
Abstract
Implementation of health information technology (HIT) has become a cornerstone of efforts to improve patient care in primary care practices. However, relatively few publications have explored the impact of HIT on the need for fundamental changes in the primary care delivery process. There is also very little published information about how HIT implementations can drive translation of research findings into practice in primary care. This article describes the process of developing and implementing the Preventive Services Reminder System in the Oklahoma Physicians Resource/Research Network, a practice-based research network, and demonstrates how strategic adoption of HIT led to the re-engineering of practices and to subsequent improvements in delivery of evidence-based preventive services.
Since the 2001 Institute of Medicine report “Crossing the Quality Chasm,”1 primary care practice-based research networks (PBRNs) have been focusing intensely on developing and testing new methods that help the timely implementation of research findings in clinical practice. PBRNs operate in a special position at the interface of classic biomedical research and daily clinical practice, connecting academic research centers with primary care providers. PBRNs are learning communities that provide excellent testing grounds for new ideas and technologies and integrate research and quality improvement into one coherent process.
In 1999, the Agency for Healthcare Research and Quality began to provide support for the growth and development of PBRNs. The initial round of funding required PBRNs to: (1) increase diversity in patient populations; (2) develop 5-year business plans; (3) develop models of translating research into practice; and (4) develop ways to routinely collect study-specific data in an electronic manner. Several PBRNs set out to meet these challenges, including the Oklahoma Physicians Resource/Research Network (OKPRN). The network was established in 1994 as a collaborative project of the Oklahoma Academy of Family Physicians and the University of Oklahoma Department of Family and Preventive Medicine in Oklahoma City.
Since 2001, OKPRN has responded to the challenge of TRIP (translating research into practice) and enrolled a wide variety of primary care practices in the network (eg, residency clinics, Native American providers, community health centers; more than 230 clinicians), became a 501c(6) nonprofit entity that is separate from the university, developed and implemented the Practice Enhancement Assistant (PEA) program, and pioneered HIT solutions that clinicians or other support staff could use with every patient. Various OKPRN projects that included HIT implementations demonstrated that translation of research findings into practice can be not only facilitated but can actually be driven by system-level adoption of information technology (IT).2
The Preventive Services Reminder System (PSRS)
OKPRN clinicians indicated that it would be useful for their practices if their staff could more easily determine needed immunizations for children and report to the Oklahoma State Department of Health immunization registry. Early in the process, OKPRN clinicians realized that they could expand this concept by including all primary and secondary preventive services. We therefore set out to create an IT application that would provide individualized prompts and reminders for primary and secondary preventive services for both children and adults while collecting and registering encounter-level demographics and risk factor data. This information could then be used for planning research projects.
Because personal digital assistants were significantly less expensive and more mobile than other computers, the prototype of the PSRS was developed for networked Palm handheld devices. The personal digital assistant prompted the nurse to ask the patient about past preventive services and current risk factors and provided a list of evidence-based recommendations on services due for the patient at that visit. A custom-designed sophisticated algorithm processed patient demographics, medical history, risk factors, and contraindications from the PSRS registry and returned an evidence-based list of services tailored to the patient. OKPRN also worked closely with the Oklahoma State Department of Health to develop an HL7 (Health Level Seven clinical and administrative data standard) interface to the state immunization database. The Oklahoma Medicaid program subsequently provided a series of contracts to continue to develop and test the system.
In the next phase, PSRS evolved into a secure open-source Java Web application that greatly expanded the functions of the system and facilitated utilization of the technology by a larger group of clinicians. This scalable system is cross-platform and available via a Web browser from most computers and handheld devices. Additional functions included automated generation of recommendation-specific patient education materials and patient reports, electronic chart audits for patient recalls, 3-year customized prevention plan, more personalized recommendations, and electronic patient record transfer from the state immunization registry.
Options in Implementing Steps of the PSRS Process
PSRS can return a simple age and gender-based recommendation list if no other information is available. However, the system can deliver a patient- and visit-specific list of suggested services when patient risk factors, contraindications, and vaccine-related allergy information are also supplied. Personalization of recommendations happens in a 3-step process within the PSRS algorithm. First, a generalized list is created using only demographic information, then personal risks and contraindications are factored in, and finally, recommendations are seasonalized (eg, flu shots are suggested only during fall and winter, sun exposure advice only in spring and summer, etc). The more information PSRS receives, the more accurate and personalized feedback it can provide.
Risk factors and contraindication information must get into PSRS either via manual entry or electronic data transfer from medical records. As an ideal solution, a patient portal to capture these data in the system is planned. However, PSRS proved to be quite flexible in accommodating different ways of collecting risk and contraindication information by the staff. Options include: (1) patient completes a 1-page printed survey at least once a year; (2) the staff interviews the patient briefly at the visit and enters information directly into PSRS; or (3) staff circles items on a preprinted patient report for consequent data entry. The PSRS algorithm immediately generates a new recommendation list upon updating the patient’s record.
Tailored patient reports can be run for the present and future time periods as well. In addition, a 3-year default wellness plan can also be generated for adults assuming that suggested services are provided within a year for each 1-year period. The default plan is generated based on US Preventive Services Task Force, Advisory Committee on Immunization Practices, and American Academy of Family Physicians guidelines and can be accepted as is or can be negotiated with the patient. The final plan is then entered into the task management component of PSRS to coordinate care at future visits.
Results of PSRS Implementation Pilot Studies
The clinical effectiveness and implementation cost of PSRS have been tested in 2 separate pilot studies. In the first study, patient records (N = 549) were analyzed from a total of 6 primary care practices assigned to control and intervention groups that were matched deliberately to examine the level of documentation and delivery of 4 childhood immunizations (fourth dose of diphtheria, tetanus, and pertussis [DTaP#4], third dose of hepatitis B [HepB#3], pneumococcal, and measles, mumps, and rubella [MMR#1]) and 3 secondary preventive services (smoking status, smoking counseling, and adult pneumococcal). Patients in this study represented a diverse population from various family practices (private, academic, and community). Apart from childhood pneumococcal vaccinations, documentation and delivery of these services increased significantly (P < .02) after a 6-month implementation period (Table 1).
Preventive Services Reminder System (PSRS) Study No. 1: Coverage Rates of Preventive Services before and after PSRS Implementation in Intervention and Control Practices
In the second study, Medicaid patient records (N = 1110) from 12 matched control and intervention practices were audited before and after a 6-month implementation period. Documentation and delivery of 6 childhood immunizations, well child visits, 3 adult immunizations, and 4 secondary preventive services were analyzed. With the exception of the third dose of childhood pneumococcal immunization and some adult vaccinations (eg, flu shot), implementation of PSRS resulted in a remarkable increase in both documentation and delivery of most services (P < .05) compared with the control group in which only performance feedback was given to the provider (Table 2). The patient group was representative of a variety of primary care practices including private, academic, Native American, and community clinics.
Preventive Services Reminder System (PSRS) Study No. 2: Coverage Rates of Preventive Services before and after PSRS Implementation in Intervention and Control Practices
It is evident from Table 2 that the control group has a higher baseline than the intervention group. The most likely explanation is that the groups were not randomized and practices with a better baseline quality of care were selected inadvertently. However, results suggest that practices with suboptimal performance can be brought up to the level of high performers with the implementation of PSRS.
Approximately 50% of the practices involved in these studies chose to continue to use PSRS after the studies were finished. Long-term PSRS users can be characterized by a high level of interest in preventive medicine, quality improvement, and IT. They also represent a group of motivated clinicians with more active involvement in OKPRN projects, who continuously strive to improve their practices and the patient care they provide. In the 2 pilot PSRS studies, we did not determine how many patients were actually eligible for certain services and what portion of these patients actually received recommended services. A current project that examines a new model of care delivery with PSRS will provide this information.
We also conducted a detailed implementation and maintenance cost analysis through time-motion studies in 2 representative intervention clinics. These studies suggested that the average cost of installing and implementing PSRS was approximately $550 per clinic assuming that basic IT infrastructure and support were already in place in participating practices. Depending on the individual implementation model and particularly physician time spent with PSRS operation, daily maintenance cost of the system was approximately $2.15 to $3.50 per patient visit. This amount includes all material, logistic, and personal costs.
Lessons Learned from the PSRS Project
Implementation of PSRS in a wide range of primary care practices taught us several lessons. We discovered that HIT cannot be used alone as a silver-bullet solution for improving care delivery. In fact, HIT implementations may often fail because they may just simply automate the existing inefficient practice workflow. This conclusion is especially important for delivery of preventive services. On the other hand, IT seems to work most effectively when practice workflow is re-engineered to support improved patient care services and the computerized system is organically integrated into the improved process.
The PSRS project underscored 3 key steps to improve delivery of preventive services in primary care practices: (1) clinicians in the practice must communicate the importance of preventive services to staff and patients; (2) responsibilities must be reassigned to practice team members other than the physician; and (3) a rigorous task management system must be put into place to coordinate activities and handle information flow during and between patient visits.
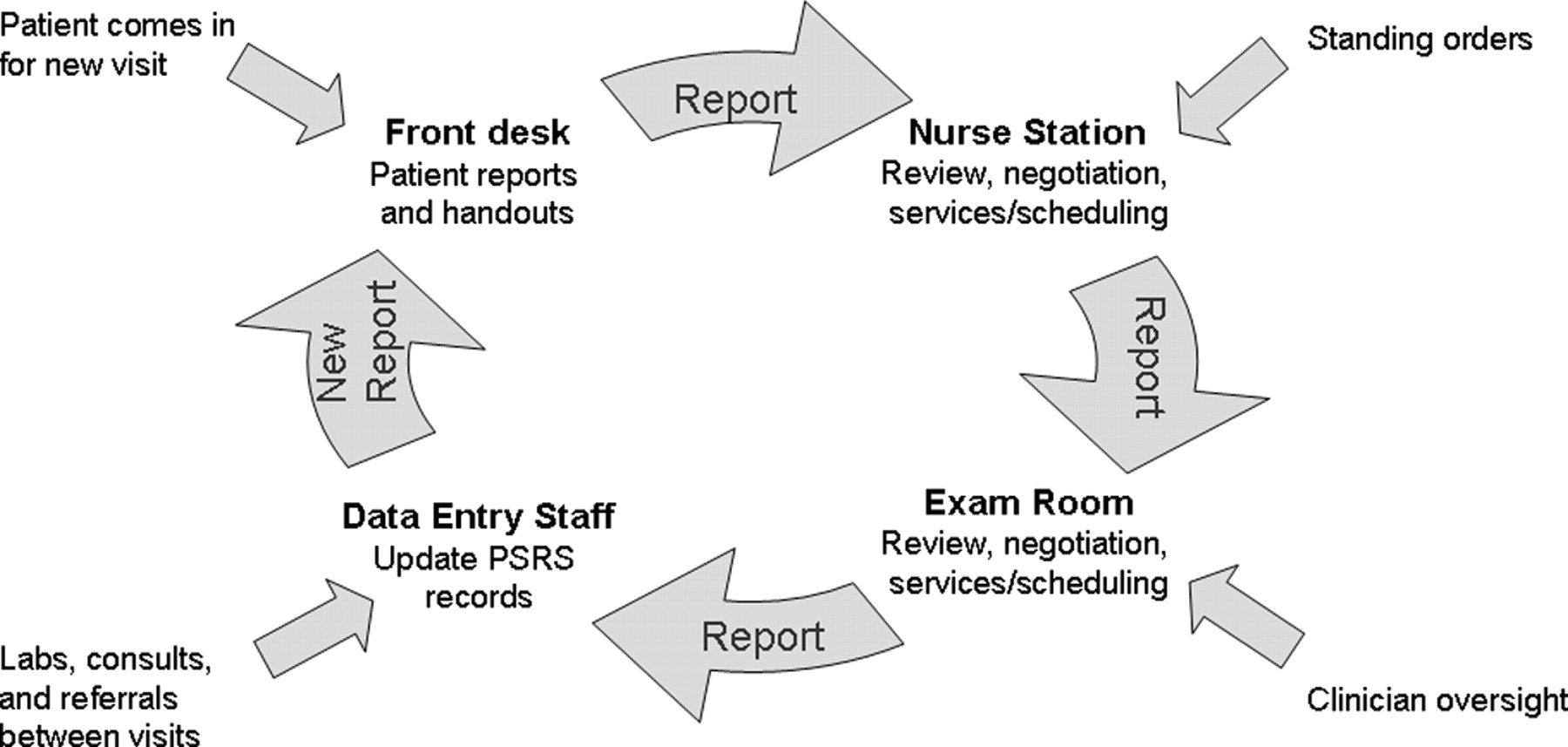
A PSRS workflow example is shown in Figure 1. In this case, PSRS was incorporated into paper-based practices in a large academic family medicine residency clinic, where the environment allowed for only small changes in the existing workflow. Note that tasks associated with PSRS are assigned to all members of the clinic team that work together in a coordinated manner. Nurse empowerment in the form of standing orders was a critical step in the process. This approach significantly improved the delivery of preventive services but left the busy nursing and data management staff with additional work to do with each patient.

Preventive Services Reminder System (PSRS) workflow in a paper-based large academic family residency practice. PSRS was incorporated into the existing office workflow, and new tasks associated with PSRS were assigned to members of the clinic team. Nurse empowerment in the form of standing orders was a critical step in the process. Although delivery of preventive services significantly improved, PSRS increased the staff’s workload.
The next example demonstrates PSRS workflow tailored to a middle-sized suburban family practice (Figure 2). In this practice, a technology-savvy clinician took the initiative and decided to be closely involved in the process. At each visit he reviewed an electronic or paper report on evidence-based recommendations and teamed with the nurse to deliver or schedule services. He also updated PSRS records during or immediately after the visit. However, clinic staff was also available as needed to keep the system up-to-date. Again, PSRS proved to be effective but resulted in additional work for the clinician and staff.
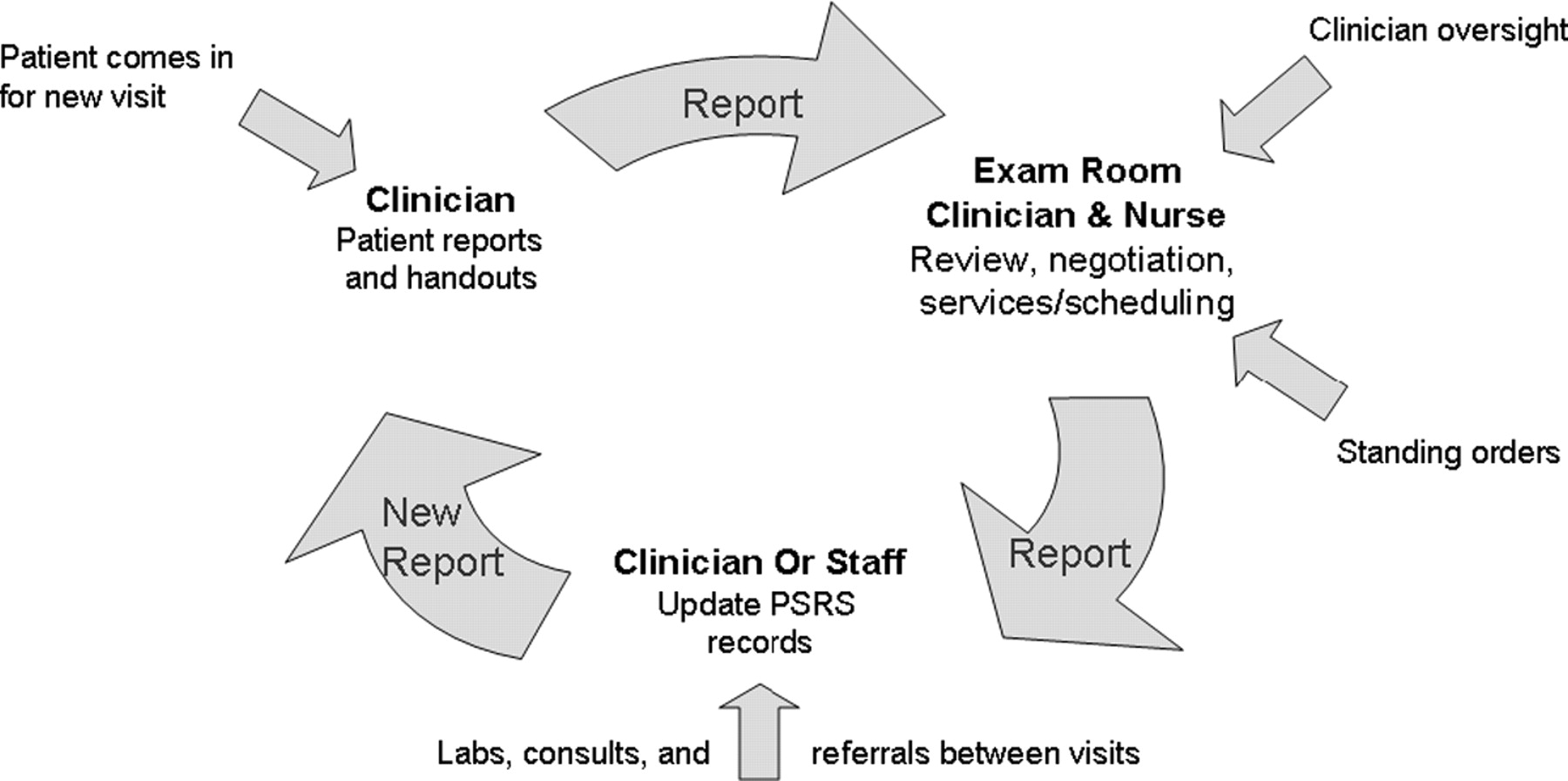
Preventive Services Reminder System (PSRS) workflow in a middle-sized suburban family practice. A physician-centered protocol was developed to implement PSRS. The nurse and occasionally the office staff assisted the physician to deliver and document services. PSRS was effective but resulted in additional work for the clinician and the staff.
Practices implementing a model similar to the first 2 examples reported that despite their achievements by using PSRS, a significant obstacle remained in providing the best preventive care they thought possible. It is not easy to address preventive medicine in the current structure of primary care. Clinicians must “shift gears” during a regular patient visit between providing acute and preventive care. In addition, it has been estimated that it would take approximately 7 hours a day for a primary care clinician to comply with all current preventive guidelines for all their patients (also referred to as the “7 hour problem”3). These considerations question the feasibility of simply “piggy-backing” comprehensive and systematic prevention programs into existing delivery models and suggest that a completely new approach is needed.
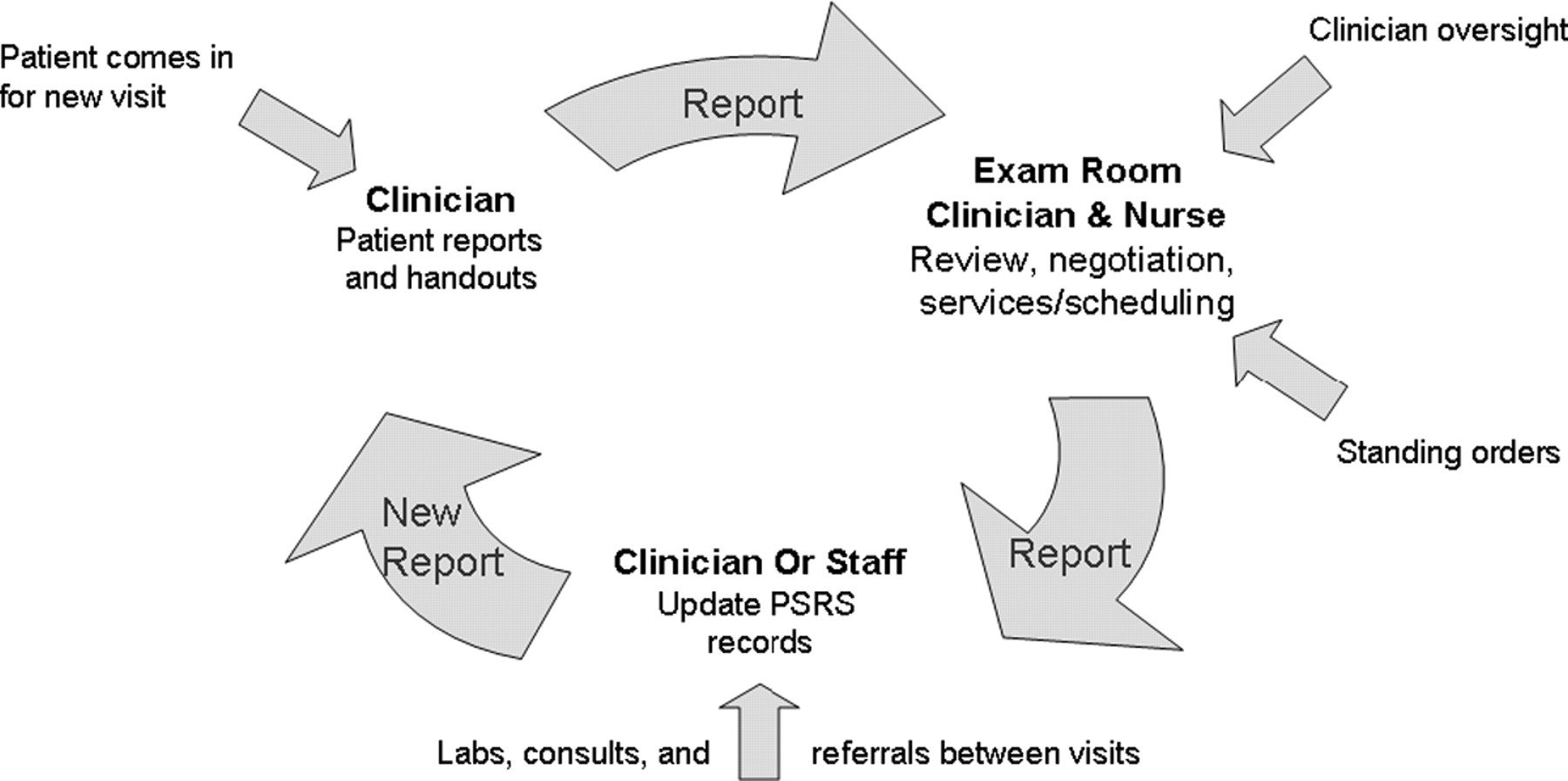
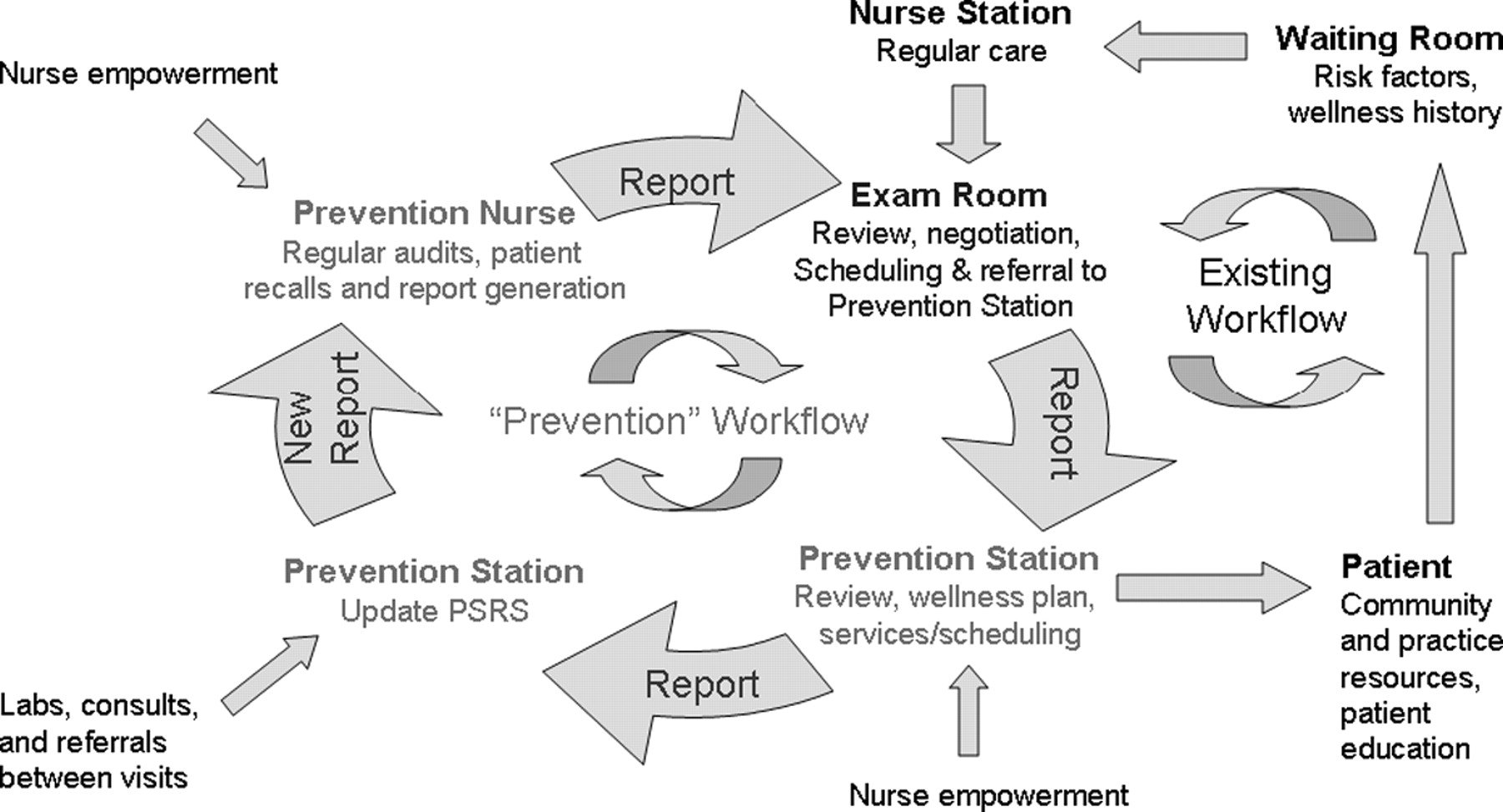
The third example shows a unique model of implementing PSRS in a rural solo physician practice (Figure 3). Based on the above considerations, the clinician set up a prevention station in his clinic with the help of a full-time dedicated prevention/wellness nurse. The majority of the preventive service delivery process was separated from the regular daily workflow of the clinic and managed by the wellness nurse in a coordinated fashion but independently from the clinic staff. The nurse proactively scanned patient records in PSRS, ran audits, recalled patients based on system prompts, reviewed recommendations, negotiated a wellness plan with the patient, and delivered services based on standing orders under physician oversight before or after regular visits or at separate nurse visits. She also connected patients to community resources and provided patient education.

Preventive Services Reminder System (PSRS) workflow in a rural solo physician practice. A prevention station was established with the help of a full-time dedicated prevention/wellness nurse. Preventive services were separated from the regular daily workflow and managed by the wellness nurse with the help of PSRS. The nurse proactively ran electronic chart audits, recalled patients, negotiated a wellness plan, and delivered services based on standing orders.
This approach successfully combined the effectiveness of PSRS with a significantly reduced burden on clinic staff compared with the first 2 implementation examples. The nurse was able to focus completely on prevention and provided effective, timely, and systematic care without disrupting the regular visit cycle. This ongoing project has been funded by an academic grant that paid one half of the nurse’s salary to test the economic viability of the wellness station model. Financial data are being analyzed in the practice, and although there is no conclusive evidence yet, preliminary results suggest that it is probably possible to recoup the expenses of a wellness nurse, or possibly even generate a modest revenue, if the nurse also provides a wider range of billable evidence-based services, including hearing and vision tests, spirometry, and EKG. However, more research is needed to provide a conclusive and generalizable answer.
Caveats
Some OKPRN practices have not been successful in taking full advantage of PSRS. Practices that are unstable, in permanent turmoil, or unable to change cannot readily improve system-level processes or implement new technology. Practices could not improve preventive service delivery in a coherent and systematic manner without forming a team that regularly reviews the care delivery process and adjusts clinic operations based on staff feedback and audit results (eg, via Plan-Do-Study-Act cycles4). It was also crucial for each member of the practice team to have a sufficient level of initiative and commitment to change the way they approach preventive care. In rare instances, some practices lacked a basic IT infrastructure to operate PSRS. Finally, clinician members of large commercially owned medical entities often faced the challenge of an excessive review process by multiple layers of their corporate bureaucracy. In some cases, the corporate leadership had implemented internal quality improvement measures and had few incentives to work with OKPRN on quality improvement activities.
Obstacles and Solutions
The most significant obstacle in the process of practice-redesign to implement PSRS was the existence of a physician-centered, “traditional” care delivery system that revolved around the quantity of patients seen per day. A hectic office workflow with extremely short visit times, a high volume of patients, and a system that lacked an effective team-based approach had to be turned into a patient- and quality-centered, office team-driven system in which there is a continuous dialogue about how to improve the quality of care, which in turn facilitates incremental improvements. This process often involves several stages of change in the way office teams are structured and provide patient care. Task reassignment, nurse and staff empowerment, and workflow optimization proved to be critical to achieve success.
Most importantly, external help provided by Practice Enhancement Assistants (PEAs), who are specifically trained to facilitate practice re-engineering and improve office systems, was necessary to bring about and sustain improvements. Five full-time equivalent PEAs regularly spend a half day in each clinic from a group of OKPRN practices to work on research and quality improvement projects. They become members of the practice team and bring in a variety of resources to assist the practice. It is likely that most practices could not have gone through the process to implement PSRS successfully without systematic personal assistance from the PEAs. See Nagykaldi et al5,6 for additional information on practice facilitation and the work of PEAs in the United States.
An Advanced Preventive Services Delivery Model
Based on clinician requests and the evolution of decision support systems, we are now considering the incorporation of disease-specific (tertiary) preventive interventions into the algorithm. This addition would involve integration of specific diseases as risk factors along with the recommendations from the relevant disease-specific clinical practice guidelines. However, when we also include a vast array of new risk information from genetic testing, clinicians may be overwhelmed by an excessive list of new recommendations. Therefore, evidence-based prioritization of recommendations becomes necessary. Prioritization could be based on the intervention’s impact on outcomes, including life expectancy or quality-adjusted life expectancy, quality of life, disability, and size of the expected clinical effect. The clinician then could start with services that would be most likely to provide benefit for the patient and streamline a long list of tasks based on clinical evidence.
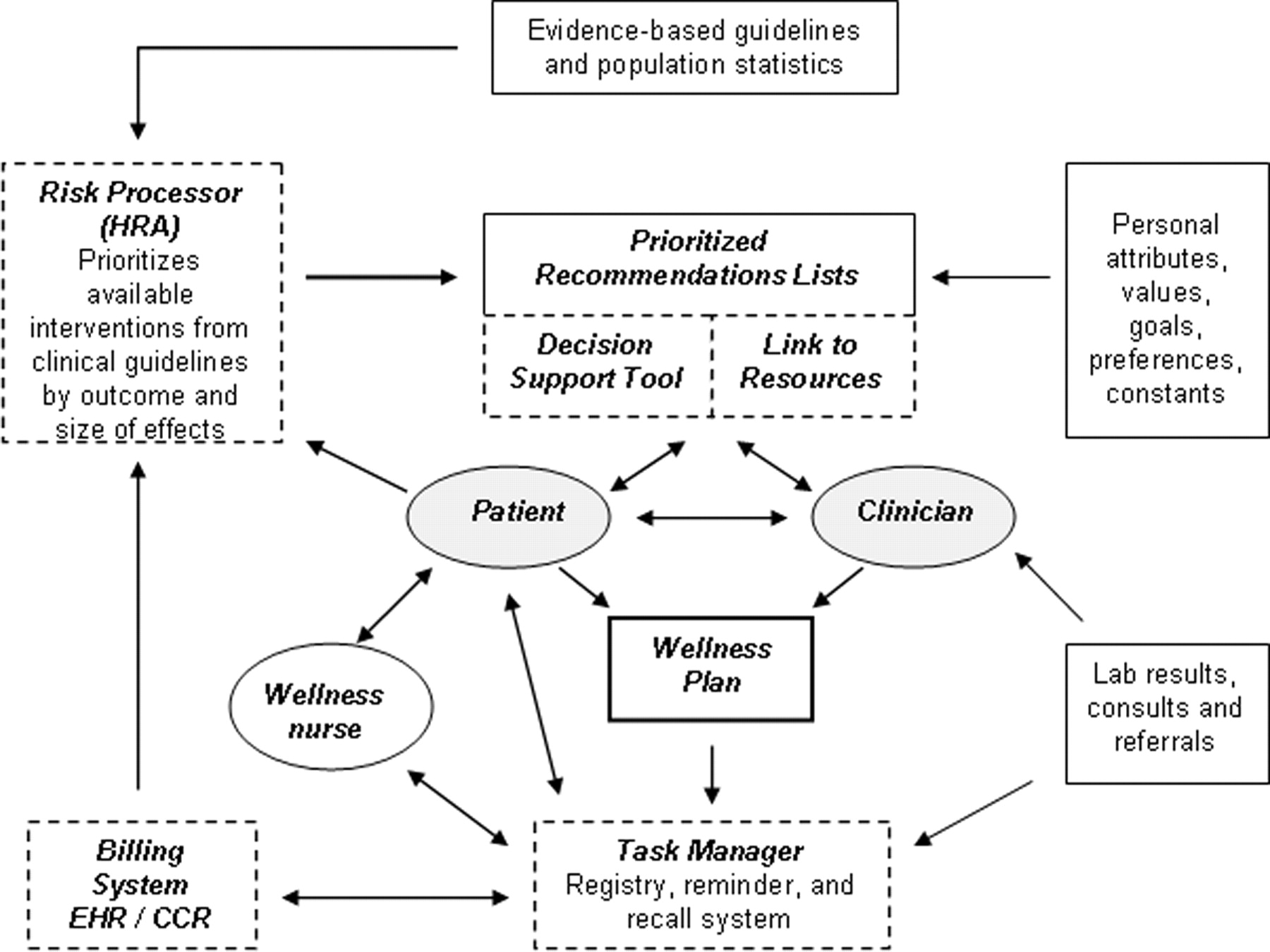
Figure 4 demonstrates an advanced prevention model using a health risk appraisal (HRA) tool connected to a risk processor engine. This novel approach allows for considering diseases and various health conditions as risk factors for adverse outcomes that the provider-patient team wants to prevent and therefore fully and natively integrates preventive medicine into the primary care delivery process.
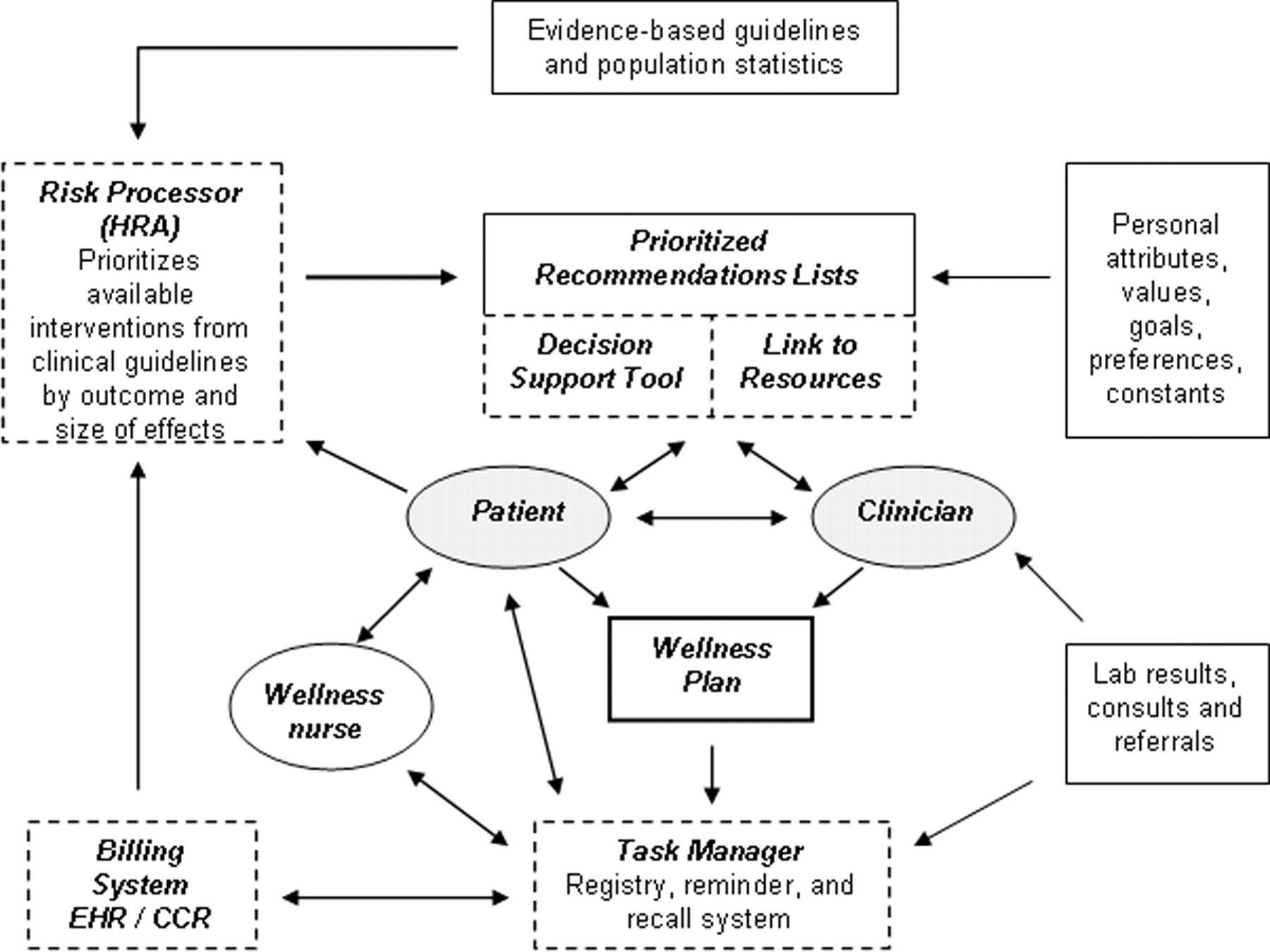
Advanced preventive services delivery model based on a health risk appraisal-driven prioritization of tasks. The risk engine generates an evidence-based prioritized list of recommendations that is turned into a wellness plan negotiated with the patient. The plan is then entered into a task management system and a wellness nurse carries out the plan in a timely manner. HRA, health risk appraisal; EHR, electronic health record; CCR, Continuity of Care Record.
Based on clinical guidelines and population statistics, patient health records, personal risk information, and direct patient input, the risk engine generates an evidence-based prioritized list of recommendations that is turned into a negotiated wellness plan. The plan is then entered into a registry/reminder/recall and task management system (PSRS), and a dedicated provider (eg, wellness nurse) becomes responsible for making sure that services are delivered in a timely manner. The clinician oversees and facilitates the process, but he/she is not directly involved in all the steps of carrying out the plan. Not surprisingly, this advanced model has a lot in common with the concept of the Chronic Care Model (CCM).7 The CCM similarly emphasizes the broad concept of connections to community resources, self-management support, delivery system redesign, clinical decision support, HIT, and interactive team-based care. However, CCM does not provide specific ideas on system-level changes for individual practices that are necessary to bring about these functional and clinical outcomes.
PSRS And Other Electronic Systems
To function seamlessly in an increasingly electronic environment in which most electronic health records (EHRs) still do not reach a desirable level of sophistication in clinical decision support, it has been vital to interface PSRS with other clinical databases. Most importantly, design of an HL7 connection to the state immunization registry (the Oklahoma Statewide Immunization Information System [OSIIS]) is under way whereas CCR (Continuity of Care Record) and OSIIS data can already be transferred into PSRS electronically. Patient demographics and medical service history data can also be exchanged in a batched format between various billing systems and PSRS. However, proprietary technology and limited access to commercial databases often makes this process challenging. On the other hand, our experience with PSRS showed that complete electronic integration of a recall/reminder and task management system may not be necessary. A preventive service database can feasibly coexist with other clinical HIT resources provided that billing information for preventive services is finally integrated within the clinic. Ideally, these functions could be incorporated into redesigned EHRs that support a workflow optimized for preventive care.
Conclusions
Careful and systematic implementation of HIT can drive practice redesign that leads to improved care delivery and bridging the “quality chasm” in primary care. HIT should not replicate inefficient and ineffective systems but should help providers rethink and change their practices, focusing on models and methods that foster a team-based patient- and outcome-centered approach. Advanced task management and task-oriented mentality is crucial to sustain improvements in preventive care. HIT implementation and team-based assignment of tasks via nurse and staff empowerment must go hand-in-hand to achieve the maximum benefit of an electronic system. Technology in the context of structural improvements is an excellent way of translating research into practice. Finally, EHRs must be redesigned to incorporate sophisticated and evidence-based decision support, task management, and prompt/recall/reminder functions.
Notes
This article was externally peer-reviewed.
Support: The development and testing of the PSRS (PSRS Phase I–IV studies) were supported by research grants and contracts with the Oklahoma Health Care Authority (20030073R1), Agency for Healthcare Research and Quality (R21HS013557 and R21HS014850), and Oklahoma Center for the Advancement of Science and Technology (HR 05 to 083).
Previous presentation: This article is based on a presentation made at the American Academy of Family Physicians National Research Network 2006 Convocation of Practices and Networks, Dallas, TX, February 23–26, 2006.
Conflict of interest: none declared.
- Received for publication May 19, 2006.
- Revision received August 28, 2006.
- Accepted for publication August 30, 2006.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- Improving Pneumococcal Vaccination Rates in Rheumatology Patients by Using Best Practice Alerts in the Electronic Health Records
- A Taxonomy for External Support for Practice Transformation
- A Sustainable Model for Preventive Services in Rural Counties: The Healthier Together Study
- An Innovative Community-based Model for Improving Preventive Care in Rural Counties
- Accelerated Adoption of Advanced Health Information Technology in Beacon Community Health Centers
- Preventing the Voltage Drop: Keeping Practice-based Research Network (PBRN) Practices Engaged in Studies
- A Model for the Electronic Support of Practice-Based Research Networks
- Impact of a Wellness Portal on the Delivery of Patient-Centered Preventive Care
- Implementation of Evidence-Based Preventive Services Delivery Processes in Primary Care: An Oklahoma Physicians Resource/Research Network (OKPRN) Study