
Abstract
Over 70% of the estimated 5 million office visits per year for migraine headache are to family physicians. Both the number of visits and proportion of migraine patients seeking medical care are increasing rapidly. Patient satisfaction with migraine care by primary care physicians is reported to be low but most data are obtained from patients referred to subspecialists or entered in clinical trials. We surveyed patients who consulted family physicians in 10 Kansas practices during 2002 to assess patient satisfaction and investigate any differences between satisfied and unsatisfied migraine patients. Of our 447 respondents, 74% were “satisfied” or “very satisfied” with migraine care by family physicians. Dissatisfied patients were significantly more likely to report moderate or severe migraine-related disability and less likely to use triptans or to have most medications paid by insurance. Dissatisfied patients were twice as likely to have discontinued taking triptans than satisfied patients. Patient satisfaction with migraine treatment in family practice is substantially higher than generally reported. Statistically significant differences exist between satisfied and dissatisfied patients.
Approximately 28 million Americans suffer from migraine headache.1 Until recently only approximately one third of migraineurs ever consulted a physician,2,3 but the number of physician visits for migraine jumped from 2.3 million in 1990 to over 5 million in 1998 and continues to increase.4 Recent estimates indicate that nearly 70% of patients with migraine have consulted a physician at least once5 and two thirds of these patients have made 5 or more physician visits for migraine. Over 72% of migraine-related physician visits are to primary care practitioners with the vast majority to family physicians.4
Unfortunately, studies report that less than 30% of migraineurs are highly satisfied with their current treatment.6,7 In one treatment study conducted in 15 primary care clinics, only 21% of migraine patients were satisfied or very satisfied with current care.8 Most studies reporting low patient satisfaction with primary care management of migraine are based on patients recruited for clinical trials8 or those referred to specialist headache centers.9 These groups could be expected to contain disproportionate numbers of patients who had not responded to first-line treatment and hence give a biased view of overall patient satisfaction with primary care management of migraine. As we could not find data on satisfaction with migraine treatment in unselected primary care patients in the literature, we included questions about satisfaction with treatment in a survey of patients who consulted family physicians for migraine during 2002. We aimed to assess overall levels of satisfaction with migraine management and to identify any significant differences between satisfied and dissatisfied patients.
Methods
An observational, cross-sectional study was conducted using a 15-item survey sent to adult patients who had consulted family physicians in 10 practices associated with the Kansas Practice Research Network during 2002. Patients were identified by use of migraine-specific International Classification Disease Ninth Revision codes for the consultation. The 5 rural practices served communities ranging from 835 to 6,313 population and were selected to represent the different regions of the state. Similarly, the 5 urban practices were selected to represent different demographic areas within the city of Wichita (population 344,284). The survey gathered demographic data and incorporated the standardized MIDAS questionnaire to assess migraine-related disability10 as well as questions about medications and satisfaction with treatment.
Patients received a cover letter from their personal physicians inviting them to participate in the study and to return the unnamed surveys directly to the primary investigator. Patients were assured that neither their personal physicians nor the researchers could identify participants and that their ongoing care would not be altered in any way by their participation in the survey or by the information provided. The study was approved by the University of Kansas School of Medicine Institutional Review Board.
Results
The 10 participating practices identified 992 patients aged ≥18 years who consulted at least once during 2002 for a migraine-related diagnosis. After 3 mailings, 447 surveys suitable for analysis were returned (response rate 45%). For individual practices, the number of patients surveyed ranged from 9 to 540, and the response rates were from 27.5 to 72%. Responders did not differ from nonresponders in age or gender distribution.
The respondents were predominantly female (83%) and the mean age was 44 years (range 18 to 82). Two thirds of the respondents had experienced migraine for >10 years, and most reported that migraine significantly impacted their lives. The standardized measure of migraine-related disability (the MIDAS score) was >10 in 60% of respondents, indicating moderate-severe migraine disability (Table 1). The majority of respondents (85%) had private insurance. Only 14% reported having no assistance with payment for migraine medications and 58% reported that “all” or “most” of their migraine medications were paid by insurance plans.
Migraine-Related Disability in Primary Care Patients
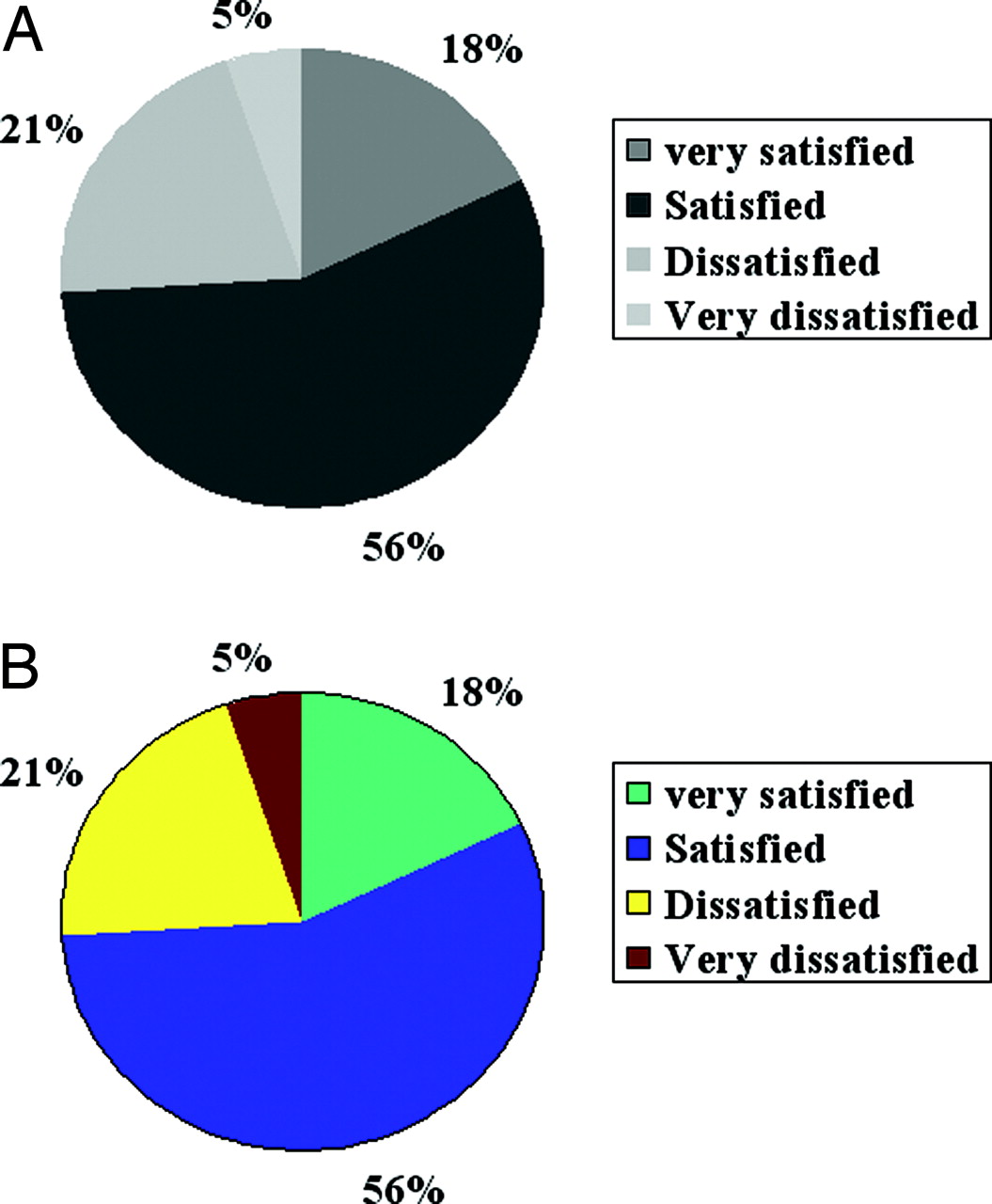
Overall, 74% of respondents were “satisfied” or “very satisfied” with medical treatment for migraine, and only 5% were “very dissatisfied” (Figure 1).

Patient Satisfaction with Migraine Treatment
Statistically significant differences were found in migraine disability (MIDAS scores), current use of triptan medication, history of discontinuing triptans, and insurance payment for migraine medications between satisfied and dissatisfied patients (Table 2). Dissatisfied patients were significantly more likely to report moderate to severe migraine-related disability and were less likely to report current use of triptans (38 compared with 61%). Although 80% of patients in both groups had tried triptans, dissatisfied patients were nearly twice as likely to have stopped using these medications as satisfied patients. Satisfied and dissatisfied patients did not differ significantly in age, gender, number of years with migraine, insurance type, use of prophylactic migraine medication or reported use of analgesics, combination medications, narcotics, ergots, “other ” or “no” medications to treat migraine attacks (Table 2).
Comparison of Satisfied and Dissatisfied Patients
Discussion
No large studies have directly assessed patient satisfaction with the treatment of migraine in primary care. Our results suggest it could be much higher than is commonly reported. Reports in the literature, usually based on patients referred for specialist care or those entering treatment studies, could bias results toward dissatisfied or more severely disabled patients, not representative of all primary care migraine patients. Nevertheless, our patients reported a high rate of satisfaction with care despite generally severe, disabling migraine of long duration. Both high MIDAS score and consulting a physician have been correlated with significantly lower rates of satisfaction with current therapy.11
The retrospective design means the study did not impact physician behavior or treatment for migraine patients. We did not attempt to verify that the patient met International Headache Society criteria for migraine12 for several reasons—mainly because studies have verified that a positive diagnosis of migraine by a family physician is 98% likely to be accurate.13 Examining how the accuracy of diagnosis and the various subtypes of migraine impact patient satisfaction would be interesting additions to a future study. Although International Classification of Disease-Ninth Revision coding has shortcomings as a technique of identifying a study population, it is reported to be very accurate for specific conditions such as migraine and for patients with insurance.14,15
This study was conducted in 5 urban and 5 rural practices in Kansas, representing a spectrum of communities and practice types. Furthermore, as minimal differences exist in practice patterns between family physicians who participate in research networks and all family physicians,16 these satisfaction rates may more accurately reflect the current status in primary care than the older studies and those using selected patient groups.
The low response rate and potential bias in patient selection are weaknesses of the study. Although surveys were returned directly to the researchers without identifying information and patients were assured that information would not be shared with participating physicians, the study design could have inhibited negative comments about medical care. Conversely, patients who were angry, upset, or disappointed about migraine care could have been motivated to complete the survey.17 Migraine patients who consult physicians are reported to have more severe migraine,18 more comorbidities, decreased quality of life, and to consult significantly more frequently for multiple medical conditions than other patients. These factors indicate a pattern of vulnerability and insecurity about the potential benefits of medical care that have been identified as key to patient dissatisfaction. Our survey return rates could therefore have been biased toward the more dissatisfied patients. The overall level of satisfaction with migraine care from family physicians could be even higher than that reported by our respondents.
The literature on patient dissatisfaction and other poor outcomes of migraine treatment has largely focused on factors related to the condition and its treatment,19–21 or on physician-related factors.7,22 This study indicates that patient-specific factors, particularly migraine-related disability, discontinuation of triptans, and payment for medications are also significantly associated with patient dissatisfaction. The study and the relevant literature do not indicate how these factors relate to satisfaction with migraine treatment or to one another. These patient factors could be consequences of poor satisfaction with care—or could be risk factors, predisposing certain patients to dissatisfaction with treatment. They could each be discrete factors associated with patient dissatisfaction or represent an accumulation of burdens that commonly exist for dissatisfied migraine patients and predispose them to poor outcomes.
Although they are preliminary, our results indicate certain warning signs for patient dissatisfaction with migraine treatment, and possibly increased risk of poor outcomes. Family physicians could use the MIDAS scoring system (available on several web sites including www.achenet.org) to identify patients with high migraine-related disability scores. Information about payment for medication and current use of triptans is also likely to be easily available to family physicians. The discontinuation of triptans is especially interesting as this could provide a warning signal of dissatisfaction with migraine treatment. If alerted to the discontinuation, physicians could intervene to suggest more effective ways to use triptans or to develop an alternative treatment strategy.23
Our hope is that further studies will clarify the subsets of migraine patients who continue to be dissatisfied with management despite advances in therapy.
Acknowledgments
We acknowledge substantial assistance from Lolem Ngong, Terry Ast, Nicole Rogers, and Mary Hursey in the conduct of the study and preparation of this manuscript and the assistance of the physicians of the Kansas Practice Research Network.
Notes
Funding: The study was funded in part by the American Academy of Family Physicians Practice Based Research Network Research Stimulation Grant.
Conflict of interest: none declared.
- Received for publication February 28, 2005.
- Revision received May 20, 2005.
- Accepted for publication May 31, 2005.




{kind=link}