
Abstract
We describe how collaboration with outpatient community health centers and other disciplines resulted in the creation of a novel interdisciplinary inpatient maternal child health system that focuses on safety and collaboration. Our maternal child health faculty team includes a mix of fellowship- and non–fellowship-trained, inpatient- and outpatient-based family physicians. Our team provides a sustainable framework for faculty to practice both inpatient and outpatient maternity care and provides strong role models for our trainees.
- Collaboration
- Delivery of Health Care
- Education
- Patient Care Team
- Perinatal Care
- Quality of Health Care
- Safety
Maternity care is a core attribute in family medicine. However, during the last several decades, there has been a steady decline in the percentage of family physicians providing labor and delivery care in the United States, with 46% of family physicians providing this care in 1978 compared with 18% in 2009.1⇓⇓–4 Many family physicians do not include intrapartum care in their practices for a variety of reasons, including malpractice costs, lifestyle implications, inadequate training, and lack of sufficient backup services.5⇓⇓–8 The Future of Family Medicine Project lists maternity care in the “basket of services” that should be provided in the New Model of Family Medicine but recognizes that the extent to which family physicians provide this care may vary.9 Ten different modes of maternity care practice in the United States recently have been defined. In response to this, a tiered approach to maternity care training in family medicine has been proposed. This approach addresses limitations in residency program resources and permits residents to individualize their training in maternity care.10
As family medicine training programs adapt to the realities of the provision of maternity care services, it is essential that some programs continue to offer opportunities for rigorous training in maternity care, including intrapartum services. Maternity care results in a younger patient population in family medicine practices and ensures that we continue to care for families and patients throughout the life cycle.11,12 These practice characteristics, in addition to broad training that includes rigorous inpatient and hands-on procedural experience during residency, correlate with early career satisfaction in family medicine.13 From a public health standpoint, family physicians are the only physicians who provide maternity services in certain communities, and a decline in the number of family physicians providing these services will severely limit access to care, especially for those in rural or underserved populations.14⇓⇓–17 Last, our specialty's focus on continuous relationships, orientation to the whole person and community, as well as our commitment to patient-centered medical homes can contribute to a field that traditionally has been led by obstetricians who are surgically trained with a focus on disease and pathology.18⇓–20
We have described the rationale for a new model of care on our labor and delivery unit and its impact on intrapartum providers.21 The model has changed family physician's role from being an extraneous provider of maternal and newborn services to one that is integral to daily operations of our hospital and community health center (CHC) network. Our labor and delivery model offers a safer system for patients, sufficient volume for family medicine faculty to maintain skills, colleagues invested in their growth as clinicians, and adequate experience and educational excellence for our trainees. After the establishment of our role in the labor and delivery unit, our interdisciplinary collaboration extended to a reorganization of postpartum services. We worked with obstetricians, midwives, and pediatricians to create a family medicine postpartum inpatient service. We are now working on improving collaboration and communication between the hospital and our CHC network.
Our History
Boston University School of Medicine is based at Boston Medical Center, the largest safety net hospital in New England. We serve an ethnically diverse population, and the majority of labor and delivery patients (81%) are insured by government-sponsored health insurance. Family medicine faculty and residents provide care for patients at 6 of 16 CHCs associated with the hospital. Our department started in 1997 with 6 faculty, the majority of whom provided intrapartum maternity care. The chair of family medicine approves core labor and delivery privileges; operative and advanced labor and delivery privileges are credentialed jointly with the chair of obstetrics and gynecology.
Three disciplines provided intrapartum care at our hospital: obstetricians, midwives, and family physicians. The 3 services worked alongside one another with minimal communication unless there was a need for formal consultation or transfer to the obstetrician on call. Respectful communication and trust among providers across disciplines was neither consistent nor expected. There was a range of skills among the family medicine faculty depending on training and clinical experience. Some faculty were new graduates, others were faculty who had delivered in high-volume settings before joining the department, and 2 completed a fellowship in obstetrics and were skilled in the care of high-risk patients and operative deliveries. However, there was not adequate opportunity for collaboration and support between maternity care providers either within our own department or with the other services. Guidelines for consultation between family physicians and obstetricians were not defined and the culture did not encourage early consultation.
Family medicine faculty provided 24/7 coverage for our patients and came to the hospital when our patients required an attending's presence. Because our volume was low and our presence in house was required infrequently, faculty members generally had competing clinical or administrative duties while on call and after a call. Some providers delivered their own prenatal patients regardless of whether they were on call. Some family medicine faculty performed fewer than 7 deliveries a year, a number that has been shown to be associated with an increased rate of complications.22 Our newborn census was even lower than our maternal census because a portion of our patients chose pediatricians for their children despite being followed themselves by a family physician. Given these circumstances, by the early 2000s we recognized the need to change our system to preserve the delivery of safe maternal and newborn services by our faculty.
Since its beginning, our department partnered with CHCs, placing our model residency and faculty practices at 2 CHCs. In 2003, we expanded to include one of the largest CHCs in the country and doubled the number of family medicine prenatal patients from approximately 100 to 200 patients. In January 2005, this same CHC chose to move all its obstetric deliveries to our hospital, increasing the number of deliveries by 400 annually. Although there was a backup obstetrician available overnight, this person had clinical responsibilities the next day so mobilizing this resource on a regular basis was not an option for helping to manage the increased volume. The hospital recognized that a new system of care would need to be established to safely handle this increased volume.
Designing a System
The Departments of Obstetrics and Family Medicine envisioned the creation of a team of providers working in labor and delivery continuously, each with distinct yet valuable expertise in patient care. To emphasize teamwork and remove financial disincentives to collaboration, the department chairs merged the billing for the care of all patients under a single entity that reimburses each department for attending time spent in labor and delivery. Hospital leadership agreed to support this model financially because of anticipated benefits to patient safety and to protect both departments from financial loss. This was facilitated because the hospital recently had begun to self-insure its physicians and agreed that the added emphasis on safety should translate into decreased malpractice expenses and more than offset the additional cost. The departments and hospital leadership made the decision to initiate the new model and require the continuous in-house presence of a family medicine physician starting in January 2006.
Preparing Family Medicine Faculty
In preparation for its increased presence in the labor and delivery unit, the Department of Family Medicine realized that it needed to create a strong group of faculty committed to maternity care. We initiated regular meetings that allowed the faculty to work together toward the common goal of becoming a group of physicians excellent at maternity and newborn care. During these meetings, we provided support for each other, discussed educational or clinical issues, and tackled any issues that hindered the successful operations of our team.
We wanted to design a team that could staff these hours without causing burnout in our faculty since increased workload and less flexibility are reasons that physicians stop delivering intrapartum care.23 We did this by recruiting 3 additional fellowship-trained faculty, thereby anchoring our maternity team with a total of 5 fellowship-trained family physicians. They staff a larger proportion of our labor and delivery time, specifically during weekdays when more scheduled surgical events occur. Some of these fellowship-trained physicians are maternity care “hospitalists,” whereas others continue to practice full scope family medicine. Our non–fellowship-trained physicians participate in the in-house coverage but with fewer shifts and a weekly schedule that is more focused on their outpatient practices.
Our collaboration with obstetricians and midwives in labor and delivery helps all family medicine faculty keep up to date on clinical guidelines. Faculty who practice intrapartum care act as a resource for those who provide outpatient maternity care services only. We wanted to bolster the knowledge and skills of our faculty that had waned in the preceding years and asked faculty to provide a self-assessment of their obstetric skills and knowledge. The self-assessment showed that faculty felt uncomfortable with some of their skills; therefore, we planned a series of faculty seminars to review clinical topics and increase hands-on skills. During this time of transition, a few of our faculty members chose to stop providing intrapartum maternity care and focus on other areas of their family medicine practice. We determined that 14 to 16 was the optimal number of family medicine faculty to staff the service and that all must engage in at least twenty 12-hour shifts in the labor and delivery unit annually to maintain competency.
Building a Multidisciplinary Team
The continuous in-house presence of the family medicine faculty challenged us to re-evaluate our role in labor and delivery. A multidisciplinary leadership group made up of family physicians, obstetricians, midwives, nurses, and residents met weekly to define a new model of collaborative team care in labor and delivery (Table 1). During the first year, our presence improved the work flow of the unit, specifically in the care of triage patients (all patients at more than 16 weeks' gestation presenting to the hospital are sent to a triage unit that is geographically contiguous with the labor and delivery suite), postpartum patients, and the performance of circumcisions. However, family physicians were still less involved in attending deliveries compared with the obstetricians and midwives because our prenatal population remained stable, only contributing less than 10% of hospital deliveries. Mistrust of family physicians persisted and some of our faculty spent a good portion of their in-house hours in the call room.
The multidisciplinary leadership group introduced an innovative proposal in July 2007 regarding the distribution of laboring patients between the 3 services. Continuity generally was preserved, with preference given to keeping midwife patients with the midwifery service and family medicine patients with the family medicine service. However, most patients who were followed prenatally by an obstetrician did not require a provider with advanced obstetrical or surgical skills. These patients primarily were assigned to the family medicine service, with careful consideration of individual needs such as language or patient preference. As a safety issue, attention also was given to the number of patients on each service, and we followed a principle of balancing workload between each of the 3 disciplines. This algorithm for distribution of patients increased the volume of deliveries for the family physicians over time (Figure 1). The increase in delivery volume reflected an increase in both vaginal and Cesarean deliveries, providing our faculty with sufficient clinical opportunities to practice and refine their skills, to work more frequently with residents and nursing staff, and to show competence that was not always apparent because of our previous low volume. Slowly but steadily, familiarity with our faculty changed the culture of our labor and delivery unit and broke down barriers related to mistrust and poor communication. Our colleagues in midwifery and obstetrics delivered fewer patients in the new model of care, but with the merged billings, there was no decrease in compensation for our colleagues at either the individual or department levels. For family medicine, our obstetrics services became a part of the merged billings, but we retained hospital financial support to break even on salary support for our in-house labor and delivery family medicine provider. Of note, faculty in both departments are supportive of a culture that strongly encourages sharing the workload without a financial incentive. This structure was integral to promoting patient centeredness and safety as the true priorities. Our model minimizes situations when a single provider carries an overwhelming clinical load, thereby creating opportunities for safer, more fulfilling patient interactions. Midwives had more time to be at the bedside and focus on socially at-risk patients such as teenagers or those who were socially isolated. Obstetricians were able to devote more time to medical or surgical high-risk patients.
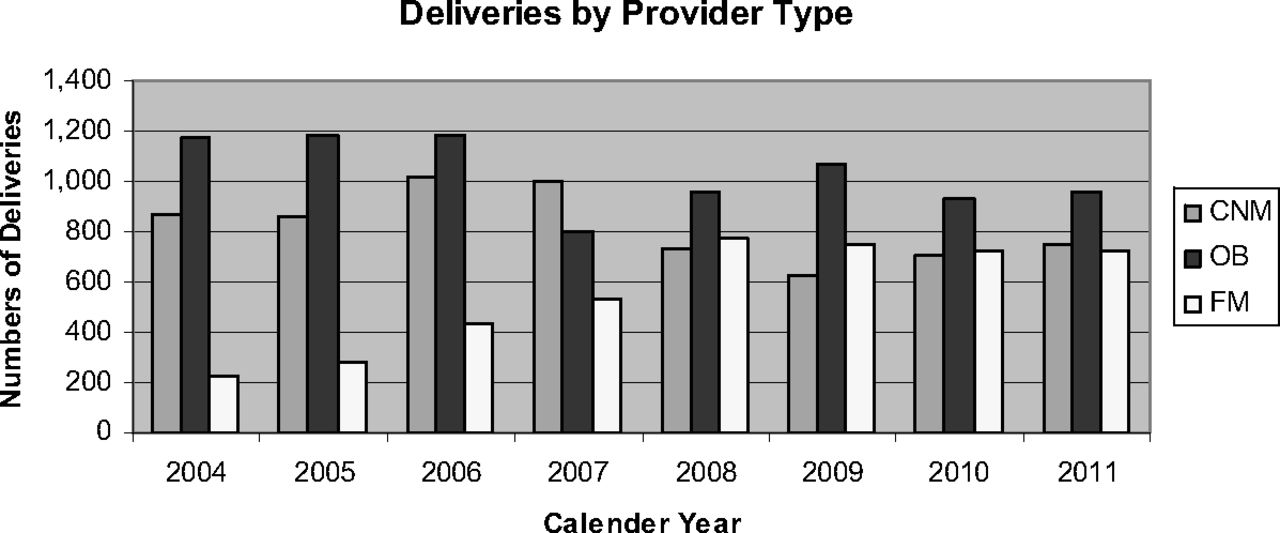
Annual change in distribution of deliveries by provider group. CNM, certified nurse midwife; FM, family medicine; OB, obstetrics.
The Department of Pediatrics requested that we develop a similar collaboration with its faculty and nurse practitioner staff to assist with the workload issues in the newborn nursery resulting from these additional 400 deliveries. We established a new system of care to admit approximately one third of all newborns and their mothers to a newly created family medicine maternal-child inpatient service. With this system, the hospital was able to accommodate the increased number of deliveries and was able to accommodate the request for newborn hospitalist services by our health center pediatricians.
The success of our interdisciplinary collaborative relationships has been dependent on creating a culture that encourages communication. Leaders from family medicine, midwifery, obstetrics, and nursing trained to teach teamwork concepts to all individuals who work in the labor and delivery unit. We start the day in labor and delivery with an interdisciplinary meeting that includes family physicians, midwives, obstetricians, and family medicine and obstetrics residents. Likewise, we start the day in the maternity ward with a meeting that includes family physicians, pediatricians, and family medicine and pediatric residents. During these meetings, we review all patients, discuss plans of care, teach, and learn together. We also use this time to ensure appropriate distribution of workload between the different disciplines. Team-based care is emphasized and our interdisciplinary team capitalizes on the strengths of each member so that the patient is offered a team of care providers rather than separate, uncoordinated services.
Another guiding principle of our collaborative system is that all disciplines have agreed to practice according to standard clinical guidelines. These guidelines ensure the practice of evidenced-based care and were developed as a natural progression of mutual respect for the value that each group brings to clinical care. There has been minimal resistance to their adoption because all stakeholders have an opportunity to contribute to the process. Furthermore, increased communication and consultation between disciplines is occurring between the ambulatory and labor and delivery staff, between labor and delivery and postpartum/newborn staff, and within each health center, resulting in the adoption of patient-centered, evidence-based practices for our patients.
Impact on Resident Education
Redefining the role of family medicine faculty in labor and delivery has improved education for both obstetrics and family medicine residents. The Department of Family Medicine's leadership made a specific decision to improve faculty skills and refine the new relationships with the Departments of Obstetrics and Gynecology and Pediatrics before redesigning our residency experiences. Our attendings supervise residents from both departments in all activities including circumcisions, triage visits, and vaginal and abdominal deliveries. Rather than highlighting a differential of knowledge and skills between interns of different disciplines, our current model encourages teamwork and the sharing of knowledge between residents of the 2 disciplines, mirroring the teamwork at the attending level.
In 2008, we launched a complete revision of our 3-year maternity curriculum. Whereas we previously staffed the labor and delivery unit with family medicine interns only during rotations when the obstetrics residents were unable to cover the unit, a family medicine intern or resident now works alongside obstetric residents weekdays and weeknights and participates in the weekend call pool as the solo on-call intern or resident throughout the year. Our residents now have earlier exposure to labor and delivery care and perform more than 40 deliveries each during their first year. This has allowed those who plan on practicing obstetrics after graduation to have the opportunity to gain additional experience during the remainder of their residency.
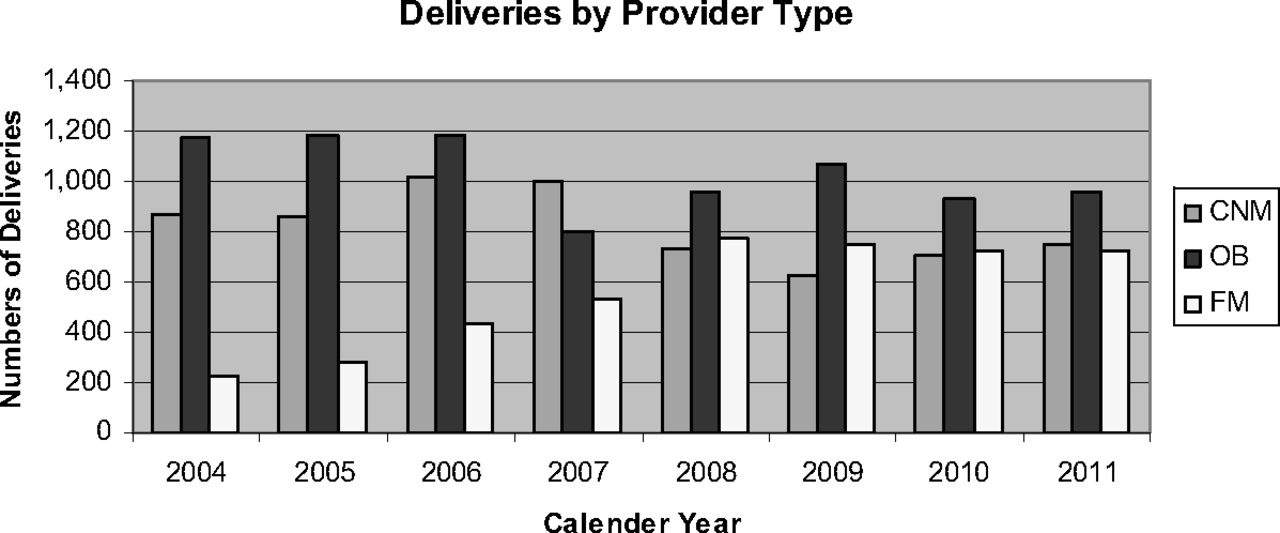
Midwives perform all their deliveries with obstetrics, family medicine, or midwife trainees in this new collaborative model of care. The addition of approximately 800 midwifery deliveries to the pool for resident education was evident in the increased number of deliveries performed by our residents (Figure 2). Previously, midwife patients were seen and delivered by only midwives or midwife students unless there was a specific indication for consultation or transfer of care to an obstetrician. Although midwives valued delivering their patients without the involvement of residents, this system created barriers between the midwifery and physician services and did not encourage early consultation. The opportunity to teach interns and residents a midwifery model of care, as well as the benefit to patient safety, ultimately inspired the midwifery group to collaborate with enthusiasm. In 2010, the family medicine residents recognized one of the midwives with the “Out-of-Department Teacher of the Year Award.”

Total residency deliveries per academic year.
Our maternal-child inpatient service has increased our visibility with the pediatrics and family medicine residents in this clinical area. Newborns are attended by either pediatricians or family physicians and our increased volume has provided us greater opportunities to interact and teach.
Discussion
Our new model of maternity care provides an approach that has resulted in apparent reductions of maternity-related hospital and professional malpractice claims and costs24 without decreasing patient satisfaction. It has improved the educational environment, supports the maintenance of faculty competencies, and provides trainees with a sustainable model of family physician participation in maternity care in an urban environment. It has improved the culture of care with a shift toward evidence-based care, true interdisciplinary collaboration, timely communication, and continuing reassessment and improvement involving all labor and delivery, postpartum, and newborn nursery professional groups. Thus far, we have not seen a significant change in outcomes such as the rate of Cesarean delivery, rates of vaginal birth after Cesarean delivery, and the number of infants with low Apgar scores, low birth weight, or that require admission to the neonatal intensive care unit. We monitor these outcomes on a quarterly basis, and though there is stability in these measures, the reduction in malpractice claims is, in fact, an important outcome and may imply increased patient satisfaction with care.
We have created an innovative structure through the process of developing a strong team of faculty in our department that is engaged in maternity and newborn care and teaching. This strays far from the cherished concept of a family physician practicing the full scope family medicine, delivering their own patients and caring for their own patients in the hospital. Though continuity is satisfying for both the physician and patient,25 and may be important to some women,26 a wider review of the literature suggests that women can be satisfied with the delivery experience even if they do not know their delivering provider. Other factors during delivery, including communication and shared decision making, contribute to patient satisfaction.27,28 Although not specifically targeted at assessing our team-based care, Press Ganey patient satisfaction surveys responded to by our maternity patients have increased from a score of 80 in 2004 to a score of 85 in 2010.21
At our institution, there are few patients who are delivered by their prenatal care provider. For this reason, our trend regarding patient satisfaction may not be generalizable to other hospital systems or family medicine practices where delivery by a specific provider or small group of providers is expected. In the absence of a woman's prenatal care provider, our model offers a safe, patient-centered method for selecting an appropriate provider and offers care that is characterized by frequent communication between the labor and delivery team and the patient herself.
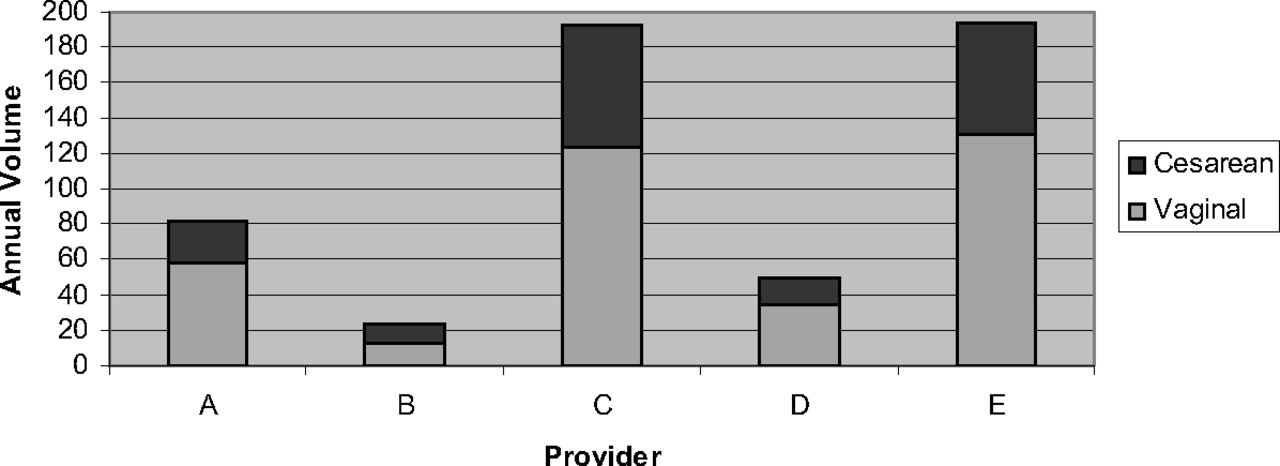
We previously were unable to provide an adequate labor and delivery experience for our family medicine faculty. Fortunately, in our case, the recognition and response to waning faculty skills was precipitated by an opportunity to increase the number of women receiving care at our hospital rather than as a result of an adverse intrapartum event. Whereas new graduates may need robust volume to grow clinically, experienced faculty can maintain their skills with fewer deliveries. Fellowship-trained faculty generally feel comfortable with high-risk medical or surgical procedures29 and, in fact, may apply for board certification in operative obstetrics.30 These faculty need an adequate volume of high-risk or operative procedures to continue to grow and maintain their advanced skills. Our current volume ensures adequate volume for non–fellowship-trained faculty, with 2 to 3 shifts a month and an average of 0.8 deliveries per shift (Figure 3). As seen in Figure 4, provider B did not achieve a minimum of 20 shifts because of an extended maternity leave. Fellowship-trained faculty have a mix of vaginal and Cesarean deliveries at a volume that more than maintains their operative skills (Figure 4). Their average number of deliveries is 1.1 per shift because they are able to attend both delivery modes. Our in-house model allows faculty to focus solely on maternity care, avoiding the need to juggle multiple commitments and distractions that may impact patient care or faculty enrichment.
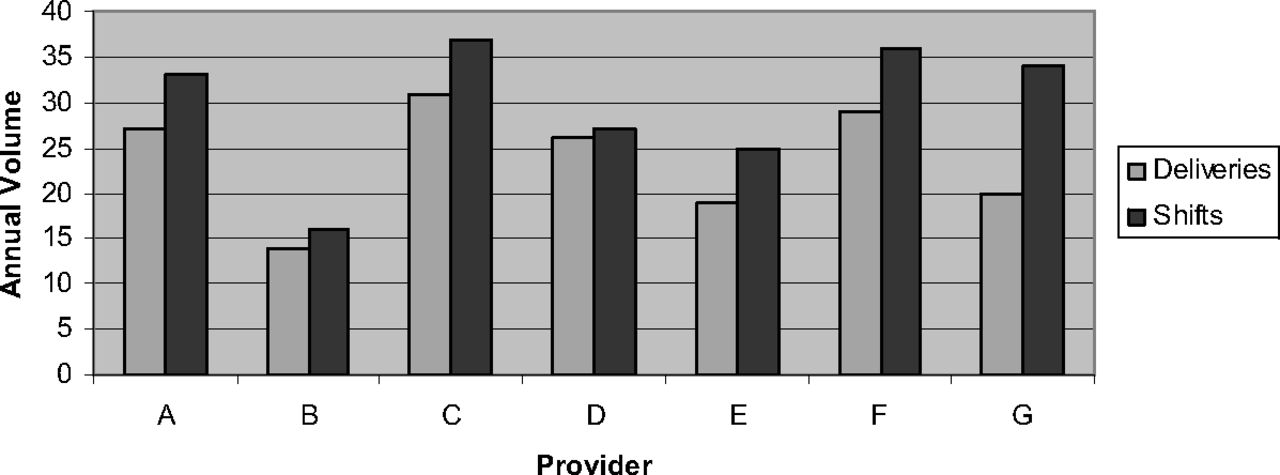
Shifts and deliveries per provider, July 2010 to June 2011.

Deliveries by fellowship-trained faculty, July 2010 to June 2011.
The laborist model has increased job satisfaction for obstetricians by offering a flexible schedule and addressing work load stressors. It a may also provide safer labor and delivery care in a manner that is acceptable to patients.31 The concept mirrors the hospitalist model in adult and pediatric inpatient care. We have seen a trend in family medicine programs, including ours, to employ “hospitalists” or hospital-focused faculty to staff inpatient adult medical services. With 2 obstetric fellowship–trained faculty members who focus on inpatient maternity and newborn services only, spending 36 hours per week in labor and delivery and additional hours with the postpartum and newborn inpatient service, we present a parallel model for a family physician “maternal-child health hospitalist.” This role ensures consistent teaching for our residents, reliable staffing, and content experts within our department. Because we train both obstetrics and family medicine residents, it is important to have enthusiastic faculty with a special interest in maternal-child health who can be expert teachers and model advanced skills that family physicians can achieve competence in, if desired. It offers an additional career option for those who have a strong interest in maternal-child health, including those who do not choose to maintain a robust outpatient practice.
Our collaborative team, however, values all members who practice labor and delivery care, including non–fellowship-trained family physicians and midwives, even in the midst of our high-risk patient mix. We keep a balance of non–fellowship-trained faculty in our group because they also are important role models for the trainees we work with, showing excellence in the practice of routine intrapartum care and the integration of labor and delivery care into a full-spectrum family medicine career. Some of our faculty chose to discontinue intrapartum care during our transition. These faculty would have had to commit a significant amount of faculty development to practice safely and teach effectively and had the support of the department if they had so chosen. Helton et al32 similarly observed a decrease in the number of family medicine faculty providing maternity care during a time of change in their maternal-child health program. However, we believe that in the long run, the team we have created will be more supportive of a range of family physicians who provide intrapartum care. Our faculty become highly competent and are able to enjoy their practice of maternity care because they are supported by an organizational framework rather than individual heroic faculty dedication or effort.
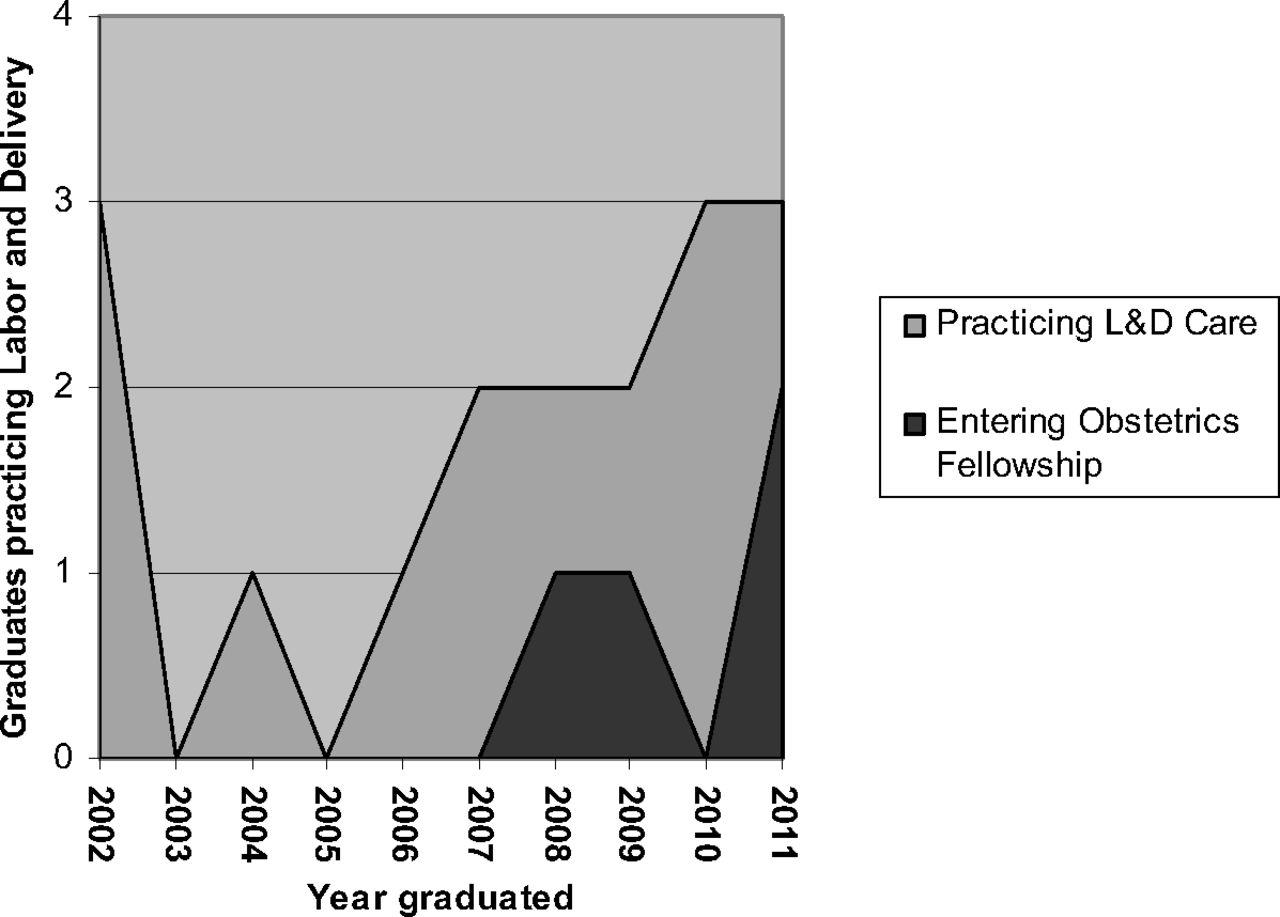
The Residency Assistance Program Criteria for Excellence has proposed replacing the current Residency Review Committee requirements with tiered levels of training for maternity care, which will increase the current Residency Review Committee requirements toward competence in intrapartum care while allowing trainees who are not interested in labor and delivery care to have minimal exposure.33 We have yet to discover whether changing the requirements for maternity care during training will change the number of graduates who choose to practice intrapartum care. Studies consistently show that providing strong role models and exposure to a collaborative relationship with obstetricians and midwives are vital in encouraging family medicine residents to practice maternity care after graduation.34,35 The diversity of our maternity care team shows our residents a variety of careers including maternity care, that are fulfilling and realistically sustainable, a characteristic that is likely to be increasingly important for future graduates.36⇓–38 Although our numbers are small, we have seen a recent increase in the number of residents choosing to include obstetrics in their first jobs after residency (Figure 5). It is too early to determine if the trend will persist and whether it is related to exposure to robust faculty role models, a collaborative labor and delivery experience, or both. A formal survey of our graduates regarding their experience with and attitudes toward obstetrics and their reasons for including or excluding obstetrics in their current practice will better address the true impact of our model once a sufficient number of graduates are available.

Inclusion of labor and delivery (L&D) in graduates' practices.
We also are hopeful that our collaboration and supervision of residents in the Departments of Pediatrics and Obstetrics will change the climate for family physicians practicing maternal-child health. Unfortunately, negative attitudes about the competency of family physicians exist.15 In the absence of successful models such as ours, this may hinder the willingness of our colleagues in these disciplines to collaborate and provide back-up services and may discourage future graduates from providing maternity services. Obstetricians who work with family physicians who deliver are more likely to be supportive of them.39 We anticipate that our family medicine faculty will influence the obstetrics residents graduating from our hospital and encourage them to support or back up family physicians who deliver in their future communities.
Fortunately, in our case, the recognition of and response to a culture of poor communication and waning family medicine skills was precipitated by an opportunity to increase the number of women receiving care at our hospital rather than as a result of an adverse intrapartum event. For this reason, our model may not be easily reproduced because it occurred during a time of special circumstances and required financial support from the hospital. The hospital was interested in supporting the collaboration because it sought to improve the safety and efficiency of care. This model was one of a number of patient safety initiatives at our hospital that contributed to a decrease in the number of malpractice claims.38
Collaborating with inpatient and outpatient partners has been crucial in ensuring our provision of safe maternity care and exemplary role models for our trainees. We focused on developing a collaborative environment with other departments for inpatient services and were able to respond to increased patient volume during a time when existing hospital systems were already operating at full capacity. Interdisciplinary models in Canada have been successful in increasing the numbers of family physicians practicing labor and delivery care.40,41 Some communities have been successful in increasing maternity care volume with collaboration with family physicians in the outpatient setting in the community. Others describe sharing practices or calls with obstetricians and midwives.40,41 Each community offers unique partners for collaboration that could improve patient safety and support a vibrant maternal-child health practice. There may be partners who are overstretched or who would prefer to participate in more lucrative activities. We recognize that the practice of maternity care, particularly intrapartum care, is difficult to sustain by heroic individual efforts but reflect on the value of preserving family medicine's role in the delivery of maternity care, a core event in the life of a family. We challenge each practice to look at their health care communities and search for potential team partners that could strengthen or revive maternity care in their practice.
Acknowledgments
We wish to acknowledge Brian Jack, MD; Aviva Lee-Parritz, MD; Ronald Iverson, MD, MPH; and Julie Mottl-Santiago, CNM, MPH, for their vision of collaboration and their dedication to making the model successful. We also thank Mayra Mieses for her assistance in compiling data for this manuscript.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication May 2, 2011.
- Revision received February 13, 2012.
- Accepted for publication February 20, 2012.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}