melanoma diagnosis when comparing patients with a dermatologist visit only versus PCP visit only (adjusted odds ratio, 1.07; 95% CI, 0.92–1.25).
Mortality
Vital status for all study patients (n = 18,884) at the end of follow-up was as follows: alive, n = 12,820 (67.9%); died of melanoma, n = 2083 (11.0%); died of other causes, n = 3853 (20.4%); unknown if died, n = 128 (0.7%). The proportions of persons dying of melanoma by category of physician utilization were as follows; PCP, 1,133 deaths per 9,485 persons (11.9%); dermatologist, 100 deaths per 981 persons (10.2%); both PCP and dermatologist, 481 deaths per 5,888 persons (8.2%); and neither, 369 deaths per 2,402 persons (15.4%). Survival varied by category of physician utilization (P < .0001, log rank test) (Figure 1).
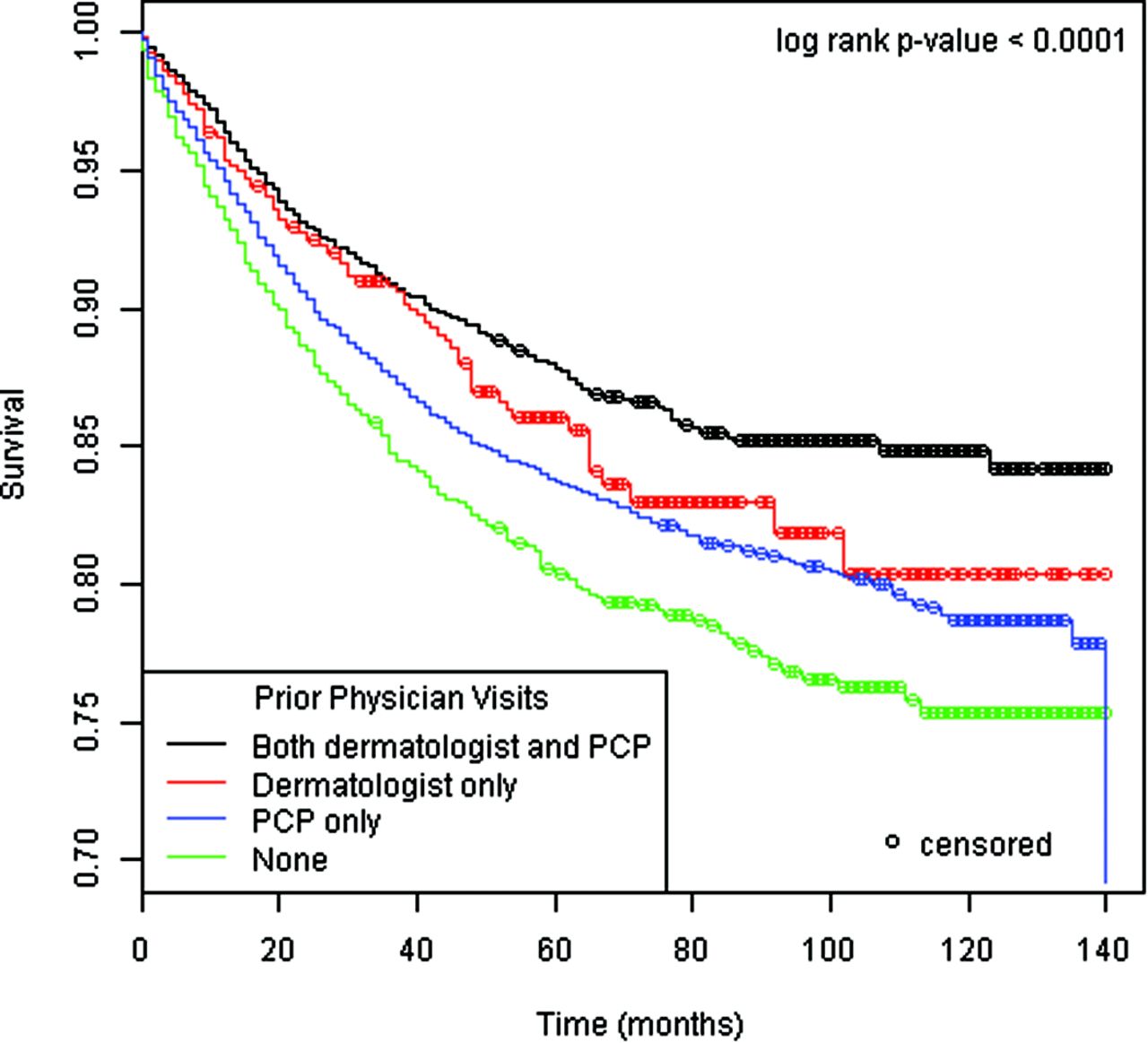
Melanoma-specific survival. PCP, primary care physician.
In the analysis adjusting for all factors except stage (model 1), prediagnostic visits to PCPs alone or both PCPs and dermatologists were significantly associated with reductions in melanoma mortality (Table 3). Prediagnostic visits to both dermatologists and PCPs were associated with 34% lower melanoma mortality (adjusted hazard ratio, 0.66; 95% CI, 0.57–0.76). These findings were attenuated once stage at diagnosis was included in the model (model 2), but remained significant, reflecting the potential effects of physician visits in reducing mortality beyond those associated with earlier stage diagnosis. Other factors associated with reduced mortality included female sex, younger age, being married, lower comorbid burden, and having favorable histologic subtypes, such as lentigo maligna or superficial spreading melanoma. When repeating our analysis to exclude OB/GYN from our definition of primary care, we found that in model 2 visits to PCPs only were no long statistically significant. There was no substantive difference in results for model 1.
Discussion
Subjects having ambulatory visits to both PCPs and dermatologists before diagnosis were more likely to be diagnosed with thin melanomas. Likewise, those having previous visits to both PCPs and dermatologists had 34% lower melanoma mortality, a finding that was explained in part, but not entirely, by earlier stage diagnosis.
Physicians can theoretically affect melanoma mortality through screening exams of asymptomatic patients, timely evaluation of lesions discovered by patients, and patient education about melanoma. Lesions identified by physicians tend to be thinner than those discovered by patients.6⇓–8,38,39 Our results support the hypothesis that ambulatory physician visits are associated with thinner melanoma diagnosis and subsequent improved melanoma survival.
Studies have suggested that dermatologists provide greater accuracy during skin examinations40 and diagnose melanoma at earlier stage than other physicians.41 Our study did not find any difference in stage at diagnosis for subjects having ambulatory visits to only dermatologists compared with those having visits only to PCPs. The best outcomes, however, were seen among patients who had previous ambulatory visits to both dermatologists and PCPs, suggesting that these services can complement one another. For example, PCPs may facilitate referrals to dermatologists, and we found that dermatologist visits were more common for patients who had seen PCPs before diagnosis.
Although dermatologists may provide more accurate skin examinations relative to PCPs, some have argued that their affect is more limited because of fewer contacts with patients and thus fewer opportunities to diagnose melanoma.42 Our results are consistent with this argument: more than half of the patients diagnosed with melanoma had contact with only their PCP in the 24-month period before diagnosis. It is uncertain whether educational programs can improve the diagnostic accuracy of skin examinations by PCPs43 and whether such screenings can ultimately improve outcomes.44
The association between PCP and dermatologist visits and lower melanoma mortality seemed to be mediated in part by earlier stage diagnosis. PCP and dermatologist visits after diagnosis could also theoretically affect adherence to melanoma treatment and subsequent surveillance, but this was not examined in our study. Whether ambulatory visits to dermatologists and PCPs after diagnosis affects treatment or surveillance of melanoma is unknown.
Some have argued that greater physician surveillance is leading to overdiagnosis of melanoma, detecting early stage melanomas with limited malignant potential.45 Overdiagnosis of cancer is suspected when there is an increased incidence of early stage cancers but no corresponding increase in late-stage disease or cancer mortality.46 While overdiagnosis is one potential explanation for our findings, the increasing incidence of melanoma in patients 65 years and older has been accompanied by increased incidence of late-stage disease and melanoma mortality.47
A diagnosis of thin melanoma was associated with younger age, lower comorbidity, prior influenza vaccination, being married, living in a zip code with higher educational attainment, and more recent diagnosis. A diagnosis of non–thin melanoma was more common among minorities, including African Americans, Asian/American Indian/Pacific Islanders, and Hispanics. In prior studies, late-stage melanoma diagnosis has been similarly associated with older age,8 being unmarried,48,49 lower socioeconomic status,50⇓–52 and lack of health insurance,53,54 The trend over time of diagnosis at an earlier stage may be the result of improved detection of melanomas or could be explained in part by improved SEER reporting of early stage lesions.55
This study has a number of limitations that should be considered when interpreting the findings. First, this study was limited to patients ages 67 years and older with Medicare fee-for-service insurance and living in SEER registries, and findings may be different for other populations. Associations between physician visits and lower mortality could result if healthier people are more likely to visit PCPs. Our models adjusted for prior influenza vaccination as a proxy for healthy behaviors in effort to minimize this potential bias, but residual confounding is still possible. The SEER-Medicare database lacks potentially important confounders. For example, we lacked data on severity of comorbid illness, which could affect survival, and data on melanoma risk factors (skin type, precursor lesions, etc.) that could affect stage at diagnosis. Nor did we have detailed information on the specific nature of the physician visits assessed or the reasons that patients were seeing dermatologists.
Conclusion
We found that previous ambulatory visits to both dermatologists and PCPs were associated with a greater likelihood of a diagnosis of thin melanoma and reduced melanoma mortality. People with previous visits to both a dermatologist and a PCP had the best melanoma outcomes. Further study is warranted to understand the effect of physician utilization on melanoma outcomes.
Notes
This article was externally peer reviewed.
Funding: This study was supported in part by the American Cancer Society (RSGHP-08-141-01-CPHPS).
Conflict of interest: none declared.
See Related Commentary on Page 623.
- Received for publication January 21, 2013.
- Revision received April 25, 2013.
- Accepted for publication May 24, 2013.




{kind=link}