
Abstract
Objective: To understand changes in reasons for visit to primary care in the face of an aging population, growing evidence for proactive preventive and chronic disease services, and the rise of the chronic care model.
Methods: We examined the reason for visits to primary care physicians using the National Ambulatory Medical Care Survey (NAMCS) from 1980–2015.
Results: Among all physicians, the percent of visits for prevention increased from 17% in 2001 to 20% in 2015. Among visits to primary care, most continued to be for acute problems – with the percent of visits for acute illness declining over the past 15 years, after remaining steady for two decades. Preventive care visits increased from 19% in 2001 to 26% in 2015. The percent of primary care visits for chronic conditions declined between 1980 and 2000, and then remained steady, accounting for 30% in 2001 and 31% in 2015.
Conclusions: Growing emphasis on chronic disease management is not reflected in the percent of primary care visits for chronic illness. This study highlights the potential utility of longitudinal data within a historical interpretive frame, while raising questions about the utility of using a main reason for visit to classify complex primary care visits.
- Chronic Disease
- Delivery of Health Care
- Disease Management
- Preventive Health Services
- Primary Care Physicians
- Primary Health Care
Introduction
Recent decades have seen dramatic changes in the practice of medicine.1⇓⇓⇓⇓–6 These changes have been fomented by forces within and outside of health care and many other factors, including response to an aging population, a growing burden of behaviorally mediated and chronic illness, expanding technology, a changing health care workforce, ongoing cost increases, and reforms in the organization and payment for care.
During the past 3 decades, the US Preventive Services Task Force7,8 has systematically provided evidence of the effectiveness of preventive services, and the chronic care model9⇓–11 has assumed prominence in policy and practice circles by calling attention to the rising rates and costs of caring for people with chronic conditions. The past decade has seen growing recognition of the rise in multimorbidity—people living with multiple chronic conditions,12⇓–14 which constitute the majority of visits by adults to primary care.15
The frontline for these health care changes is primary care, which accounts for about half of all outpatient visits,16 and which has been the target of some of the most intensive reform efforts, most notably the patient-centered medical home17⇓–19 but also other payment and practice reform efforts.20⇓–22 Concomitant changes toward an employed physician workforce and growing use of urgent care centers and emergency departments also influence care.
Despite all this change, there has been little longitudinal study of changes in practice over time.23 Therefore, we undertook this study to examine the changes in the major reason for visit to primary care during a 35-year period using the nationally representative National Ambulatory Medical Care Survey (NAMCS), for which reason for visit data have been available since 1980. We hypothesized that we would see a growing percentage of visits for chronic illness and a concomitant reduction in the percentage of visits for acute illness.
Methods
Data from the NAMCS were obtained via the public domain of the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/nchs/ahcd/ahcd_questionnaires.htm) and the Interuniversity Consortium for Political and Social Research (ICPSR) (https://www.icpsr.umich.edu/icpsrweb/). NAMCS was not administered in 1974, 1982 to 1983, and 1986 to 1988, and reason for visit was not collected in 1977 and 1985 to 1996. For these reasons, data points pre-2000 were limited but were included to use all available data. NAMCS is a long-running survey of ambulatory care visits in the United States that uses a multistage probability design to capture information about a representative sample of clinical encounters.24⇓⇓–27 These samples are then weighted to establish national estimates and were weighted within each year using the provided weighting information.
Our primary analyses were focused on major reason for visit, a categorical variable coded from information reported during the visit. Due to variable changes over the years, we made a number of decisions in an effort to provide measures that as consistently as possible assess the same construct over time. For the chronic disease category, we merged flare-up and routine chronic visits, which exhibited similar trends. For the acute visit category, the following variables were combined across years: acute problem (1980, 1981, 1997, 2000 to 2004), new problem (2005 to 2006), new problem (less than 3 months) (2007 to 2015). A preventive visit category became available in 2001. These decisions were made after multiple visualizations of the variable availability and rates across the years.
To provide additional context for interpreting changes in the major reason for visit, we also analyzed a more granular categorical variable reflecting more detailed reasons for visit: 2 preventive categories (general examination and well-baby examination) and 2 common chronic conditions (diabetes mellitus and hypertension).28,29
Our main analyses grouped visits to general practitioners, family physicians, general internists, and general pediatricians. To provide additional context, we examined data for all physicians together and then for each of the 4 primary care specialties separately. To assess if specialists have been seeing more chronic conditions in recent years, we evaluated reason for visit in a subset of specialists available in NAMCS, excluding primary care and all surgical specialties. Although the exact language and specialists captured varied from year to year, they included allergy, cardiology, dermatology, endocrinology, gastroenterology, gynecology, hematology, nephrology, neurology, obstetrics/gynecology, occupational medicine, oncology, ophthalmology, other, otolaryngology, otorhinolaryngology, physical medicine, psychiatry, public health pulmonary, and urology.
Data cleaning and weighting were conducted via SAS version 9, specifically using the PROC SURVEYFREQ procedure with the included strata, cluster, and weights to account for the complex survey design. All main analyses followed proper procedures and ensured adequate sample size for weighting. Data visualization was conducted via R version 3.6.0, using the “tidyverse” package, to depict the percentage of visits in each category over time. For the early years in which NAMCS was not administered every year (1975 to 2000), we conducted analyses at 5-year intervals or during years when data were available. Beginning in 2000, we analyzed data for each year.
Results
In the years 1980, 1981, 1997, and 2000 through 2015, a national total of 16,935,413,908 visits to ambulatory care providers were estimated to have occurred, based on a sample of 661,327 visits reported in NAMCS. Of these, visits to primary care (defined as family medicine, internal medicine, general practice, and pediatrics) represented 256,068 visits weighted to a national total of 8,580,957,687.
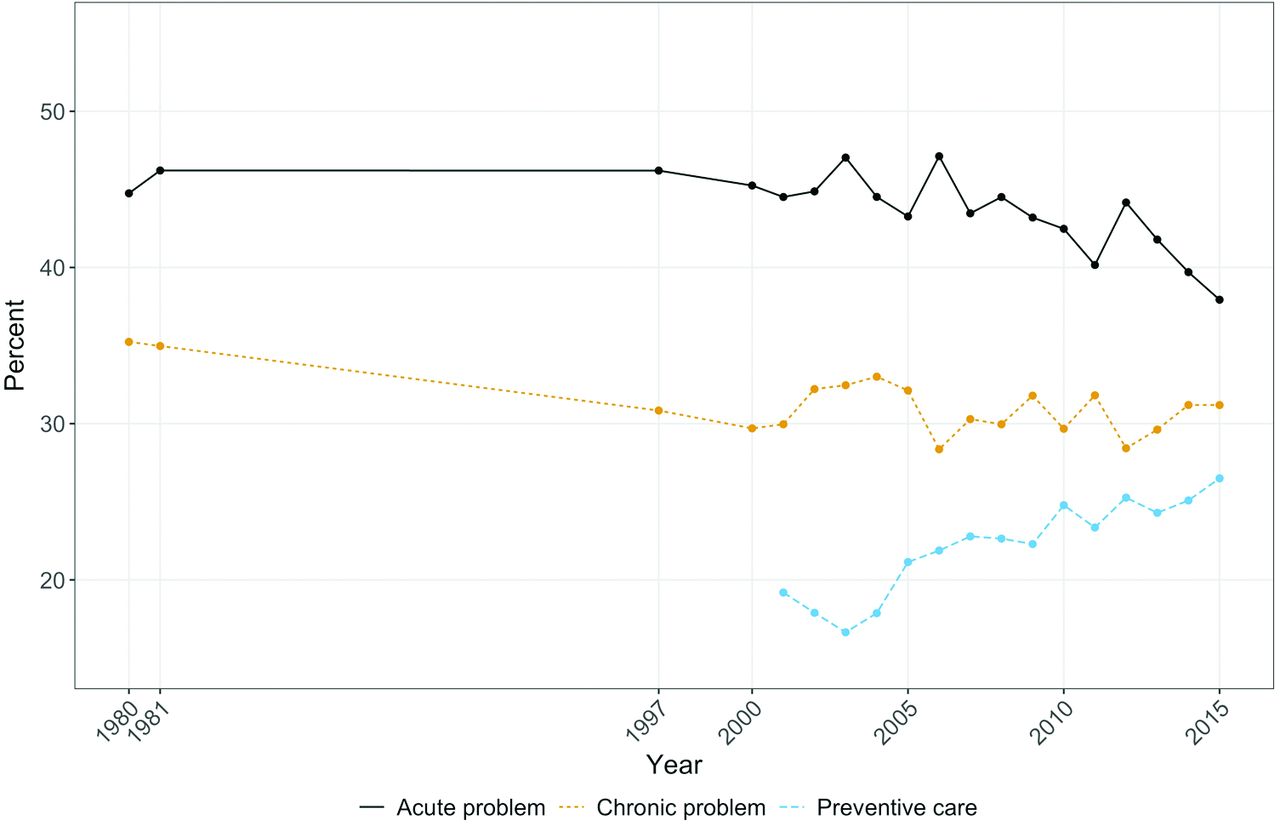
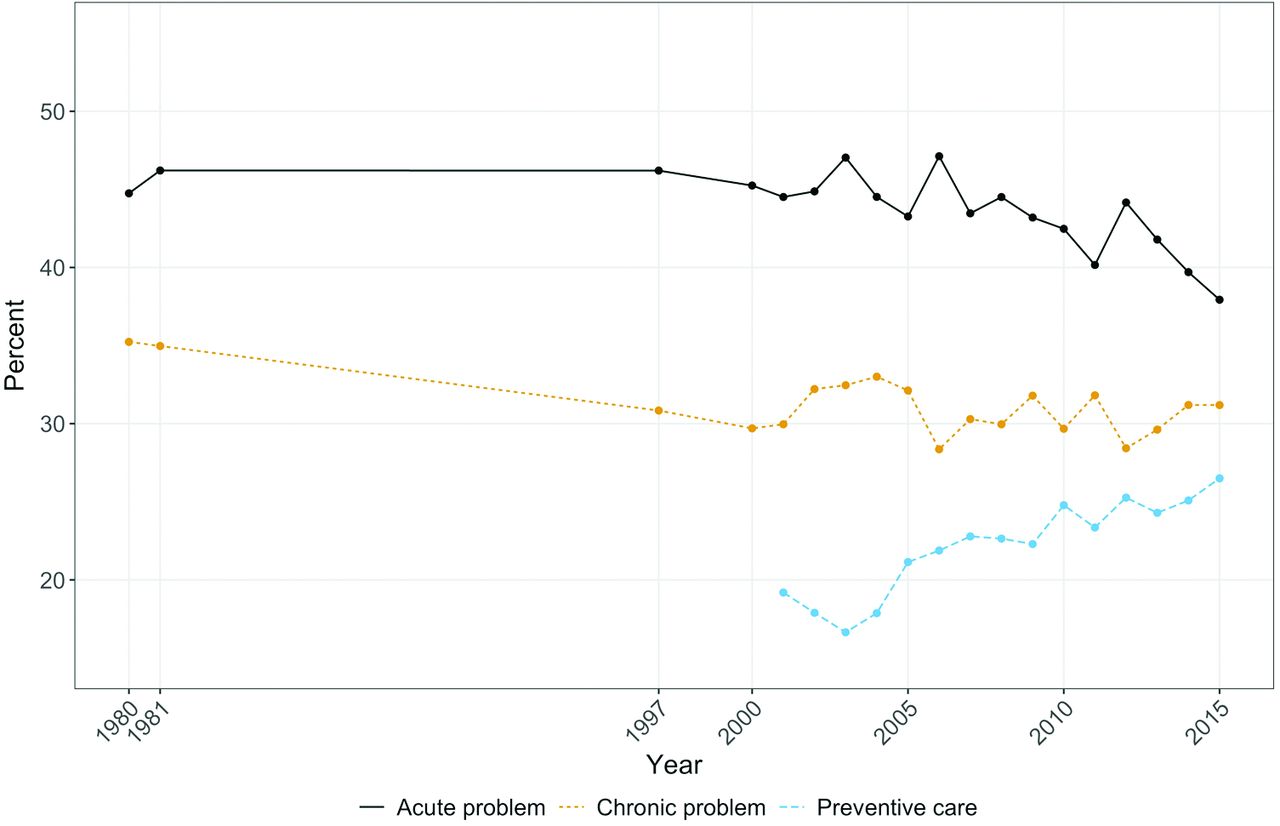
Among all specialties together, as shown in Figure 1, visits for chronic illness are most common and account for a higher percentage of visits since 2000. The percentage of all visits that were for acute illness has declined since 2000, and the percentage of visits for prevention has gone up.

Major reason for visit, all.
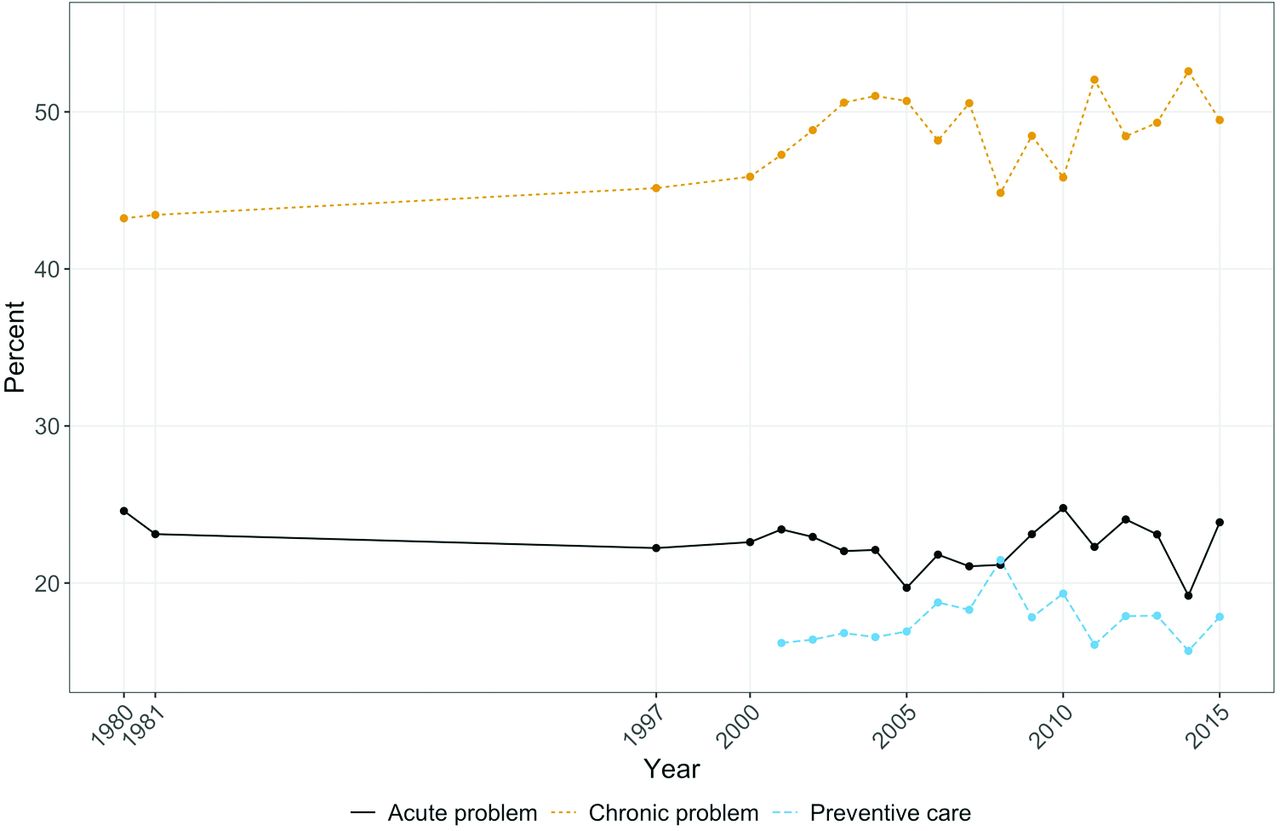
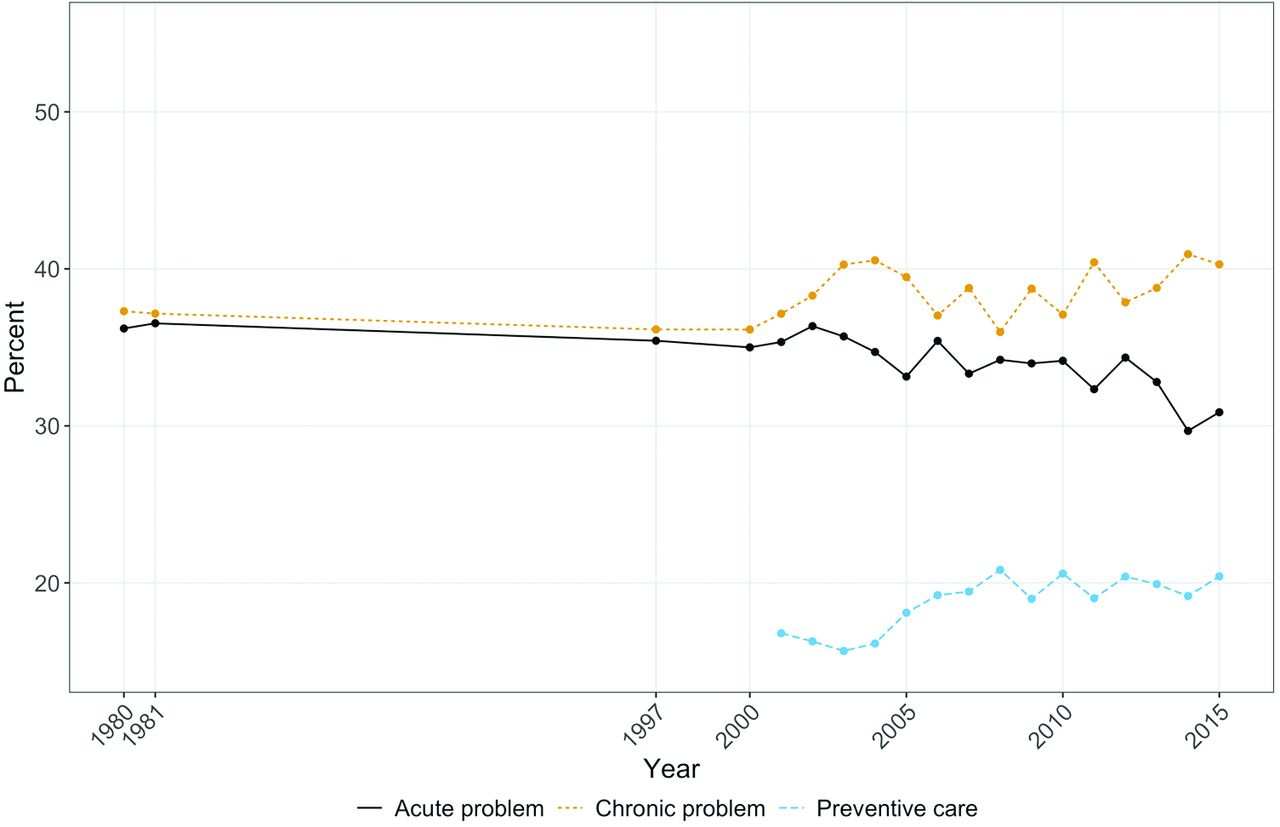
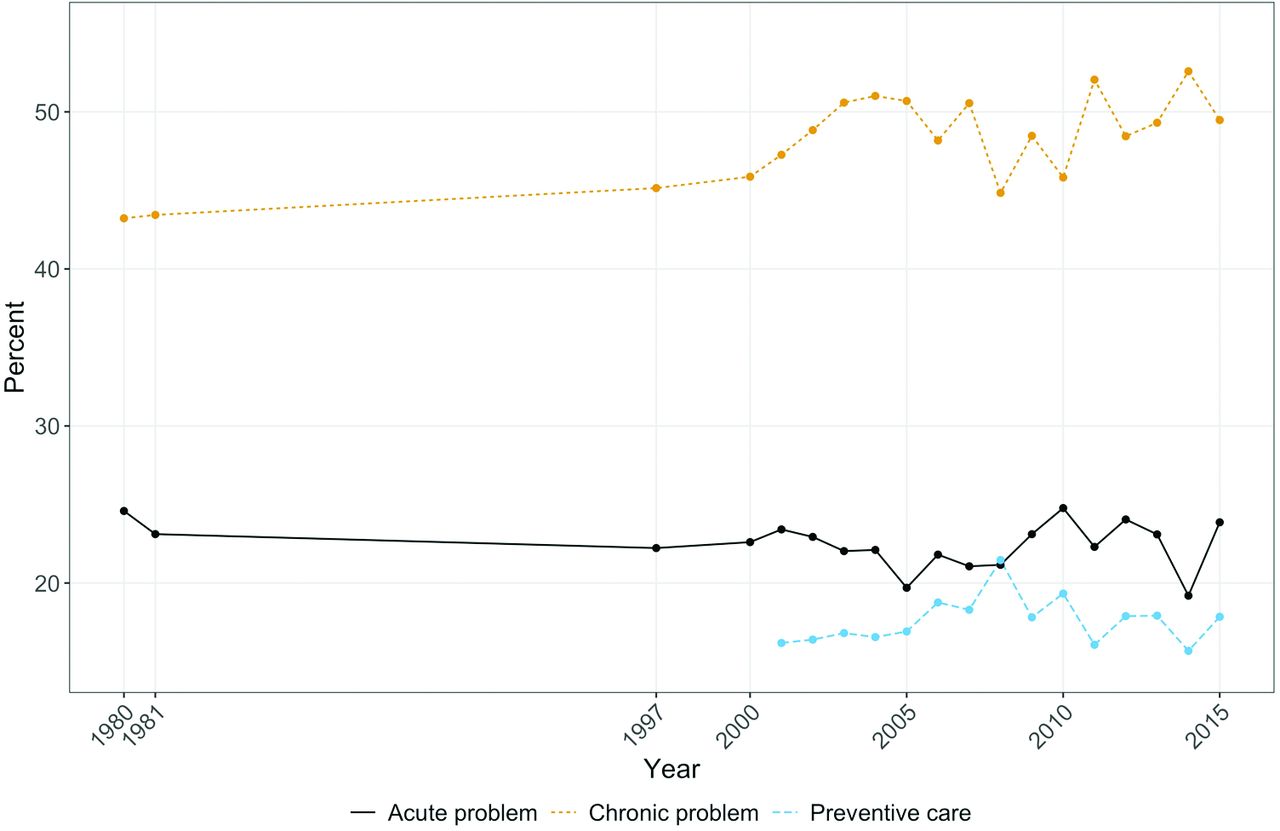
Within primary care (Figure 2), acute illness visits account for the majority of visits and have declined during the past decade. Visits for chronic illness have declined slightly over 35 years, with a small rise 2000 to 2005, then declining to the 2000 base and remaining fairly steady through 2015. Visits for prevention, assessed only since 2001, have been increasing steadily since 2003. Parallel to these changes in primary care, among specialists we saw an overall increase the percentage of visits for chronic illness (Figure 3).
Major reason for visit, primary care.
Major reason for visit, specialists.
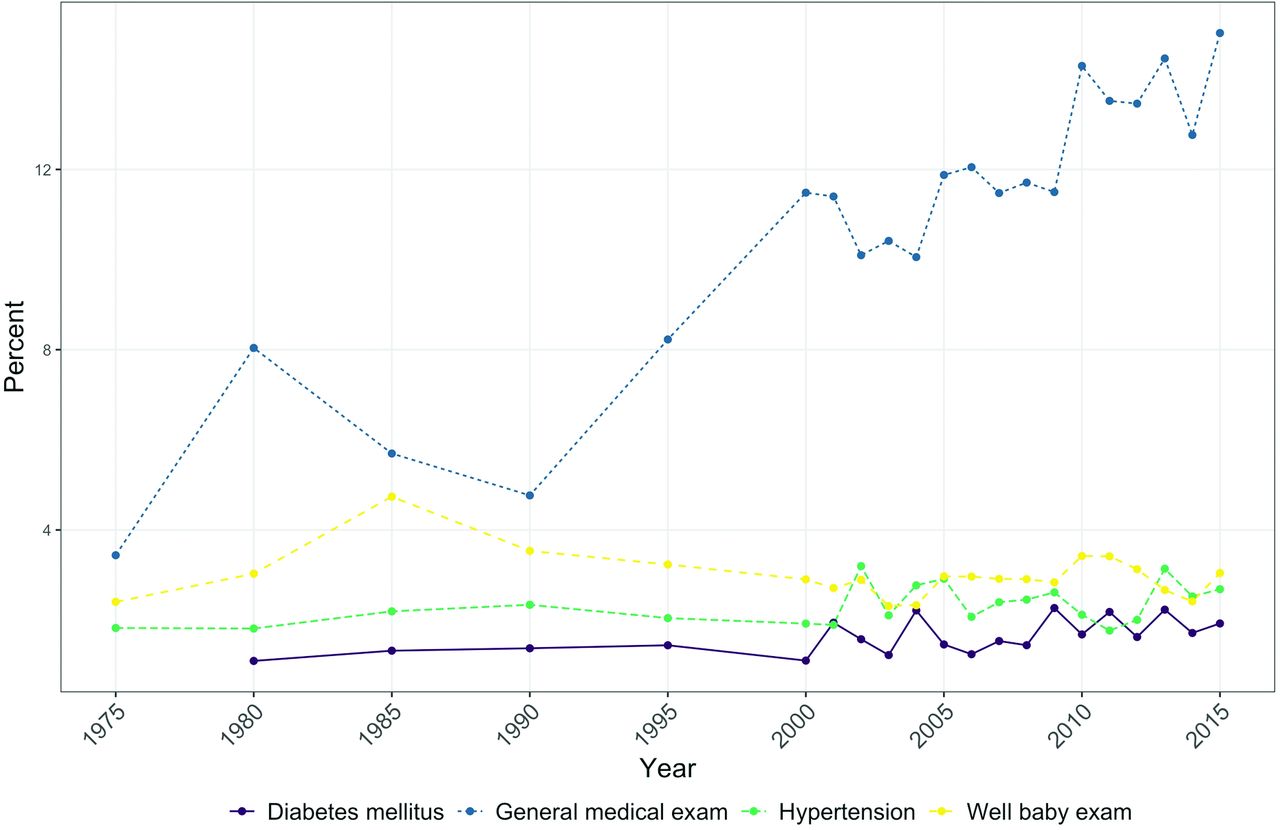
Of the selected more granular reasons for visit, the most striking change over time is the sharp increase in the proportion of visits for general medical examination, amid stable rates for well-baby care and for the 2 chronic conditions examined (Figure 4).
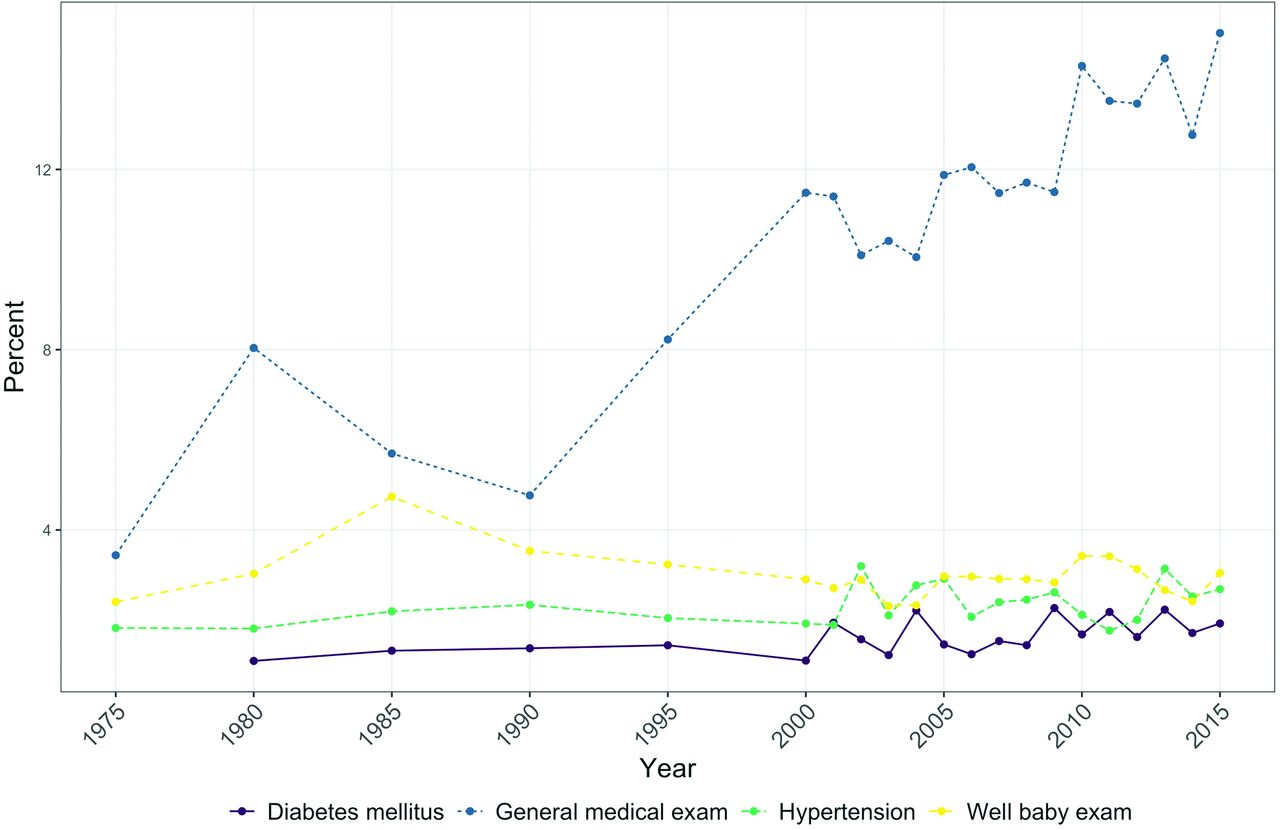
Major reason for visit, selected reasons.
Discussion
We expected to see a large rise in the percentage of visits for chronic illness, due to the aging of the population, the growing burden of chronic disease,30,31 and the rising prominence of the chronic care model.9⇓–11,32 Instead, we observed an increase in the percentage of visits for preventive service delivery. We saw a slight increase in the percentage of visits for chronic illness among all specialties together and a slight decline followed by relative stability since 2000 in primary care. In the past decade, the percentage of visits for acute illness has declined for all specialties together and for primary care.
The rise in the percentage of visits for preventive service delivery may reflect the growing evidence for effective clinical preventive services, the rising prominence of the US Preventive Services Task Force,7,8 and the incorporation of its recommended services in insurance plans.
The surprising lack of increase in the percentage of visits for chronic illness, particularly in primary care where recent reforms emphasize proactive chronic disease care through management programs that aim to reduce visits for these chronic diseases, may reflect the offloading of some of this care to chronic disease management programs not captured in physician visit data.33⇓⇓⇓–37 Despite the growing emphasis on chronic disease management in primary care, it is interesting that the most common reason for visit in primary care is acute illness and across all specialties is chronic illness. The decline in the percentage of visits for acute illness also may reflect growing use of urgent care centers, emergency departments, and telehealth.
During the past 35 years, there has been an expansion in specialty care.38 The rise in the percentage of visits for chronic disease among all physicians may be an indication that a growing percentage of chronic illness is managed in specialty care.38⇓⇓–41 This may be problematic, given the growing rates of people living with multiple chronic conditions for whom a medical home that integrates care is important.42 The growth of specialty and subspecialty fields combined with the fluctuation of primary care workforce suggests that conditions that perhaps were handled solely by primary care physicians are now being referred out and managed by specialists.43,44 Although we were unable to fully confirm this hypothesis, in evaluating the reason for visit among specialists included in the NAMCS, we did observe an increase in reason for visit being chronic condition, suggesting that this is a plausible explanation (Figure 3).
This study underscores the potential utility and challenges of using the longitudinal NAMCS data to assess broad changes in care delivery. The utility relates to the ability to examine trends in nationally representative data whose sampling method has remained reasonably consistent over multiple decades of immense change in US health care. The challenges relate to changes in the wording of questions that limit the ability to examine trends.
The findings also raise concerns about how well common reason for visit classifications fit with the many problems and opportunities addressed in primary care practice and how sensitive the reason for visit categories are to changes in practice. As the chronic disease burden in the United States has increased, it is plausible that these become a routine part of the visit and are not reported by the physician as the major reason for visit.45 This is supported by the observed steady rates of visits where the primary reason was diabetes and hypertension, as we would expect these rates to rise otherwise (Figure 4).
The physician-report measure used in NAMCS has shown generally good concordance with direct observation, but over-reporting of visit duration and under-reporting of behavioral counseling shows the potential for inaccuracy in physician report using the NAMCS form.46 There are many factors that may affect physicians' judgment of what to indicate as the major reason for visit in the NAMCS survey. Certainly, what is paid for and therefore incentivized to be coded for billing purposes likely changed what care is salient to physicians over time. We also do not want to underestimate the cognitive challenge of coming up with a major reason for visit when multimorbidity has been found to be the norm in primary care visits,15 and when the number of problems addressed during a primary care visit has been found to be 2 to 3 based on billing data for the average visit,47,48 5 to 6 for visits by diabetic patients,49 and by a more sensitive direct observation measure, 25 problems addressed during the average diabetes follow-up visit at a high-functioning community health center.50
The findings of this study both highlight changes in reason for visit during the past 35 years and raise questions about the utility of using a physician-reported reason for visit to classify increasingly complex visits. Future work should follow these findings to further assess the changes and evolution of primary care over the years, while concurrently develop methodology that can be used prospectively to more accurately reflect the complexity of care.
Acknowledgments
The authors would like to thank Dr. William L. Miller and Dr. Siran M. Koroukian for their support and assistance through the project, including interpreting initial data and findings.
Notes
This article was externally peer reviewed.
To see this article online, please go to: http://jabfm.org/content/34/2/442.full.
Funding: None.
Conflicts of interest: None declared.
- Received for publication April 13, 2020.
- Revision received July 28, 2020.
- Accepted for publication July 29, 2020.




{kind=link}
{kind=link}
{kind=link}
{kind=link}