
Abstract
Background: Primary care physicians and patients perceive that they lose contact with each other after a cancer diagnosis. The objective of this study was to determine whether colorectal cancer (CRC) patients are less likely to see their primary care physicians after cancer diagnosis.
Methods: This was a longitudinal cohort study using 1993 to 2001 Surveillance Epidemiology and End Results (SEER)-Medicare claims data. Eligible patients were those with stage 0 to 1 and 2 to 3 CRC aged 67 to 89 years at diagnosis. Main measures included the proportion of individuals with a face-to-face primary care visit and mean annual primary care visits per patient at baseline and during 5 years after treatment.
Results: Fewer than half of the cancer patients visited with a primary care physician at baseline. In the first year after treatment, patients with stage 0 to 1 CRC (48.9% vs 53.3%; P ≤ .001) and stage 2 to 3 CRC (43.6% vs 53.4%; P ≤ .001) significantly increased their likelihood of visiting a primary care physician from baseline. The proportion of patients with stage 0 to 1 CRC with a primary care visit remained relatively stable, and the proportion of patients with stage 2 to 3 CRC decreased somewhat between the first and fifth year after treatment. The findings for mean annual primary care visits per patient roughly paralleled those for the proportion of individuals with a primary care visit.
Conclusions: Elderly patients with CRC, especially stage 2 to 3 CRC, increase rather than decrease contact with primary care providers after diagnosis. More work is needed to understand the care that different physician specialties provide cancer patients and to support their collaboration.
Patients diagnosed with cancer enter an intense world of specialized care, including surgery, chemotherapy, and/or radiation therapy, to treat and manage their disease. Although other chronic illness care and preventive health recommendations persist throughout and after cancer treatment, both patients and primary care providers perceive that they lose contact with one another after a cancer diagnosis.1–3
Patients express the desire to maintain contact with their primary care providers during cancer care.3–5 They value these providers' involvement in managing their chronic diseases and acute needs, as well as in providing clarification and support during cancer treatment.1,6 At the same time, primary care providers want to stay involved with their patients with cancer,2,5,7–10 providing care for treatment side effects, surveillance for recurrence, care of noncancer conditions, and coordination of care.5,7–10 Research has demonstrated that management of health screening and chronic illness care after cancer is improved when patients are seen by both cancer specialists and primary care providers,11,12 suggesting that an ongoing primary care relationship is important throughout cancer care.
This longitudinal study examines whether, as patients and providers perceive, patients are less likely to visit their primary care providers after colorectal cancer (CRC) diagnosis relative to before diagnosis. These findings can help to determine whether efforts to ensure that cancer patients receive chronic disease and preventive care should focus on increasing visits to primary care providers or on better coordinating care between cancer care and primary care providers.
Methods
Data Sources
This study used Surveillance, Epidemiology, and End Results (SEER) cancer registry data from 1993 to 1999, linked with 1991 to 2001 Medicare claims. SEER data include patient demographics and cancer type and stage. Medicare data include enrollment dates, health maintenance organization membership, patient demographics, and, for fee-for-service beneficiaries, billed claims that include diagnoses, tests, and procedures provided in hospitals, physician offices, and clinics. The American Medical Association Physician Masterfile data linked to the Medicare claims provided physician specialty.
Study Phases
Study phases included baseline year (12 months before treatment phase); the 7-month treatment phase (month before the diagnosis month through fifth month after diagnosis month); and after treatment (up to five successive 12-month periods after treatment phase). We excluded treatment phase data because we expected justifiably few primary care visits. At the time of this study, standard treatment was surgery alone for stages 0 to 1 CRC patients and surgery plus six cycles of chemotherapy for stage 2 to 3 CRC. We expected the most intensive treatment to be completed for the majority of patients with stage 0 to 3 CRC by the end of the 7-month treatment phase.
Study Population
Cancer patients were aged 67 to 89 years at diagnosis, had stage 0 to 3 CRC with typical histologies, were not diagnosed at autopsy, and had diagnosis month and year recorded (n = 64,410). We distinguished between patients with early-stage (stages 0 to 1) and later-stage (stages 2 to 3) CRC because prior analysis showed they differed in receipt of noncancer care.13
We excluded individuals without continuous enrollment in fee-for-service parts A and B Medicare from baseline through the first year after treatment, leaving 22,161 patients with CRC. Successive years after treatment were included if the individuals remained alive and had continuous enrollment (Table 1). The majority of attrition from both stage 0 to 1 and stage 2 to 3 CRC study groups was because of disenrollment rather than death (more than 80% for the group with stage 0 to 1 CRC and more than one third for the group with stage 2 to 3 CRC).
Number of Persons in Each Study Observation Year by Study Group
Study Variables
Our study outcomes were proportion of individuals with a primary care physician visit and the mean annual primary care visits per patient during each observation year. Unique visits were claims for face-to-face, nonprocedural services occurring in physician offices, patient homes, or clinics with the same date of service; provider identifier; and beneficiary identifier. Primary care physicians had a primary specialty of family medicine, general internal medicine, or pediatrics (to ensure all physicians with combined general internal medicine/pediatrics training were included), and they had no more specialized, secondary specialty in the American Medical Association Physician Masterfile (or a Centers for Medicare and Medicaid Services specialty code for these specialties from the carrier claims if Masterfile data were unavailable).
For descriptive purposes, we defined demographic variables (patient sex, race); ecological variables (ZIP code–based median annual household income); reason for initial Medicare entitlement; and calculated comorbidity using the National Cancer Institute combined CRC-specific comorbidity index14 during the year before baseline. This index, an adaptation of Charlson et al's15 comorbidity index, is based on 13 conditions identified from diagnoses on both inpatient and outpatient claims (renal disease, congestive heart failure, dementia, chronic pulmonary disease, cerebrovascular disease, paralysis, diabetes with and without complications, peripheral vascular disease, rheumatologic disease, acute myocardial infarction, prior myocardial infarction, ulcer disease) and uses weights specific to patients with CRC.
Analysis
We described the cancer patient groups (patients with stage 0 to 1 CRC and patient with stage 2 to 3 CRC) then calculated the proportion of individuals with primary care visits and the mean annual primary care visits per patient by group during the baseline year and for each observation year after the treatment phase. We analyzed whether there were differences over time within each study group using χ2 and standard t tests, as appropriate.
Results
The majority of both stage 0 to 1 CRC and stage 2 to 3 CRC study groups were women, white, eligible for Medicare because of age, and living in ZIP codes with more than $30,000 in median household income (Table 2).
Characteristics of the Study Population at Baseline
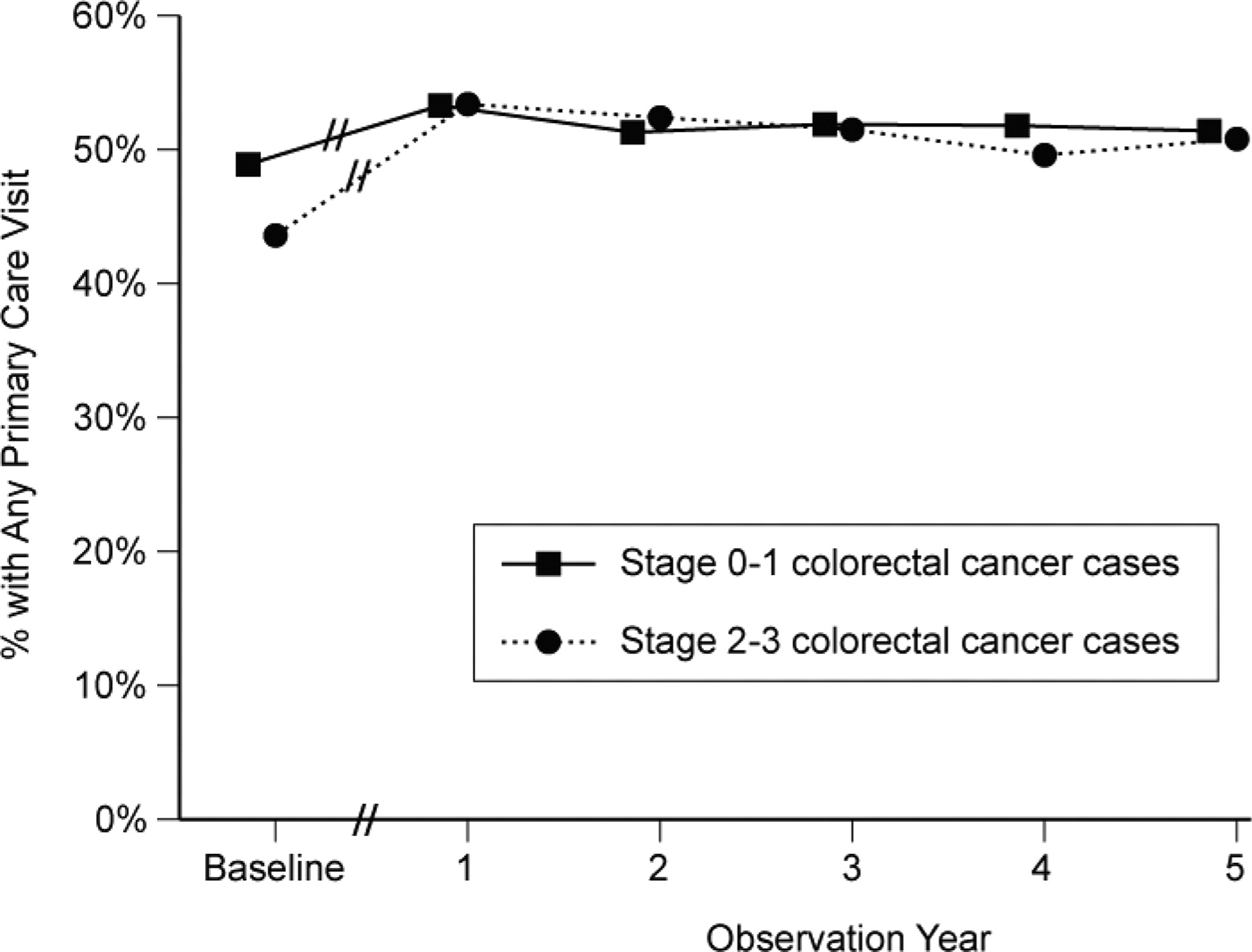
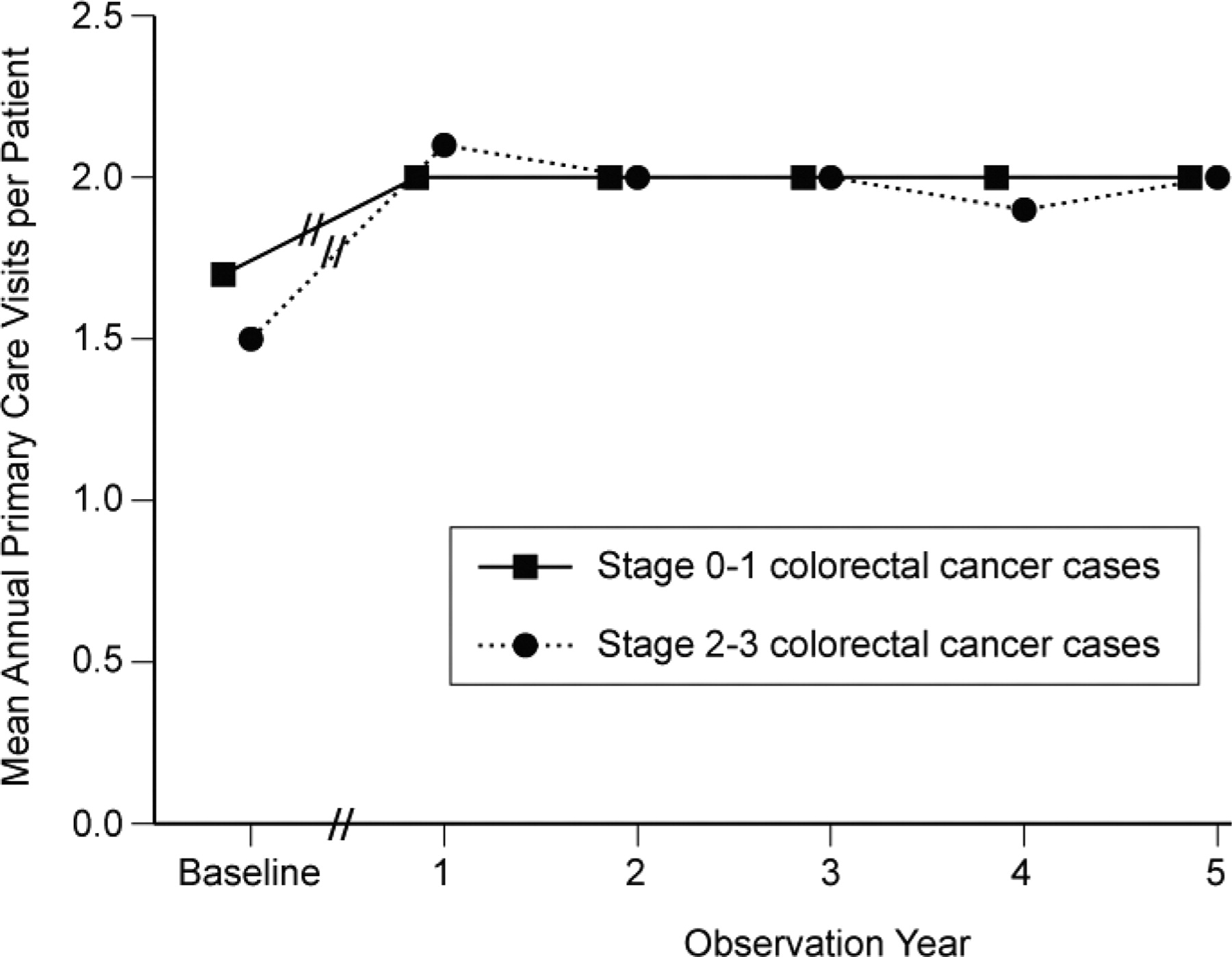
Fewer than half of the two study groups visited with a primary care physician during the baseline year (Figure 1). During the first year after treatment, patients with stage 0 to 1 (48.9% vs 53.3%; P ≤ .001) and stage 2 to 3 (43.6% vs 53.4%; P ≤ .001) CRC significantly increased their likelihood of visiting a primary care physician from baseline. Patients with stage 0 to 1 CRC had a minor decrease in the second year after treatment (53.3% to 51.3%; P ≤ .01) then remained stable until the fifth year after treatment. The proportion of patients with stage 2 to 3 CRC who visited a primary care physician decreased between the first and fourth year after treatment (53.4% vs 49.6%; P ≤ .001) then remained stable in the fifth year after treatment (50.8%). These lower proportions of stage 2 to 3 CRC visiting a primary care physician in the fourth and fifth years after treatment were still significantly higher than the proportion at baseline. The findings for the outcome—mean annual primary care visits per patient—paralleled the findings for proportion of individuals with a primary care visit (Figure 2).
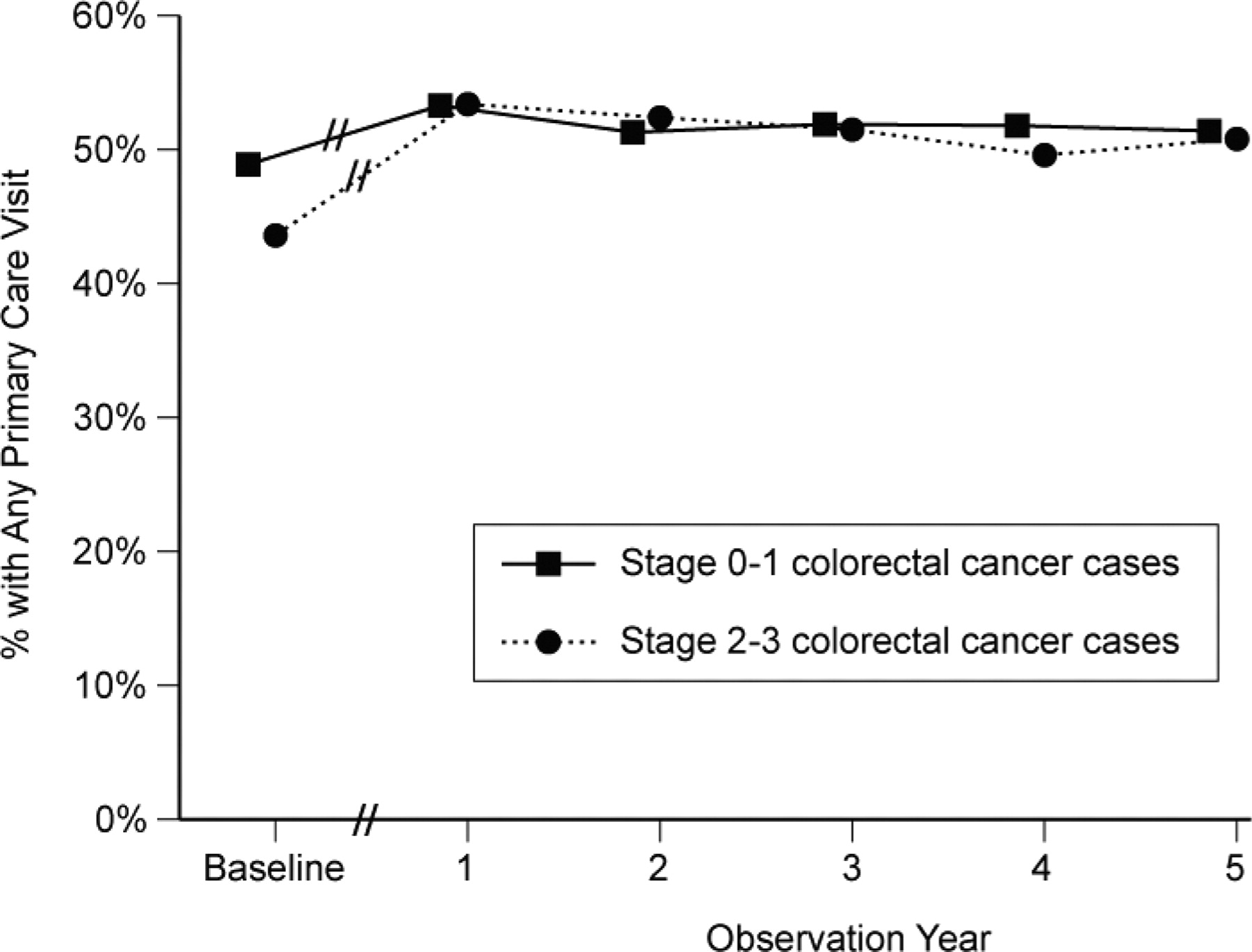
Proportion of colorectal cancer patients with a primary care visit over the observation period. // indicates that the beginning of observation year 1 lags by 7 months from the end of the baseline year. We excluded this treatment phase because we expected primary care visits to be superseded by frequent cancer-related care during this time.

Mean annual primary care visits per patient among colorectal cancer patients over the observation period. // indicates that the beginning of observation year 1 lags by 7 months from the end of the baseline year. We excluded this treatment phase because we expected primary care visits to be superseded by frequent cancer-related care during this time.
Discussion
Our study asked, Do patients continue to visit primary care physicians after a colorectal cancer diagnosis? Contrary to patients' and primary care providers' perceptions,1–3 this study found that older patients with CRC increase their likelihood of seeing primary care physicians after cancer diagnosis and treatment, and this higher rate continues through the first 5 years after diagnosis and treatment. Other research has found that, over time, cancer survivors have stable rates of seeing primary care providers,12,16 but this study is the first to demonstrate the increase in primary care use after cancer diagnosis.
Why do patients and primary care physicians perceive a loss of contact with one another when their contact actually increases initially, especially for CRC patients with more advanced disease? One hypothesis is that, for patients with CRC, visits with primary care physicians are relatively infrequent compared with visits with cancer care specialists. In turn, primary care physicians may perceive a loss of contact if they know their patients are in intensive treatment yet they receive limited or delayed information about that care.7,8,10 Lastly, we did not measure visits during the 7-month treatment phase because we expected primary care visits to be superseded by frequent cancer-related care during this time. Perhaps a lower primary care visit rate during that period fuels provider perception that they lose contact with their patients.
Despite their more intensive cancer treatment regimens, patients with stage 2 to 3 CRC are significantly more likely to see primary care providers after cancer diagnosis, suggesting that diagnosis has altered their care-seeking behavior. Perhaps, as Denmark-Wahnefried et al17 suggest, cancer diagnosis provides a teachable moment when individuals are more willing to hear health promotion messages and participate in activities and lifestyle modifications that optimize health. Primary care visits may represent important opportunities to influence prevention and management of other health conditions as well as monitor for cancer recurrence and short- and long-term treatment effects.
This study's limitations include lack of generalizability because of inclusion of only elderly patients with CRC who receive fee-for-service Medicare. Younger cancer patients with fewer chronic conditions may visit primary care physicians differently. Other studies have shown greater proportions of patients have access to or see primary care physicians; they include more specialties and a broader range of visit codes.16,18 Our study, using only face-to-face nonprocedural visits, may have underestimated the total primary care visits for both CRC patients and controls.
Attrition in the stage 0 to 1 and stage 2 to 3 CRC groups over the study years was dominated by disenrollment from Medicare fee for service to Medicare health maintenance organizations. Research has demonstrated that patients moving from enrollment in Medicare fee for service into health maintenance organizations are healthier.19,20 Thus, because of this phenomenon and aging, over time the comorbidity of our study cohorts and their visits to primary care physicians will increase. However, between baseline and the first observation year, when the study sample had no shifts from death and disenrollment, there was a significant increase in primary care visits. Regardless of these influences, our study's conclusion does not change: primary care physicians continue to see their patients with CRC as much or more after diagnosis.
Patients with CRC receive ongoing primary care after cancer treatment; for patients with stage 2 to 3 CRC, it is more often than before the diagnosis. Some work suggests that patients seeing both their oncology team and their primary care physicians obtain the greatest benefit in delivery of preventive services.12 Other work describes an independent benefit of care provided by primary care providers.21–24 Future research is needed to characterize the components of care provided by different specialties to cancer patients and to seek ways to support the collaboration between the physicians involved in their care.
Acknowledgments
The authors would like to thank Barbara Matthews for her assistance in developing the database used in this research; Denise Lishner for carefully documenting the work of the research team; and Roger A. Rosenblatt, MD, MPH, MFR, for his advice on study development and design.
Notes
-
This article was externally peer reviewed.
-
Funding: Funding was provided by the National Cancer Institute (grant no. 1 RO1 CA104935).
-
Conflict of interest: none declared.
- Received for publication August 24, 2010.
- Revision received June 4, 2011.
- Accepted for publication June 15, 2011.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Regional Variation in Primary Care Involvement at the End of Life
- Primary care physician use across the breast cancer care continuum: CanIMPACT study using Canadian administrative data
- Sharing Care to Achieve the Triple Aim of Health Care Delivery
- Change, Lack of Change, and Creating Optimal Change Out of Chaos