
Abstract
Objective: Assessing health literacy during the clinical encounter is difficult. Many established instruments are lengthy and not practical for use in a busy practice setting. Our objective was to compare the performance of 3 health literacy screening questions against the Short Test of Functional Health Literacy for Adults (S-TOFHLA) in an urban, ethnically diverse primary care practice-based research network.
Methods: A convenience sample of patients in clinics in the Detroit area were recruited to complete a questionnaire that included the S-TOFHLA and 3 items similar to the Chew screening questions. Area under the receiver operating characteristic (AUROC) curves compared the test characteristics of the screening questions to the S-TOFHLA.
Results: The participation rate was 92% (N = 599). Most participants were women (65%) and African American (51%); 51.8% had a household annual income of <$20,000. Almost all (96.7%) had an adequate score on the S-TOFHLA. The screening question with the largest AUROC (0.83; 95% CI, 0.70–0.95) was “How often do you have someone help you read instructions, pamphlets or other written materials from your doctor or pharmacy?”; the AUROC for all 3 questions was 0.90 (95% CI, 0.85–0.95).
Conclusions: Self-administration of the 3 screening questions demonstrated high performance compared with the 36-item S-TOFHLA interview instrument. These screening questions should help providers identify patients who may need extra support to follow health prescriptions.
Health literacy often is defined as the ability to obtain, process, and understand the basic information and services needed to make appropriate health decisions.1 It is possible that as many as half of the American population lacks the literacy skills to take appropriate health care actions.2 Although race/ethnicity and speaking a language other than English before beginning school are associated with limitations in health literacy,3 large segments of white, native-born Americans also have marginal or inadequate health literacy.2,4
Health literacy is a strong predictor of health status; a systematic literature review5 revealed associations of lower health literacy with infrequent receipt of preventive services, increased hospitalizations, more frequent use of emergency care, and poorer control of chronic diseases such as diabetes, hypertension, and asthma. Lower health literacy also is associated with unhealthy behaviors such as smoking,6 less patient knowledge about their health problems,2,7 and more medication errors.3 People with lower health literacy are at risk for increased mortality as well.8,9
Low health literacy may also increase health care costs. In 2004, Weiss and Palmer10 estimated that mean charges among Medicaid patients with very low literacy skills were approximately 3 times higher than those with better literacy skills. These included charges for hospital, emergency department, short-term nursing home, and physician care in addition to charges for laboratory tests, radiography, prescriptions, and durable medical equipment.
Education is not a reliable indicator of health literacy.2,6 Thus, health care providers and researchers have been searching for a brief and valid screening tool to identify patients with inadequate health literacy.11⇓⇓⇓–15 Although some studies provide evidence that one or more screening questions can be used to identify individuals with literacy needs,16 the research demonstrates that performance on screening tests varies across different populations.1,13 Our goal was to evaluate the performance of an adaptation of the screening questions defined by Chew et al13 for use in a diverse sample recruited from primary care clinics in a local practice-based research network. In this study we used the Short Test of Functional Health Literacy for Adults (S-TOFHLA)17 as a reference standard in an urban, ethnically diverse primary care patient population.
Methods
Patients were recruited from 6 family medicine clinics that are members of the MetroNet practice-based research network in the metropolitan Detroit area. A convenience sample of 100 consecutive patients were recruited from each of the 6 clinics (including 1 federally qualified health center), representing suburban to urban patient populations over the period of January through March 2009. Inclusion criteria were age between 18 and 80 years; fluent in English; and being a patient at a family medicine clinic. Patients who completed the self-administered questionnaire were given $5 for their time. The study received ethics approval from the institutional review boards of Wayne State University and a local community hospital that sponsored the institutional review board of record for 3 of the participating MetroNet sites.
The questionnaire contained 3 sections: demographics, the 3 questions adapted from Chew et al,13 and the 36-item S-TOHFLA,17 which is a validated measure of health literacy (when read aloud to patients). Chew et al reported a sample of outpatient veterans affiliated with a specific hospital; in 2 questions their items referred to “hospital materials.” Similar to others,3 we adapted the questions from Chew et al to our study population and circumstance. We replaced the reference to “hospital” with “doctor and pharmacy.” Thus, the 3 health literacy assessment questions we used were (1) How often do you have problems learning about your medical condition because of difficulty understanding written information? (“problems learning”); (2) How confident are you filling out medical forms by yourself? (“confident with forms”); and (3) How often do you have someone help you read instructions, pamphlets, or other written materials from your doctor or pharmacy? (“help read”). Each of the 3 screening questions was scored on a 5-point Likert scale. The questionnaire was usually completed in 10 to 15 minutes.
Each of the S-TOFHLA questions was scored 1 if correct and 0 if wrong, with a possible score ranging from 0 to 36. On the basis of the S-TOFHLA, patients were classified as having inadequate (score of 0–16), marginal (score of 17–22), or adequate (score of 23–36) health literacy.1 Receiver operating characteristic curves were used to compare each of the 3 screening items to the S-TOHFLA. These curves plot sensitivity versus specificity, demonstrating the trade-off between sensitivity and specificity at different thresholds for diagnosing health literacy. Each question was examined individually and in combination with the other questions to determine the combination with optimal sensitivity and specificity in identifying inadequate health literacy in the study sample. Confidence intervals of the diagnostic measures were determined using a formula for small sample size.18
Results
Of the 653 eligible patients who were invited to participate, 599 (92%) completed the questionnaire. Table 1 describes the sample: 65% were women; 51% were African American and 43% were white; 52% had a household income of <$20,000; and 51% had some college education. The mean age was 45 years. Using the S-TOFHLA, 15 (2.5%) were identified as having inadequate health literacy, 5 (0.8%) as having marginal health literacy, and 579 (98.7%) as having adequate health literacy. Based on the S-TOFHLA, inadequate literacy was observed in 12 patients with less than a high school education (86%), 1 patient among high school graduates (7%), and 1 patient with some college education (7%) (data not shown).
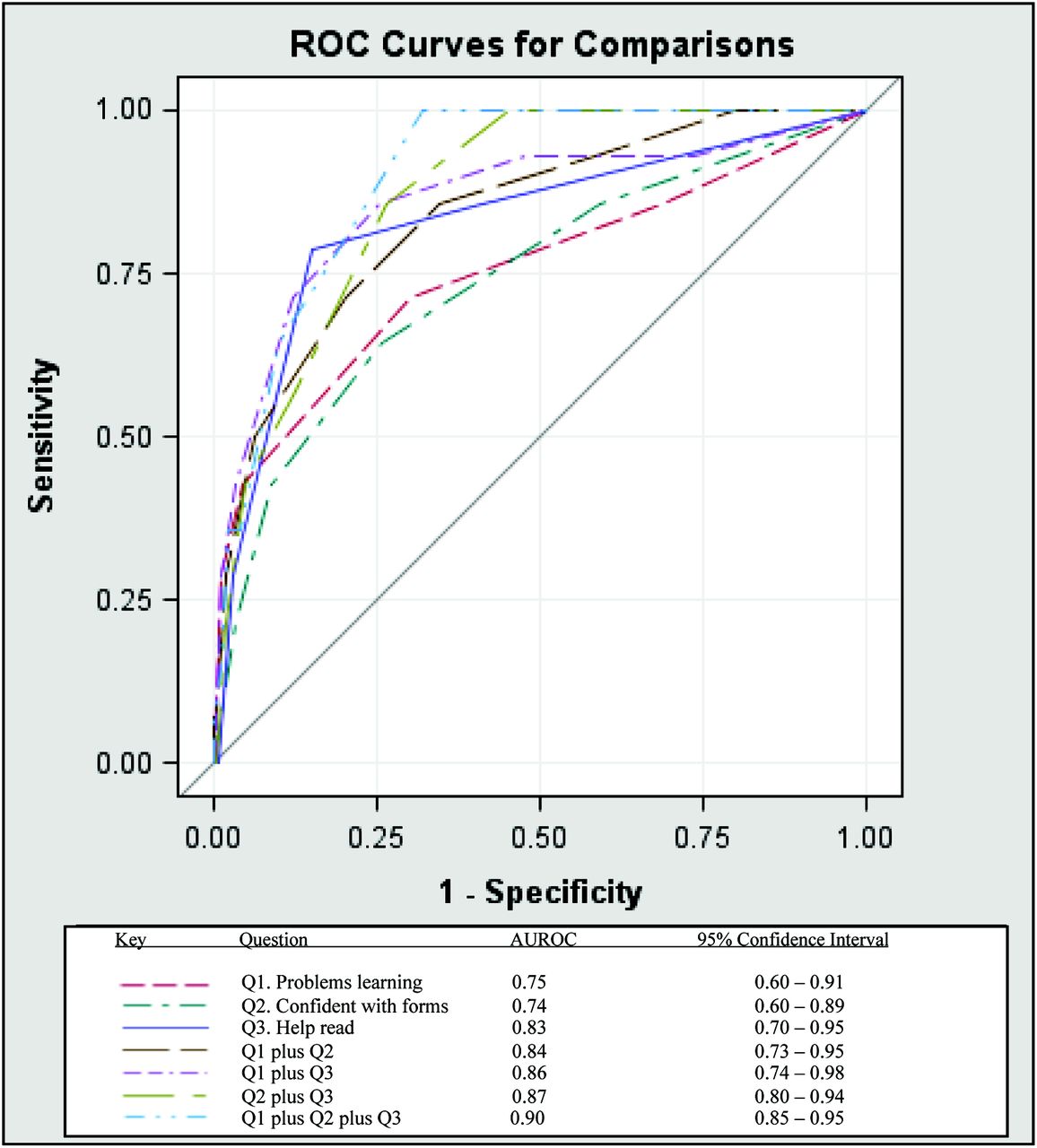
The area under the receiver operating characteristic curves (AUROCs) for each of the 3 screening items and combinations of these items are presented in Figure 1. The item “help read” had the largest AUROC (0.83; 95% confidence interval, 0.70–0.95). However, the confidence intervals overlapped for the AUROCs derived from each of the other 2 items and from the different combinations of the 3 items.
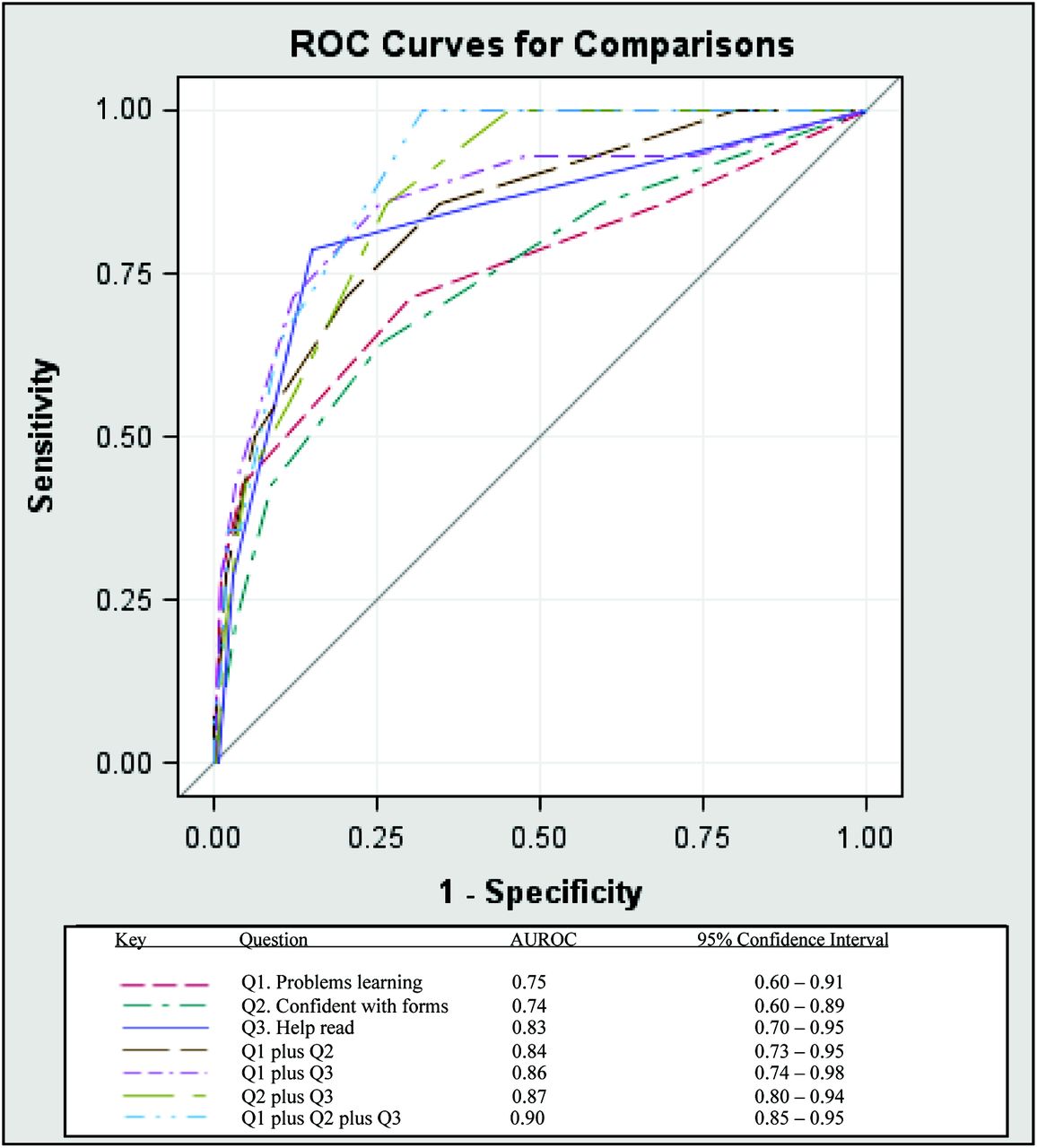
Performance of 3 health literacy screening questions compared to the Short Test of Functional Health Literacy in Adults (S-TOFHLA). AUROC, area under the receiver operating characteristic curve; ROC, receiver operating characteristic.
Discussion
Enhancing literacy may be an effective mechanism to reduce health disparities,18 and identifying individuals with inadequate health literacy is a priority to reduce their morbidity and mortality. Our study examined the utility of using 3 screening questions11,13 in a racially and socioeconomically diverse sample of primary care patients in metropolitan Detroit, a population different from those studied in previous reports. We also tested the feasibility of self-administration (rather than interview) in busy clinical settings, with the plan to recommend the clinical use of these questions to identify inadequate health literacy at the patient's initial (intake) visit.
We found that the 3 self-administered screening questions performed as well as the 36-item S-TOFHLA, and the question, How often do you have someone help you read instructions, pamphlets or other written materials from your doctor or pharmacy? (“help read”) had the largest AUROC as a single item. In contrast, Chew et al11,13 reported that the “confident with forms” items had the largest AUROC compared with the S-TOFHLA. However, their sample of veterans receiving care at Veterans Affairs hospital was interviewed,13 whereas ours was a sample from community primary care practices completing a self-administered written questionnaire.
The prevalence of inadequate health literacy (2.5%) in our urban population using the S-TOFHLA was low compared with other studies using the same instrument.11,13 This was not anticipated given the low income level of many of our respondents. This may have occurred if the S-TOFLA failed to detect people with marginal literacy.2 Our results might also have differed from published S-TOFLA findings because we administered the questionnaire in a self-administered written format rather than reading it aloud. Three of our MetroNet sites also collected data using the Newest Vital Sign2 health literacy assessment; although those data are not reported here, the Newest Vital Sign data from those sites indicated a proportion of inadequate health literacy more consistent with other reports.2
Conclusion
In primary care clinic settings where resources and time are limited, the use of any or all of the 3 screening questions may be valuable to providers seeking to easily identify patients who may have low health literacy. Our findings support the conclusion that health literacy cannot be assumed based on a patient's sociodemographic characteristics. Clinical providers' awareness of patient health literacy is important to identify those patients who may need extra support to make health care decisions or follow medical prescriptions.
Notes
-
This article was externally peer reviewed.
-
Funding: none.
-
Conflict of interest: none declared.
- Received for publication February 1, 2013.
- Revision received May 20, 2013.
- Accepted for publication May 24, 2013.




{kind=link}