
Abstract
Purpose: Primary care practices are an ideal setting for reducing national smoking rates because >70% of smokers visit their physician annually, yet smoking cessation counseling is inconsistently delivered to patients. We designed and created a novel software program for handheld computers and hypothesized that it would improve clinicians' ability to provide patient-tailored smoking cessation counseling at the point of care.
Methods: A handheld computer software program was created based on smoking cessation guidelines and an adaptation of widely accepted behavioral change theories. The tool was evaluated using a validated before/after survey to measure physician smoking cessation counseling behaviors, knowledge, and comfort/self-efficacy.
Results: Participants included 17 physicians (mean age, 41 years; 71% male; 5 resident physicians) from a practice-based research network. After 4 months of use in direct patient care, physicians were more likely to advise patients to stop smoking (P = .049) and reported an increase in use of the “5 As” (P = .03). Improved self-efficacy in counseling patients regarding smoking cessation (P = .006) was seen, as was increased comfort in providing follow-up to patients (P = .04).
Conclusions: Use of a handheld computer software tool improved smoking cessation counseling among physicians and shows promise for translating evidence about smoking cessation counseling into practice and educational settings.
One third of the world's adult population smoke cigarettes (>1.1 billion people), resulting in nearly 5 million deaths annually, with projections of 10 million annual deaths if current global smoking patterns continue.1 Previous declines in smoking rates have stalled over the past 5 years,2 and nearly half of the United States' 45.3 million current smokers are expected to die prematurely as a result of smoking.
A recent Institute of Medicine report calls for implementing successful cessation methods and approaching smoking as a disease management issue,3 yet it has been difficult to translate these recommendations into clinical practice. Excellent evidence-based guidelines for smoking cessation counseling have been available for more than 2 decades, and an update was published in 2008.4,5 Distribution of paper-based guidelines seems to have little effect; the National Cancer Institute spent nearly $10 million distributing guidelines in the 1980s, with little impact on physician practices.6 Wide dissemination of Public Health Service guidelines to all U.S. physicians in 2000 also led to no appreciable difference in rates of physicians asking patients about tobacco use or counseling them to quit.7
Clinicians in primary care have the potential to impact national smoking rates; >70% of smokers visit their physician annually.8 Despite having these guidelines for smoking cessation available, physicians continue to perform poorly in delivering smoking cessation counseling to their patients. Goldstein et al.9 found that a majority of community-based primary care physicians reported asking (67%) and advising (74%) their patients about smoking, but rates of assisting (35%) or arranging (8%) follow-up were much lower. Several additional studies have confirmed these low rates of recommended physician smoking cessation counseling,10⇓⇓⇓⇓⇓–16 demonstrating the need for innovative, dynamic, and accessible methods to translate and disseminate smoking cessation counseling information to clinicians.
Personal digital assistants (PDAs) and smartphones (eg, iPhones and Android-powered phones) can be useful in helping clinicians apply information at the point of care. We have previously piloted the delivery of basic smoking cessation guidelines and prescribing information on these devices, with promising results.17,18 PDA-based interventions with carefully synthesized information and interactive processes have the potential to mitigate time, training, and confidence barriers that frequently are cited as reasons for lack of preventive services being delivered in primary care settings.19⇓⇓⇓–23
To improve smoking cessation counseling in primary care, we designed and developed the Modular Lifestyle Intervention Tool (MLIT), a novel software program for hand-held computers that expanded on our previous work by providing a scripted, algorithmic approach to smoking cessation counseling. We hypothesized that the MLIT would improve clinicians' ability to provide patient-tailored counseling at the point of care.
Methods
Participants
This study was approved by the University of Virginia Institutional Review Board. Clinicians were recruited from 4 practices affiliated with the Virginia Practice Support and Research Network, which includes University of Virginia academic practices and community-based practices in central Virginia. This study was open to approximately 31 faculty and 24 resident family medicine and internal medicine physicians at 4 different practice-based research network practices. Physicians all had their own PDAs and used the tool in practice for a period of 4 months. Routine smoking cessation counseling and pharmacotherapy for patients was not widely covered by payers at the time of this trial. An electronic medical record was not in use during the study period, although laboratory and imaging results were retrievable via computer.
Study Instruments
A before/after survey instrument was designed and validated to measure self-reported physician behavior, knowledge, and comfort/self-efficacy related to counseling patients about smoking cessation (Appendix 1). The survey also included items on obesity and overweight counseling, which will be reported separately. Content validity was assessed by 6 experts in the fields of behavioral change and smoking cessation. In addition, this instrument was adapted from a similar, previously validated survey in which face and content validity were assessed and the reliability of subscales was measured.17 Because this previous measure showed good reliability for the physician behavior (Cronbach α = 0.74) and physician comfort subscales (Cronbach α = 0.71), the majority of these items were retained. Additional knowledge questions were added to the current survey to address low reliability in the previous survey (Kuder–Richardson formula 20 = 0.23). Demographic variables included hand-held computer literacy, age, and sex.
Use of the Tool at the Point of Care
Use of the tool was monitored via data usage logs that were saved on the device and downloaded to a desktop computer at the end of the study. Activity reports included total sessions, average pages viewed per session, unique pages viewed per session, page contents, date and time of each use, and length of time per use.
Statistics
Self-reported physician behavior, knowledge, and comfort/self-efficacy related to counseling patients about smoking cessation were analyzed for differences from before the intervention to after the intervention. Binary data were analyzed with McNemar χ2 test; all other data were analyzed with Wilcoxon signed rank test. Statistical significance was assumed at α < 0.05. All analyses were conducted with S-Plus 6.1 (Insightful Corp., Seattle, WA) and SPSS version 19 (IBM, Chicago, IL).
Creation of the Clinical Decision Support Tool
A multidisciplinary software development group (SDG) was convened and included a family medicine physician with experience in smoking cessation, 2 general internists with expertise in motivational interviewing (MI) and smoking cessation, and a clinical psychologist with expertise in behavioral change. The SDG adapted the Public Health Service's Clinical Practice Guideline for Treating Tobacco Use and Dependence4 and 3 behavioral health theories—the 5 As,24 Stages of Change (SOC),25 and MI26—into a logical and navigable format. The SDG used an iterative process, meeting weekly for approximately 12 1-hour sessions. The software was designed by the software programmer for both Windows CE and Palm software platforms.18
Description of the MLIT
The SDG developed a theoretical framework integrating the 5 As, SOC, and MI, which we have described previously.27 The “Ask” component of the 5 As was operationalized by encouraging practices to adopt smoking status as a vital sign, but it was not included in the MLIT software. The “Advise” component was integrated into the tool by including information on MI pertinent to physician counseling. The “Assess” and “Assist” components were operationalized using SOC and MI theories. The MLIT uses 2 questions on one screen to guide the identification (assessment) of the patient's current “stage” of change then directs the clinician to “Assist” by providing staged-based information and MI-based scripts promoting smoking cessation (see Figures 1 to 5 in Appendix 2, available online) At the end of the script, MLIT prompts the clinician to “Arrange” follow-up and provides a list of both local and national resources (Figure 6 in Appendix 2, available online).
Results
Twenty-four physicians enrolled in the study (17 faculty and 7 residents), and 17 participants (71%) completed the trial. Before/after surveys were available for all 17 participants (5 residents); however, data usage results were only available for 14 physicians (58%; 4 residents), representing all 4 practice sites. Missing data resulted from hardware failures leading to data loss. Practice locations included 2 large, urban teaching sites (one family medicine teaching clinic with approximately 11 providers, one internal medicine teaching clinic with approximately 13 providers); and 2 rural university-affiliated practices (both family medicine practices, one with 4 physicians and one with 3 physicians). Mean age of the participants was 41 years (range, 28–57 years), and they had spent a mean of 20 years in practice. Of the participants, 71% were men, and 71% reported their hand-held computer literacy as intermediate on a 3-point scale (from novice to expert). Physicians from all 4 separate practices participated in the study. Table 1 contains results discussed in the subscale sections that follow.
Physician Comfort and Self-efficacy With Smoking Cessation Counseling
Physicians reported increased self-efficacy in smoking cessation counseling (before intervention, 4.3 of 7.0 [range, 2–6]; after intervention, 5.0 of 7.0 [range, 4–6]; Wilcoxon signed rank test, P = .006) and increased comfort in following patients once they had initiated a smoking cessation plan (before intervention, 4.9 of 7.0 [range, 2–7]; after intervention, 5.6 of 7.0 [range, 4–7]; P = .04). Reliability of subscales was measured using Cronbach α and found to be 0.70 for the comfort/self-efficacy subscale.
Physician Smoking Cessation Counseling Behavior
Smoking cessation counseling behaviors were measured before and after the intervention using 18 questions (Cronbach α = 0.54). Five questions measured use of the 5 As (ask, advise, assess, assist, and arrange; Cronbach α = 0.64); another 4 questions identified general counseling behavior (Cronbach α = 0.58); and 3 asked about stage-specific interventions, use of motivational interviewing, and use of the Public Health Service guidelines (Cronbach α = −0.170). Finally, 6 questions asked about use of pharmacotherapy (patch, inhaler, nicotine gum, nasal spray, Zyban [GlaxoSmithKline, Research Triangle Park, NC] and Commit lozenges [GlaxoSmithKline]; Cronbach α = 0.56). Performance on the summed 5 As behaviors improved after use of the tool (mean before intervention, 11.0 ± 1.8 [range, 7–15]; mean after intervention, 11.8 ± 1.6 [range 8–14]; P = .03). Improvement was seen in advising smokers to quit smoking (P = .049), and there was a nonsignificant increase in assisting smokers with quitting (P = .09). General counseling behaviors did not change after use of the tool (eg, How often do you counsel? How often do you provide smoking cessation information? How often do you use smoking cessation pharmacotherapy? How often do you refer smokers for counseling?). More physicians used stage-specific interventions, MI, and the Public Health Service guidelines after use of the tool, but these changes were not statistically significant. There were no significant changes in pharmacotherapy use; however, an increase in the use of Commit lozenges after use of the tool was observed (P= .07).
Physician Knowledge About Smoking Cessation
Overall smoking cessation knowledge was unchanged (before intervention, 75.2 ± 12.7% correct; after intervention, 76.9 ± 10.9% correct; P= NS). When the subscales for stage-based classification and interventions were examined (Cronbach α = 0.65), we found no statistically significant increase in knowledge. However, there was an increase in smoking cessation pharmacotherapy knowledge (before intervention, 50 ± 19.8% correct; after intervention, 64.7 ± 23.5% correct; P = .053; Cronbach α = 0.04).
Physician Use of Tool at Point of Care
Clinicians who completed the study and had valid use data (n = 14) had a total of 71 sessions (average of 5 sessions per user). The majority of physicians used the tool during clinic hours (93%), and the average session lasted 21 minutes. Additional data on tool use and content accessed are detailed in Tables 2 and 3.
Discussion
We created a novel clinical decision support tool to assist clinicians with smoking cessation counseling. Use of this tool was associated with increased use of the 5 As well as increased physician self-efficacy and comfort in providing smoking cessation counseling.
The MLIT tool integrated 3 theoretical frameworks. The 5 As provides a broad framework for behavioral counseling and its adoption is recommended by the U.S. Preventive Services Task Force. Physicians can vary the intensity and complexity of the behavior change counseling, matching their efforts to factors individual to each patient. The framework is simple to understand, adaptable to most behavioral health risks, and provides a consistent approach with demonstrated efficacy.4,24 The SOC model has been shown to be an effective approach to smoking cessation counseling.25 This model tailors the counseling to the individual patient's readiness to change, making the process less confrontational and more efficient. The fundamental postulate of SOC is that effective behavioral change is best facilitated by sequentially moving individuals from one stage to the next using stage-matched intervention strategies. Although we recognize the potential limitations of SOC to predict individual behavior,28⇓–30 it is a model with which many physicians are familiar and is an important reminder to consider a patient's readiness for any particular message or intervention.31,32 Although the principles of SOC were used to conceptualize and assess patients' readiness for change, MI techniques formed the basis of the scripted interviews used by physicians to move patients along the SOC continuum. MI promotes relationship building and attempts to motivate patients by exploring and resolving their ambivalence about changing their behavior. Strong evidence supports the use of this approach for effective smoking cessation counseling in primary care settings,33 and there is significant literature supporting its use for other health behaviors.34,35 To our knowledge, our study is the first formal integration of the SOC, MI, and the 5 As approaches into a singular clinical decision support tool for use by physicians at the point of care.
Comparison With Prior Work
Physicians report lack of training, skill, and time as barriers to being effective behavioral counselors.19⇓⇓⇓–23 Simple clinical decision support tools available for use at the point of care can potentially overcome these barriers and may also serve as an educational tool. Our study demonstrates that even short-term exposure (4 months) to a clinical decision support tool can improve physicians' confidence and self-efficacy in smoking cessation counseling and can change physician counseling behaviors. There also is emerging evidence that hand-held computers may be an effective modality for improving patient outcomes in office-based settings. Studies of hand-held computers in these settings have shown improved treatment by physicians for asthma,36 otitis media37 and upper respiratory infections.38 Another study showed potential reductions in adverse drug events.39
Limitations
We studied a small sample of physicians, the majority of whom rated their hand-held computer literacy as intermediate. Physicians also needed to own a PDA to participate. Because of the small sample size and purposeful sampling, external generalizability is not assured, and larger trials in various medical settings should be conducted. In addition, because of the high level of computer literacy, study participants may have been more willing to use a clinical decision support tool because of their previous experience in using hand-held technology. This should also be replicated in groups that have varying levels of computer literacy. However, increasing use of electronic medical records by all physicians and smartphones by the newest generation of physicians will likely diminish this limitation over time. Our use of before/after study design is a further limitation because it cannot control for secular trends, test/retest performance, and other potential confounders inherent in this design. We did not find an overall improvement in knowledge scores among users of the MLIT. This may represent a ceiling effect in this group of physicians; many of them were already knowledgeable regarding smoking cessation counseling, the Public Health Service guidelines, and pharmacological treatment options before their use of the tool. In addition, changes in physician behavior were based on self-report and, because of the limited scope of this study, no measures of clinical outcomes were obtained. Last, some of the scales used to measure differences in physician comfort, behaviors, and knowledge did not have high internal reliability and would benefit from further psychometric analysis and development before being deployed in larger trials.
Lessons Learned and Next Steps
This new tool was accepted by physicians and used in clinical practice. In addition, use by a large number of residents and length of time of each use indicate potential as an educational intervention. Since there is increasing interest in and evidence for using this approach with other health care providers in patient-centered medical homes, we propose to test this approach with nurses, nurse practitioners, physician assistants, and other members of the health care team, as well as in residency education. Our institutional and practice environment has shifted toward the use of a full-featured electronic medical record, and therefore the use of this tool on PDAs and smartphones has become less relevant; however, the content is ideal for use with electronic medical records. To continue quick versioning the software content and applying it to other behavior changes, we have found it necessary to partner with a software development company with expertise and capacity to support rapidly evolving clinical and technical demands. We currently are developing and testing tools for use in alcohol misuse, drug abuse, and obesity. We aim to develop a full-featured behavior change platform that can be used with nearly any hardware (eg, desktop personal computers, tablet computers, smartphones, and PDAs).
Conclusions
Hand-held computers can provide portable clinical decision support at the point of contact between patients and clinicians and may be useful as educational tools. They are widely available, relatively inexpensive, and easy to access and operate. In addition, clinicians report using them for professional use in high numbers (45% to 85%, depending on the setting).40 Our study demonstrates that these tools can improve physician confidence and self-efficacy in smoking cessation counseling. Larger controlled trials in community-based and educational settings are needed to determine whether such tools can increase clinician knowledge and ultimately affect patient outcomes. If these results are confirmed, there seems to be a significant opportunity to enhance the translation of guidelines into clinical practice through this approach, ultimately benefiting patients by helping physicians address important unhealthy behaviors such as smoking.
Appendix A: Before/After Survey Measuring Physician Behavior, Attitudes, Comfort, and Knowledge About Smoking Cessation Counseling
Appendix B: Content Screens From Modular Lifestyle Intervention Tool (MLIT) Tool

Stage of change tool in MLIT used to guide clinician to appropriate stage-based intervention.

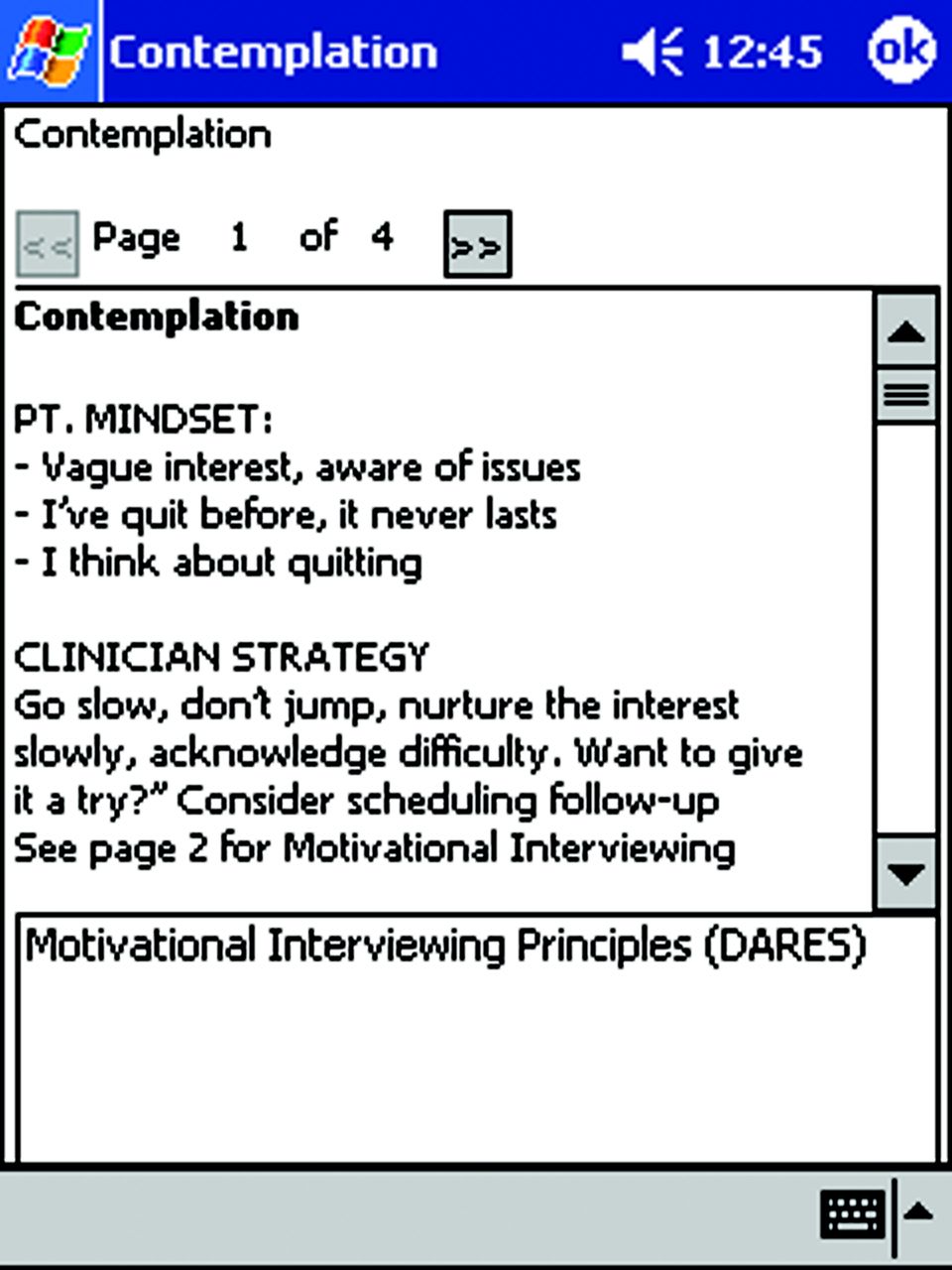
Initial “contemplation” content screen.
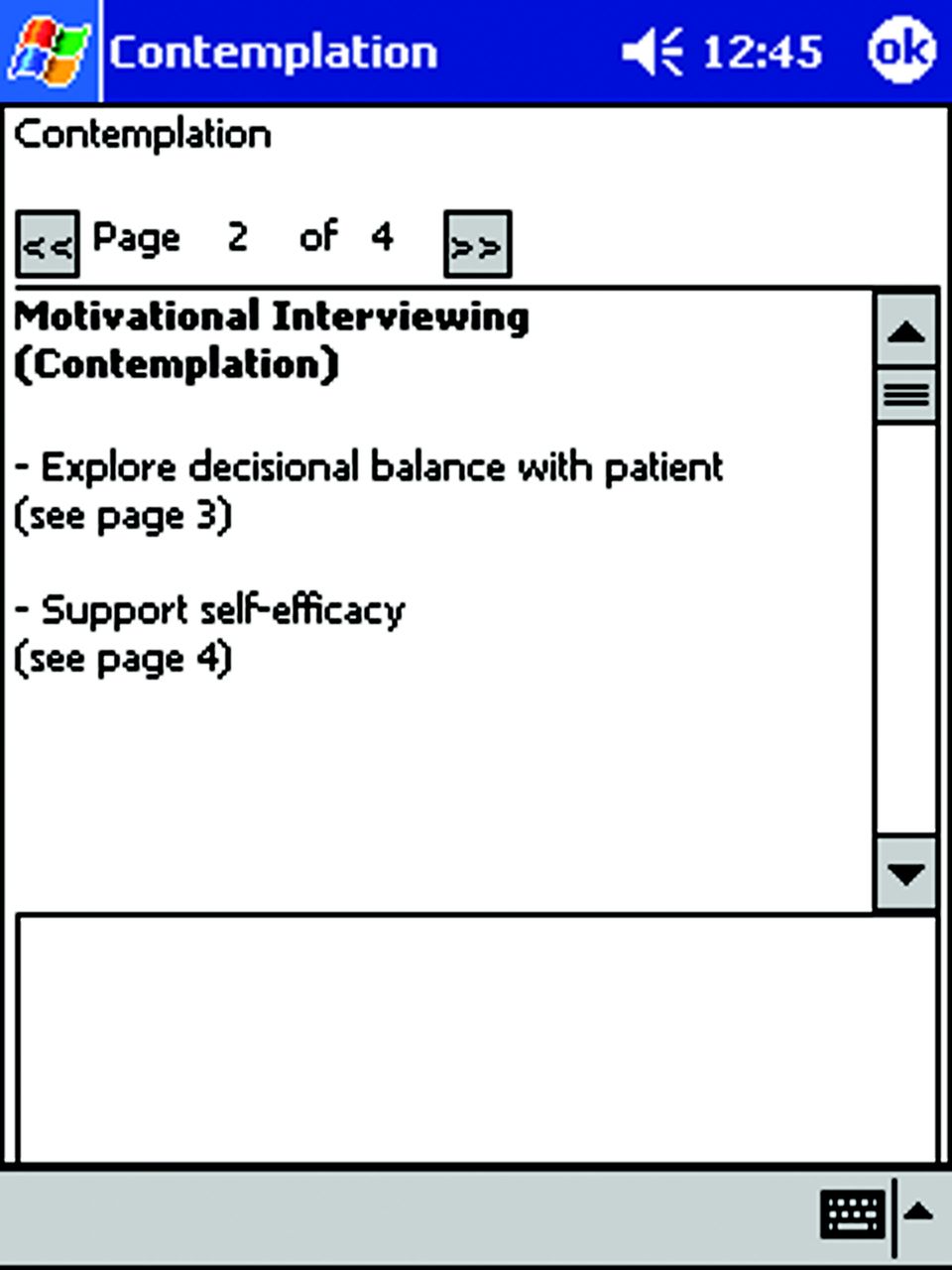
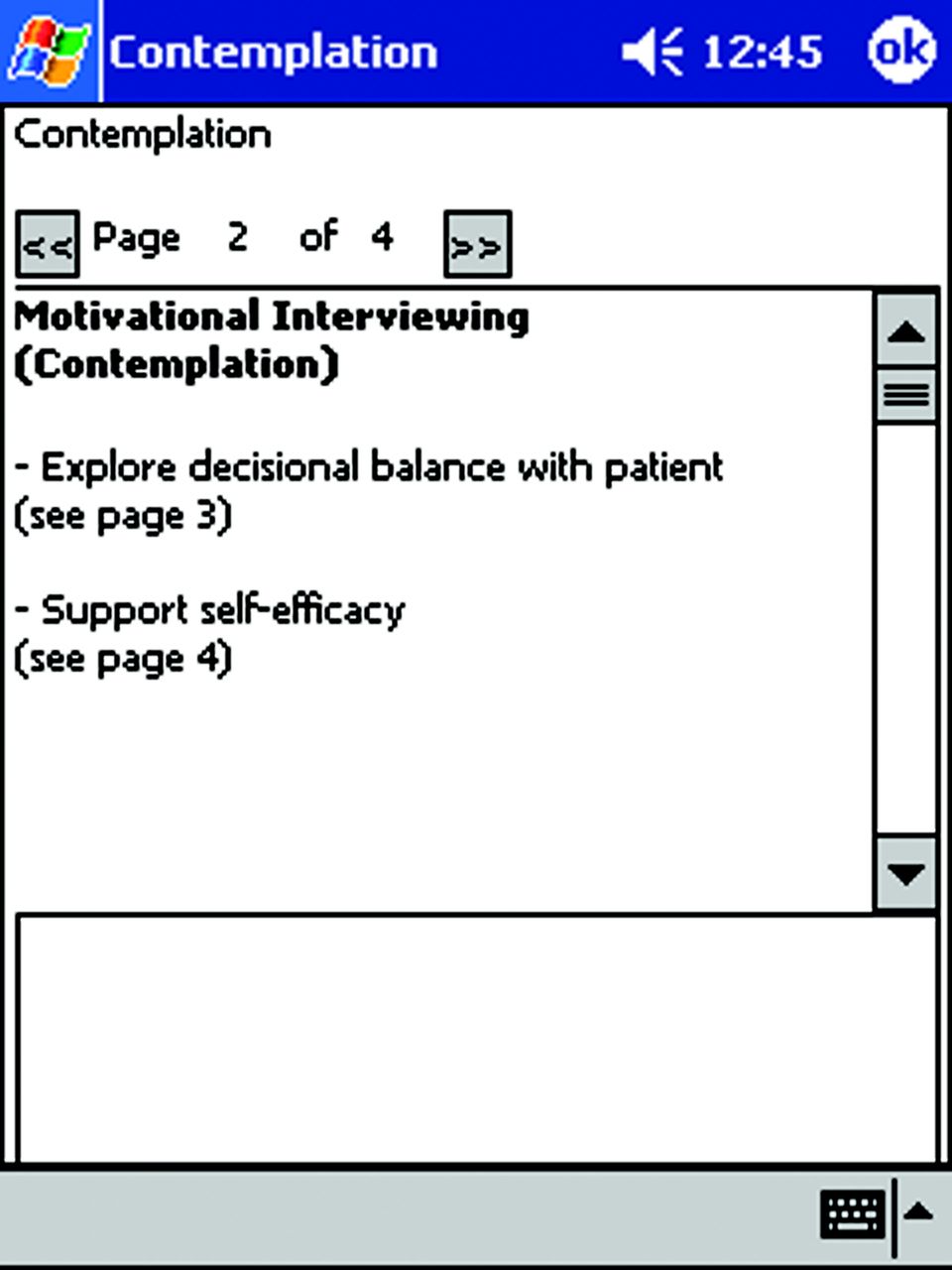
Appropriate stage-based interventions for clinicians to use with patients in contemplation stage.
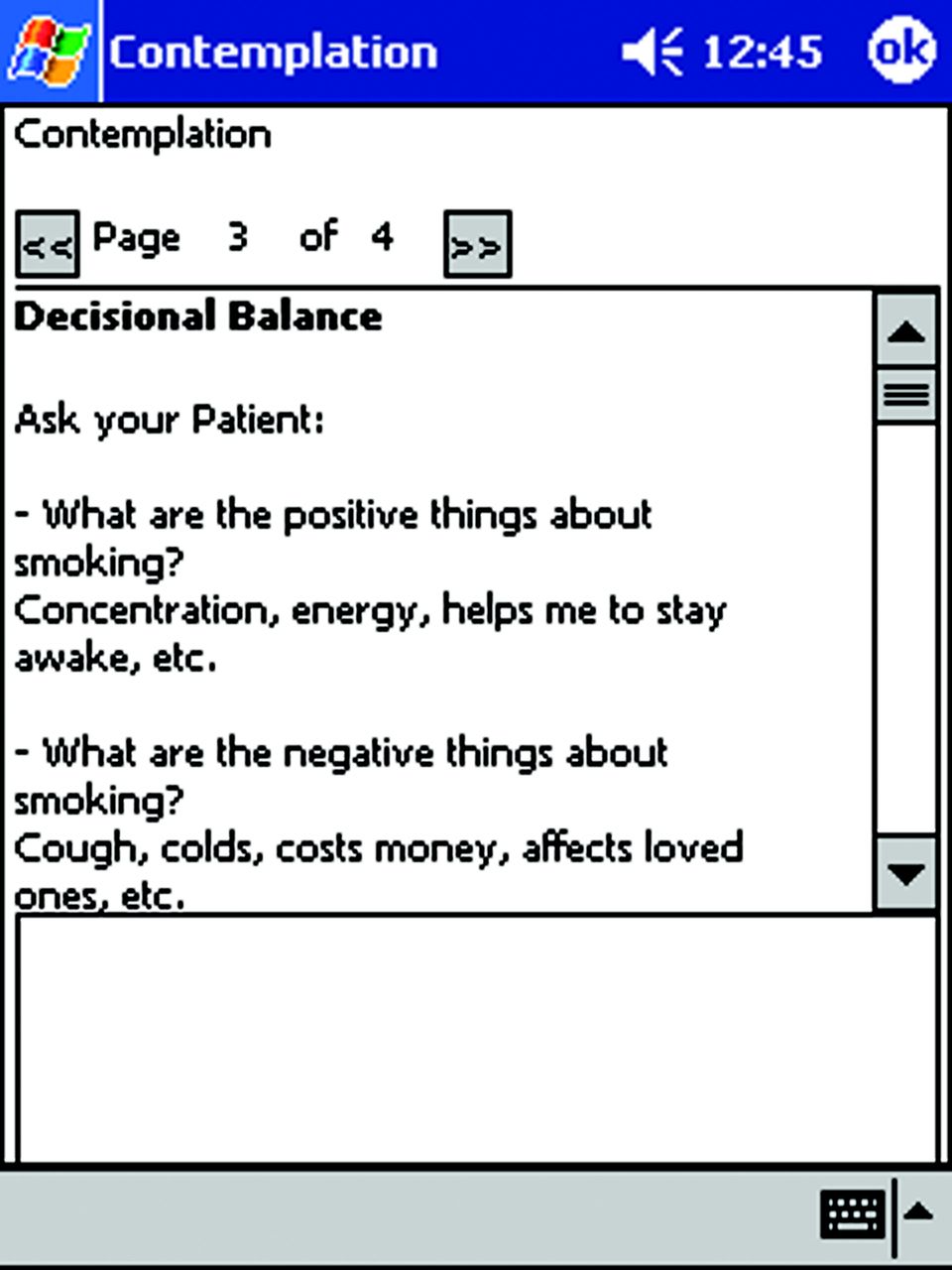
Physician prompts for addressing “decisional balance” with patient in contemplation stage.
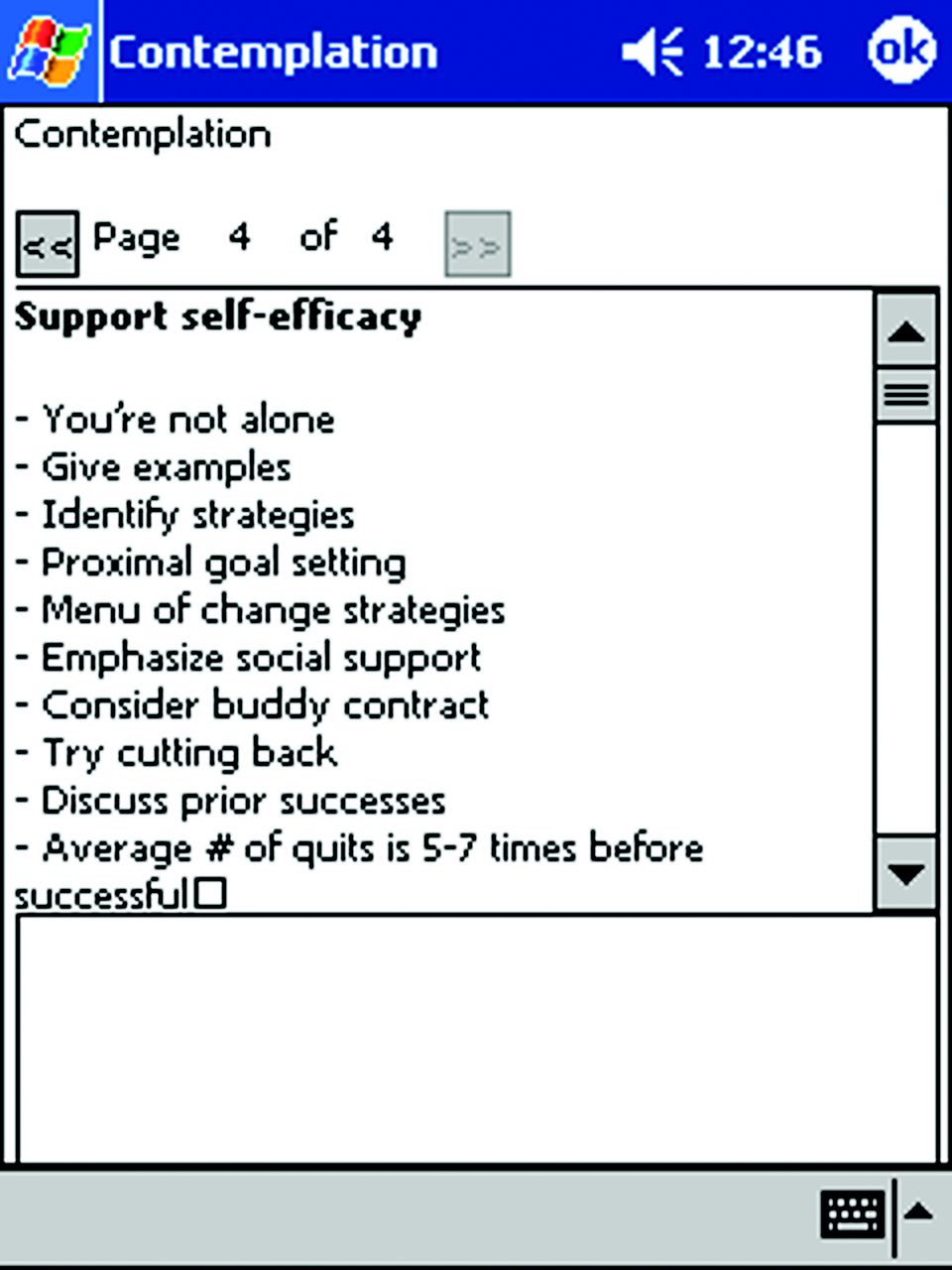
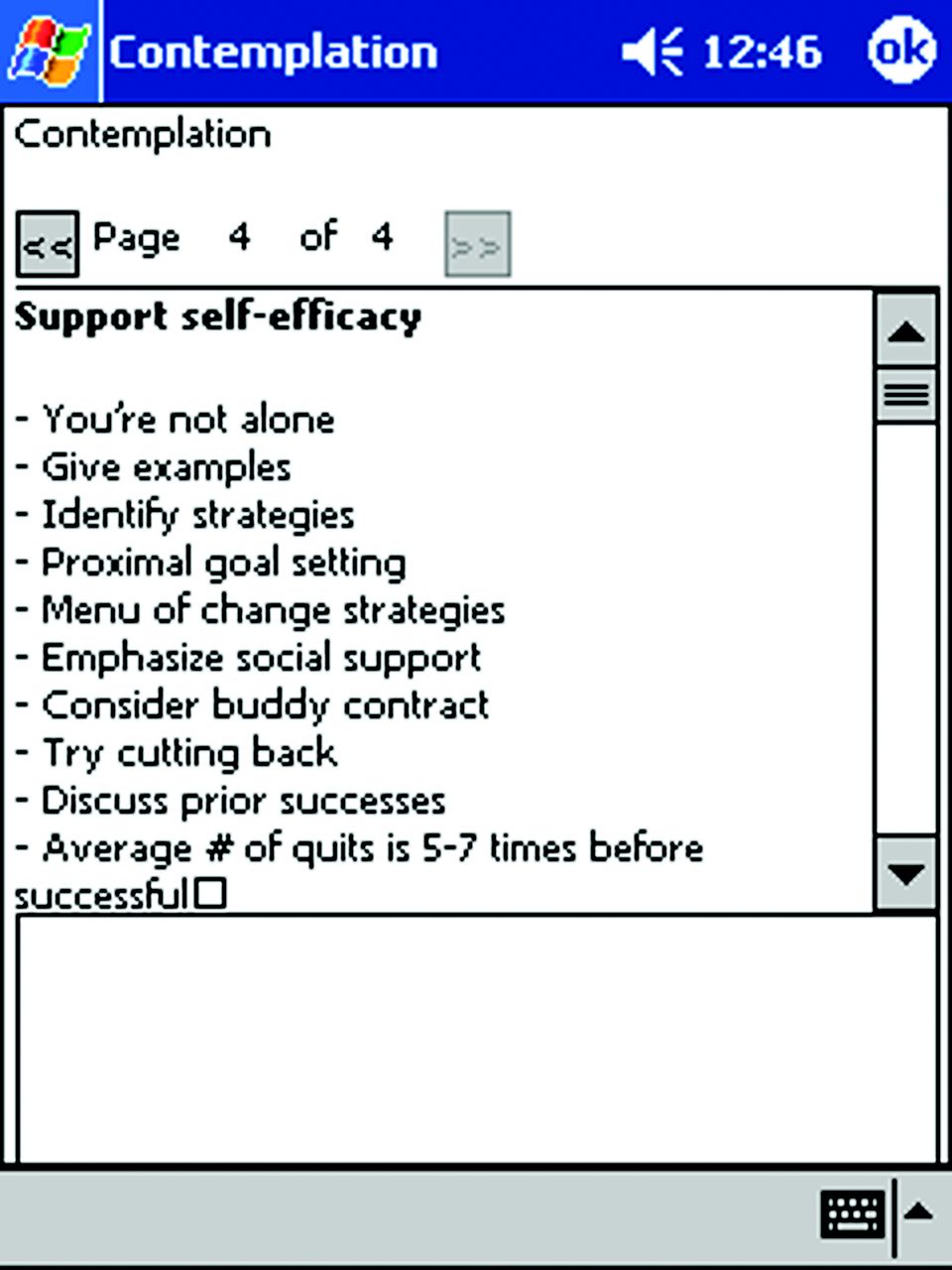
Physician prompts for “supporting self-efficacy” of patients.
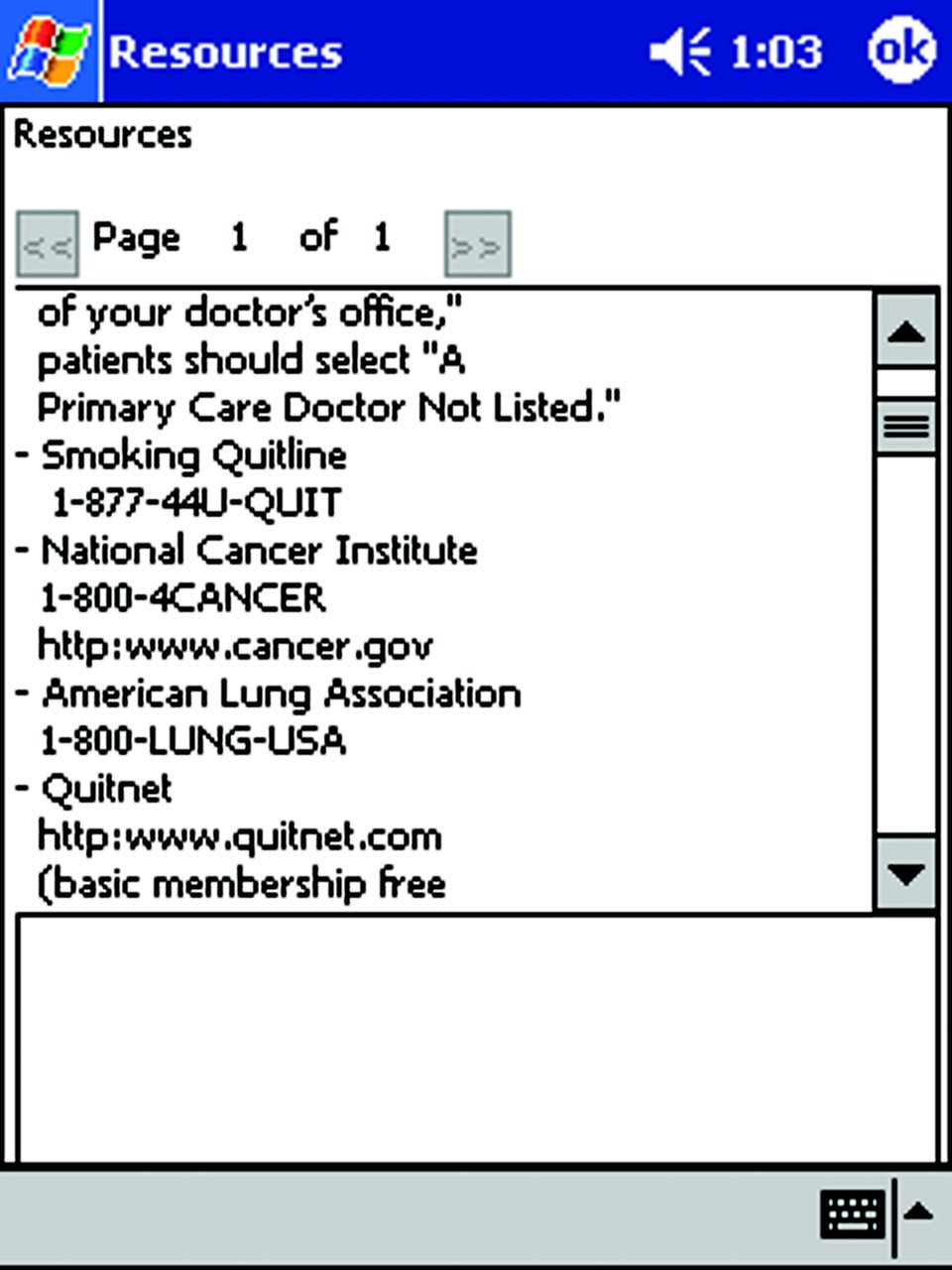
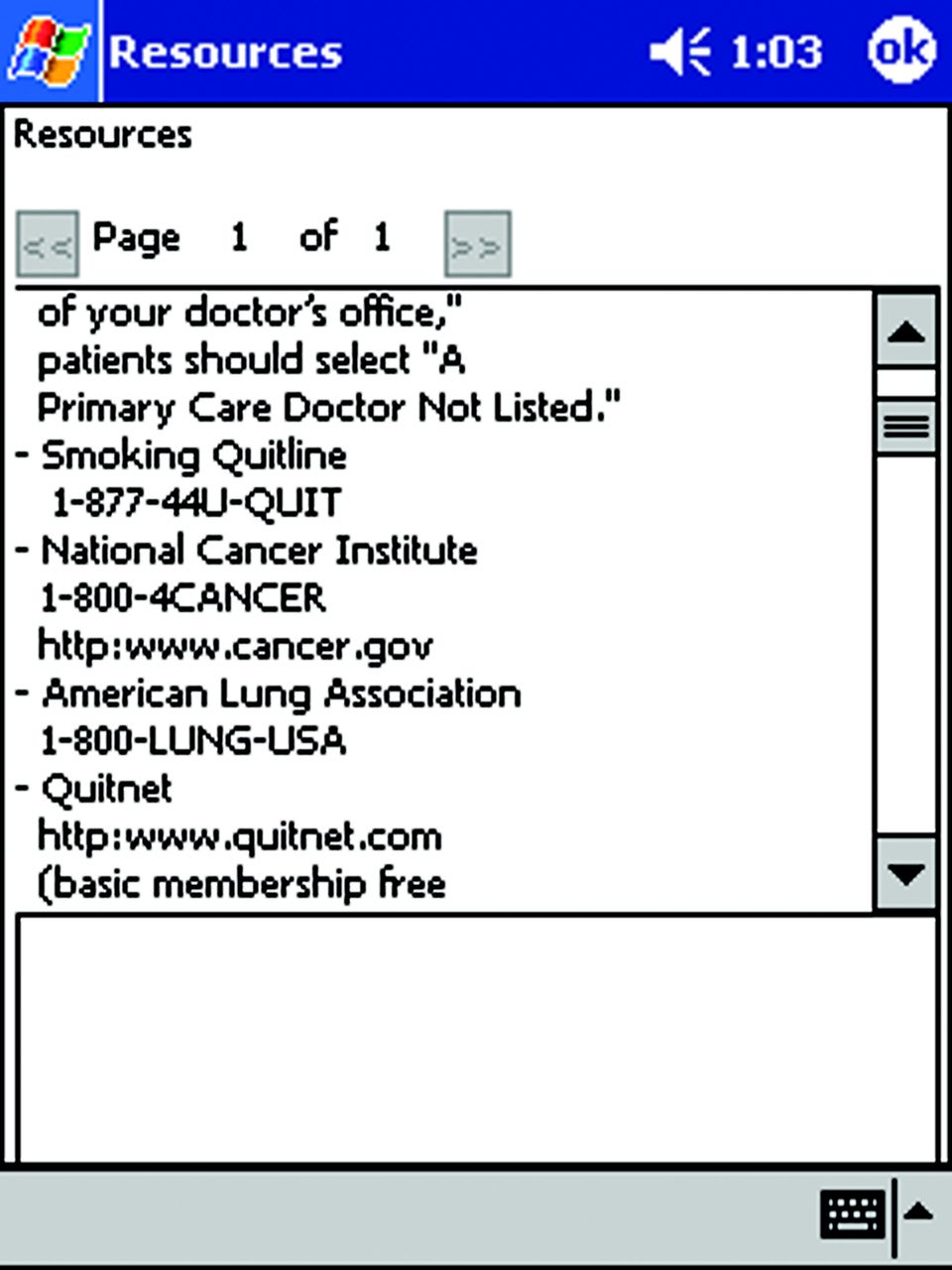
National and local resources listed to prompt physicians to arrange follow-up with patients.
Notes
This article was externally peer reviewed.
Funding: Support has been provided by Prescription for Health, Robert Wood Johnson Foundation, ID no. 049056, and a Health Resources and Services Administration Academic Administrative Units in Primary Care–Family Medicine Grant (no. D12HP00148).
Conflict of interest: none declared.
- Received for publication November 1, 2012.
- Revision received November 1, 2012.
- Accepted for publication November 1, 2012.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}