
Abstract
Background: Frail elders often receive low-quality primary care, yet the optimal role of geriatricians in primary care settings remains uncertain. We evaluated the health utilization impacts of an innovative intervention emphasizing chronic disease self-management and physical activity promotion among frail elders in primary care.
Methods: The intervention was implemented within two primary care practices at a single clinic serving a large population of frail elders enrolled in a western Washington health plan. Subjects included older patients (age ≥65 years) with disproportionate baseline outpatient service use who attended two on-site visits with a geriatrician during which each received comprehensive assessment and a problem-solving intervention to enhance chronic disease self-management and promote physical activity (N = 146). Our evaluation had a retrospective matched cohort design. Controls receiving primary care at other health plan clinics were matched 3:1 to intervention subjects by sex and a propensity score (N = 437), which was computed using demographic, clinical, and health care utilization factors that were predictive of attending the intervention. Among intervention subjects and controls following the intervention, we compared relative rates of hospitalization, outpatient and specialty visits, nursing home admission, mortality, and prescription of selected high-risk medications, as well as total health care costs.
Results: From March 2002 to November 2003, the geriatrician evaluated 146 of 725 elderly subjects (20%) in the two primary care practices. During a mean follow-up of 1.3 years, intervention subjects had a reduced rate of hospitalization relative to matched controls (incidence rate ratio 0.57; 95% CI: 0.37 to 0.86; P < .01). Intervention and control subjects did not have significantly different rates of specialty visits, outpatient visits, nursing home admission, mortality, or high-risk prescriptions. Relative to matched controls during follow-up, total health care costs were 26.3% lower among intervention subjects (95% CI: 1.3%, 44.9%; P = .04).
Conclusions: Outpatient geriatric interventions emphasizing collaboration between geriatricians and primary care physicians, chronic disease self-management, and physical activity may reduce hospitalization risk and total health care costs among vulnerable elders.
The number of older Americans with chronic disease or disability is expected to increase severalfold in the coming decades.1 Health care organizations will be challenged to adapt delivery systems to serve older patients, who frequently receive deficient care from primary care physicians.2 Geriatricians receive specialized training in the outpatient care of vulnerable elders, yet the ideal role of geriatricians in the outpatient setting remains ambiguous.3
Outpatient interventions involving geriatricians have yielded mixed results in previous studies. In comprehensive geriatric assessment, a multidisciplinary geriatric team assesses patients’ medical, cognitive, functional, and nutritional needs and provides detailed management recommendations to primary care physicians. When paired with outreach to improve adherence to recommendations among primary care clinicians, comprehensive assessment has preserved physical function and improved health-related quality of life among high-risk elders.4 Other geriatric interventions with close links to primary care have been associated with reduced risk of hospitalization, including: a senior center-based disability prevention program,5 multidisciplinary team primary care emphasizing chronic disease self-management,6 and primary care-based group medical visits.7 Positive studies, however, contrast with studies of brief outpatient geriatric interventions that have found little or no effects on clinical outcomes or health service use.8,9 In addition, ongoing geriatric management has improved some functional outcomes but has not affected health care utilization.10–12
We evaluated the effect of an innovative outpatient quality improvement intervention in which a fellowship-trained geriatrician assessed the most vulnerable elders in two primary care practices and delivered a problem-solving intervention to enhance chronic disease self-management and promote physical activity. We hypothesized that the intervention would be associated with reduced rates of hospitalization and prescription of high-risk medications without increasing outpatient visit use. We also hypothesized that the geriatrician would address many management concerns of patients’ primary care physicians, thereby reducing rates of specialty referral.
Methods
Design and Setting
Our evaluation had a retrospective matched cohort design. The intervention was implemented in March 2002 within two physician practices at a single primary care clinic within Group Health Cooperative (GHC), a not-for-profit health maintenance organization serving over 500,000 enrollees in Washington state. The clinic serves a middle-income community south of Seattle. Health plan administrators selected the clinic for the intervention because it serves a disproportionately large population of frail elders with high hospitalization rates relative to other health plan clinics. We designed the evaluation after implementation of the intervention so could not perform a prospective clinical trial. The study protocol was approved by the GHC Human Subjects Review Committee.
Subjects
We included in the intervention cohort all subjects over age 65 years from the 2 physician practices who received the intervention from March 2002 to November 2003 and were continuously enrolled in the health plan from 2 years before their index visit with the geriatrician until either death or the end of the study period (24 March 2004) (N = 146). In March 2002, clinic staff used administrative data to rank patients over age 65 years from the 2 practices by the frequency of outpatient visits during the prior year. Staff then sequentially telephoned patients with the most frequent use of outpatient services and informed them that their primary doctor recommended that they attend on-site visits with a geriatrician. The geriatrician attended patients at the clinic for half a day per week and saw one patient per hour. Staff extended invitations to the ranked patients at a rate sufficient to fill the geriatrician’s weekly schedule. The two primary care physicians also occasionally referred elderly patients directly to the geriatrician. Because of the retrospective study design, we could not ascertain which patients were invited to receive the intervention. During the study period, 146 of 725 older patients (20%) in the 2 practices received the intervention.
Control subjects were drawn from the population of patients over age 65 years with primary care physicians at 3 other GHC clinics south of Seattle. We selected the 3 control clinics because each serves a community with sociodemographic characteristics similar to the community served by the intervention clinic. Because intervention subjects were selected from 2 target physician practices, we matched 3 controls to each intervention subject by sex and a propensity score, which was derived to account for factors that predicted selection for the intervention (see Data Analyses). Only 2 matched controls were available for one intervention subject, so the control population totaled 437 subjects.
Geriatric Intervention
The intervention consisted of 2 planned visits with a fellowship-trained geriatrician. The initial visit focused on systematic assessment to identify risk factors for functional decline and included: (1) standardized assessment of psychosocial, cognitive, and physical function and physical activity; (2) screening for pain, depression, dementia, urinary incontinence, fall risk, and substance abuse; (3) review for use of medications with frequent adverse side-effects in elderly patients; and (4) focused physical examination. The geriatrician devoted approximately 30% of the initial visit to each of the first 3 tasks and approximately 10% to physical examination.
The geriatrician devoted the entire second visit to collaborative problem-solving with the following goals: (1) to ameliorate threats to quality of life and functional independence; (2) to promote appropriate physical and social activity; and (3) to enhance chronic disease self-management. During the problem-solving intervention, the geriatrician sought to help the patients prioritize their health-related goals and to identify practical steps toward those goals. The geriatrician often used open-ended questions to encourage patients to articulate their health concerns (eg, “How have you been feeling lately?”) and possible solutions (eg, “What do you think you could do to help that problem?”). To foster patient self-efficacy, the geriatrician encouraged patients to set feasible, short-term health goals. Whenever possible, the geriatrician sought to activate the patient both physically and socially and often referred patients to exercise and social programs at a local senior center. When counseling patients regarding chronic disease self-management, the geriatrician emphasized skill development and self-monitoring, consistent with principles outlined in Living a Healthy Life with Chronic Conditions.13
The geriatrician spoke with the primary care physicians after weekly clinic sessions, which provided opportunity to discuss new recommendations and to provide informal consultation regarding ongoing management. The geriatrician also sent to the primary care physicians a consultation letter regarding each patient that summarized the prioritized problem list, the patient’s treatment goals and plans for action, and recommendations for evaluation and management.
Data Sources and Measurements
Study variables were derived from automated administrative, clinical, and pharmacy databases at GHC, which have been used extensively for research. For intervention subjects and matched controls, we assigned an index date that was the date of each intervention subject’s initial visit with the geriatrician. We then determined counts of the following utilization outcomes during the year preceding the index date and from the index date to 24 March 2004: hospitalizations, medical/surgical specialty visits, outpatient visits (including the intervention visits), admissions to nursing facilities, and the number of 14-day equivalent prescriptions of selected medications that cause frequent sedative or anticholinergic side effects in elderly patients, including sedating antihistamines, selected tricyclic antidepressants (amitriptyline and doxepin), muscle relaxants, and sedative-hypnotic agents. We ascertained mortality during follow-up from health plan administrative databases. We also collected the International Classification of Diseases, 9th Edition, Clinical Modification (ICD-9-CM) diagnostic code for the principal discharge diagnosis for subjects’ hospitalizations during the baseline and follow-up periods.
GHC identifies health care costs for enrollees by integrating automated data for clinical care episodes with actual cost data from the general ledger, including costs for direct patient care within clinical departments and shared overhead (eg, information systems). In addition to overhead costs, total health care costs include costs for clinical staff salaries, drugs, laboratory, radiology, hospital inpatient care, outpatient services, and community health services. GHC costing algorithms have been designed to estimate the actual cost of delivered services and have been used extensively for research.14,15
The presence of diabetes and heart disease was ascertained from disease-specific registries used for clinical care within the health plan. The presence and date of diagnosis of non-skin cancers was ascertained from the regional Surveillance, Epidemiology, and End Results cancer registry. Subjects were classified as having dementia and/or Parkinson’s disease if one of the following ICD-9-CM diagnostic codes appeared on at least two outpatient or inpatient encounters at least 3 months apart during the 2-year period before each subject’s index date: 290.x, 331.0–331.2, 332.x. Subjects were classified as having recent depression if one of the following codes appeared during any encounters during the 3 months before the index date: 296.2, 296.3, 311.x. For each subject, we computed a validated, pharmacy-derived index of chronic disease comorbidity (RxRisk).16
To enable adjustment for additional covariates, we subsequently included socioeconomic and comorbidity variables that became available after initial data collection and analyses. In particular, we linked study subjects enrolled in GHC in January 2005 to the following year 2000 Census data: (1) block-level proportion of adults over age 25 years of non-white race; (2) block-group median household income; and (3) block-group proportion of adults over age 25 years who graduated from high school. For all study subjects, we also used automated ICD-9-CM diagnostic data from the 12 months before their index date to compute a version of the Charlson comorbidity index.17
Data Analyses
We used propensity score matching to account for selection biases that may have been introduced during the recruitment of intervention subjects.18 We developed propensity scores using baseline demographic, clinical, and pharmacy data among the 725 potentially eligible elderly subjects in the two target practices. First, we used stepwise logistic regression to build a nonparsimonious model to predict receipt of the intervention among these subjects. The final model had moderate discriminative ability (C-score = 0.74) and included the following 7 baseline factors (listed by strength of association with intervention receipt): number of outpatient visits, square of the number of outpatient visits, age ≥83 years, highest quartile of RxRisk comorbidity index, age 77 to 83 years, presence of heart disease, and one or more hospitalizations. Second, we constructed a prediction equation based on the final model to estimate the probability of receiving the intervention based on subjects’ baseline characteristics. We then computed the estimated probability, or propensity score, for the 146 intervention subjects and potential controls from the three similar health plan clinics. Finally, we matched 3 controls to each intervention subject by sex and propensity score (±0.03). When several potential matches were found, we selected the closest possible matches. The Census-linked socioeconomic variables, Charlson comorbidity index, and baseline health care cost data were not available at the time of propensity matching.
We compared baseline demographic, clinical, and utilization factors of intervention subjects and controls using t tests, χ2, and Fisher’s exact tests. We then calculated crude utilization rates of outcomes following the index date (events per 100 person-years) among intervention subjects and controls and compared rates among the 2 groups by calculating crude incidence rate ratios (IRR) and 95% confidence intervals (CI). We then used negative binomial regression to estimate rate ratios of outcome events among intervention and controls conditional on propensity score.19 We then repeated the conditional analyses while adjusting for covariates that were unbalanced at baseline (P < .10). We used ICD-9-CM codes for principal discharge diagnoses to compute crude and relative rates of hospitalization across various diagnostic categories among intervention subjects and controls.
Cost data were log-transformed before analysis to normalize distributions. We then used random-effects linear regression to estimate adjusted total cost differences among intervention subjects and controls while accounting for propensity score matching, follow-up duration, and unbalanced baseline covariates (P < .10).20 All subjects accrued costs during the follow-up period, so we chose a one-part cost model.21 Due to either death or health plan disenrollment before 2005, Census-linked data on race were missing for 105 subjects (18.0%), and income and education data were missing for 89 subjects (15.3%). These covariates, therefore, were used primarily for sensitivity analyses. Cost data were missing or incomplete for 51 subjects (8.8%), but were missing or incomplete for 30 of 47 subjects (63.8%) of the subjects who died during follow-up. Hypothesis tests were two-sided with an α of 0.05.
Results
Subject Characteristics
The subjects had a mean age of ∼78 years, had high prevalence of comorbid chronic disease, and attended a mean of 18 outpatient visits during the year before index date (Table 1). Approximately 1 in 5 had been hospitalized during the baseline year. At baseline, intervention and control subjects were similar with regard to age, gender, socioeconomic characteristics, clinical characteristics, prior health care utilization, and median health care costs. Intervention subjects had slightly greater mean age (P < .10) and higher prevalence of heart disease and dementia and/or Parkinson’s disease (P < .10), whereas the mean block-level proportion of non-white adults was higher among controls (P = .01).
Baseline Demographic, Clinical, and Utilization Characteristics of Intervention Subjects and Matched Controls
Hospitalization Rates
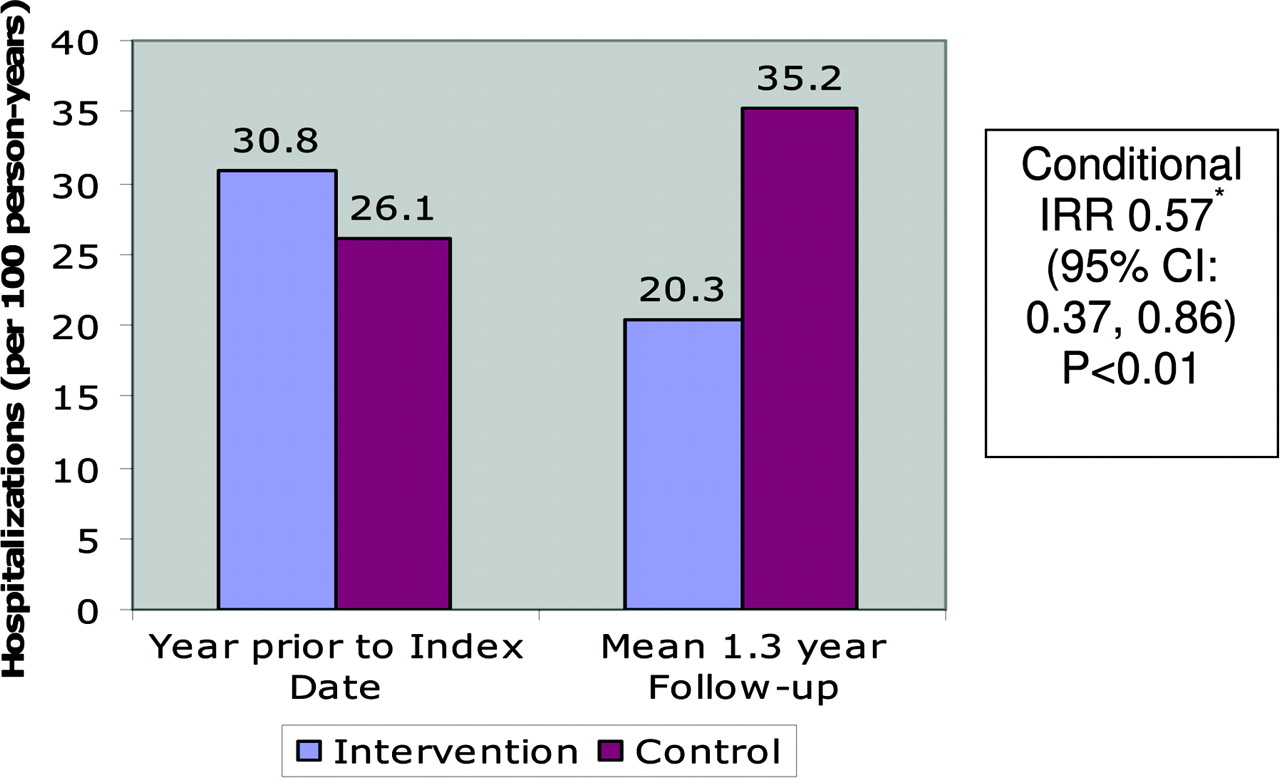
As shown in Figure 1, hospitalization rates during the baseline year were similar in the two groups. During a mean follow-up of 1.3 years, intervention subjects were hospitalized at a rate of 20.3 per 100 person-years compared with 35.2 per 100 person-years among matched controls. After the index visit with the geriatrician, the rate of hospitalization was 43% lower among intervention subjects relative to matched controls [conditional IRR 0.57 (95% CI: 0.37, 0.86); P < .01]. The observed reduction in the relative hospitalization rate was unaffected by simultaneous adjustment for age, heart disease, and dementia/Parkinson’s disease, or addition of block group proportion of non-white adults to the fully adjusted model. In separate conditional models that adjusted individually for categories of household income, the proportion of adults with a high school education, and categories of the Charlson comorbidity index, the association between the intervention and relatively reduced risk of hospitalization remained similar.

Hospitalization Rates before and after Geriatric Intervention.
Reasons for Hospitalization
During the baseline period, the rates of hospitalization across various diagnostic categories were similar among intervention subjects and controls (Table 2). During the follow-up period, hospitalization rates were relatively lower among intervention subjects across a range of discharge diagnoses, including infections, degenerative musculoskeletal diagnoses (eg, osteoarthroses), fractures and injuries, neoplasms, and chronic obstructive pulmonary diseases. The association between the intervention and reduced hospitalization risk during post-index period was similar after excluding degenerative musculoskeletal diagnoses, which may predominantly comprise hospitalizations for elective surgery (conditional IRR 0.63; 95% CI: 0.41, 0.96).
Hospitalization Rates by Principal Discharge Diagnosis Before and After Index Date of Intervention
Other Health Services and Mortality
During follow-up, there were no significant differences in rates of medical/surgical specialty visits, total outpatient visits, nursing home admissions, or mortality (Table 3). Although crude rates of specialty visits and high-risk medication prescriptions were lower among intervention subjects, there were no significant differences in rates of these outcomes in adjusted conditional analyses.
Utilization Outcomes and Mortality Following Index Date among Subjects Receiving Geriatric Intervention and Sex and Propensity-Matched Controls*
Health Care Costs
After adjustment for age (linear and quadratic), heart disease, and diagnoses of either dementia or Parkinson’s disease, total health care costs during follow-up were 26.3% lower among intervention subjects relative to matched controls (95% CI: 1.3, 44.9; P = .04).
Discussion
In this evaluation, a primary care-based geriatric intervention emphasizing systematic assessment, chronic disease self-management, and physical activity promotion was associated with reduced risk of hospitalization and lower health care costs among chronically ill elderly health plan enrollees with high baseline rates of outpatient service use. Reduced rates of hospitalization did not require a compensatory increase in outpatient or specialty clinic visits. Hospitalization rates were relatively reduced across a range of diagnoses that are associated with frailty, including infections, fractures and injuries, and some chronic diseases.
The effect of geriatric intervention on health care utilization has been mixed in recent studies. Although geriatric assessment and management has not reduced hospitalization in three trials,10–12 our observation of reduced hospitalization risk is consistent with 3 recent studies of primary care-linked outpatient geriatric interventions.5–7 Alongside these, our evaluation suggests that certain features of our intervention may hold promise. First, our study intervention involved sustained, close collaboration between a geriatrician and 2 primary care physicians, and linkage or outreach to primary care physicians has been essential to other effective interventions among geriatric outpatients.4–7 Second, our intervention emphasized chronic disease self-management, which was a major component of 3 recent outpatient interventions that were associated reduced hospitalization risk among geriatric outpatients.5–7 Third, our intervention involved a patient-centered problem-solving session that guided treatment planning and recommendations. Agreement, or concordance, between care providers and geriatric patients has been associated with much higher adherence to recommendations after geriatric assessment.22 We believe the problem-solving session would have fostered concordance of this sort between patients and the clinicians in our evaluation, whereas similar levels of concordance may be difficult to achieve in models of geriatric intervention that rely on interdisciplinary team meetings. Last, our intervention promoted physical activity, and uptake of physical activity among seniors may reduce risk of functional loss, disability, and hospitalization.5,23,24
Our study intervention was associated with reduced rates of hospitalization for a range of diagnoses. Many of these diagnoses can contribute to frailty in older adults and would conceivably be sensitive to geriatric intervention. Increased physical activity following the intervention could have reduced subjects’ risk of hospitalization for infection, fractures and injuries, and falls (eg, syncope and collapse). By enhancing self-management of chronic disease and pain, the intervention could also have contributed to reduced risk of hospitalization for chronic obstructive pulmonary disease and osteoarthroses.25 Geriatric expertise may also have contributed to reduced hospitalization risk for advanced stage neoplasms. Our evaluation, however, is limited by the lack of data on patient uptake of physical activity, changes in chronic disease self-management, or other management changes that may have stemmed from the intervention. Moreover, we had limited power to estimate hospitalization rates within diagnostic categories, so relative rates of hospitalization by diagnosis should be interpreted cautiously.
We found that the intervention was associated with significantly lower total health care costs during the follow-up period, even after accounting for increased outpatient costs associated with the intervention. Pre-paid health systems, therefore, may have considerable financial incentive to foster collaboration between geriatricians and primary care physicians. Most US primary care practices, however, receive predominantly fee-for-service payment so they may lack financial incentive to adopt innovations that may reduce inpatient utilization.26 By aligning Medicare payments with quality improvement goals, federal policymakers might facilitate dissemination of potentially cost-saving interventions to improve chronic illness care for American seniors.27,28
The limitations of this evaluation require careful consideration. First, although propensity score matching can minimize selection biases, unmeasured confounding may explain the observed association between the intervention and reduced rates of hospitalization. Nevertheless, our approach modeled the process of selection of the intervention subjects from the entire elderly populations within the 2 primary care practices, and propensity score matching allowed us to control for a broad range of demographic, clinical, and utilization factors, including socioeconomic status, 2 validated comorbidity measures, and baseline hospitalization rates. Although our design cannot entirely exclude selection bias, we believe the potential merits of this innovative intervention deserve consideration in light of the strong association observed between the intervention and reduced hospitalization risk.
Second, we studied the effect of an intervention delivered by a single geriatrician among patients from two primary care practices in a managed care setting, and the generalizability of our findings to other physicians and practice settings is uncertain. Last, cost data were frequently missing or incomplete among subjects who died during the follow-up. However, mortality was similar among intervention subjects and controls, and a similar proportion of decedents in each study arm lacked complete cost data.
Our evaluation suggests that a time-limited primary care-based intervention may reduce risk of hospitalization and health care costs among high-risk elders and that the efficacy of outpatient geriatric interventions may be enhanced by close ongoing collaboration between geriatricians and primary care physicians. Our evaluation also suggests that problem-solving techniques to enhance chronic disease self-management and encourage physical activity may be effective elements of outpatient care of chronically ill community-dwelling elders. Our results need confirmation in randomized studies in diverse clinical settings.
Acknowledgments
We acknowledge the assistance of Peter Franks, Thomas Koepsell, James Logerfo, Matt Harmon, Roy Pardee, and Gene Hart. Socioeconomic and Charlson comorbidity data were provided by the Cancer Research Network (CRN) Virtual Data Warehouse. The CRN consists of the research programs, enrollee populations and databases of 11 integrated health care organizations that are members of the HMO Research Network. The health care delivery systems participating in the CRN are: Group Health Cooperative, Harvard Pilgrim Health Care, Henry Ford Health System/Health Alliance Plan, HealthPartners Research Foundation, the Meyers Primary Care Institute of the Fallon Health care System/University of Massachusetts, and Kaiser Permanente in six regions: Colorado, Georgia, Hawaii, Northwest (Oregon and Washington), Northern California and Southern California.
Notes
Funding: This study was funded by the Robert Wood Johnson Foundation. JJF was a Robert Wood Johnson Clinical Scholar during the early phases of this project.
The study results were presented at the Robert Wood Johnson Clinical Scholars Program Annual Meeting, 12 November 2004, Tucson, AZ.
Conflict of interest: MDL was employed by Group Health Cooperative as the intervention geriatrician and is now Medical Director of Senior Care.
Disclaimer: The statements herein are those of the authors and not necessarily those of the Robert Wood Johnson Foundation.
- Received for publication July 22, 2005.
- Revision received January 6, 2006.
- Accepted for publication January 24, 2006.




{kind=link}