The Quality and Outcomes Framework—where next?
BMJ 2013; 346 doi: https://doi.org/10.1136/bmj.f659 (Published 07 February 2013) Cite this as: BMJ 2013;346:f659
- 1Lea Vale Medical Group, Luton, UK
- 2Department of Public Health and Primary Care, Institute of Public Health, University of Cambridge, Cambridge CB2 2SR, UK
- 3Norwich Medical School, Faculty of Medicine and Health Sciences, University of East Anglia, Norwich, UK
- Correspondence to: S Gillam sjg67{at}medschl.cam.ac.uk
- Accepted 8 January 2013
Introduced in 2004, the UK Quality and Outcomes Framework (QOF) is the most comprehensive national primary care pay for performance scheme in the world.1 It includes financial incentives and information technology (computerised prompts and decision support) to achieve evidence based quality targets. The inducements are substantial, with a maximum of 1000 points available to practices, and an average payment per practice in 2011-12 of £130 (€150; $205) for each point achieved.2 Over half of these points are allocated to clinical indicators, which currently cover 22 chronic conditions, and the remainder to organisational indicators (box).
Domains of Quality and Outcomes Framework
Clinical
Secondary prevention of coronary heart disease
Cardiovascular disease: primary prevention
Heart failure
Stroke and transient ischaemic attack
Hypertension
Diabetes mellitus
Chronic obstructive pulmonary disease
Epilepsy
Hypothyroidism
Cancer
Palliative care
Mental health
Asthma
Dementia
Depression
Chronic kidney disease
Atrial fibrillation
Obesity
Learning disabilities
Smoking
Peripheral arterial disease
Osteoporosis
Organisational
Records and information
Information for patients
Education and training
Practice management
Medicines management
Quality and productivity
Patient experience
Length of consultation
Additional services
Cervical screening
Child health surveillance
Maternity services
Contraception
The QOF was designed to improve the management of chronic disease by rewarding practices for delivering interventions linked to improved health outcomes for heart disease, diabetes, and other major scourges. The money to implement the scheme was intended to raise pay for general practices. Subsequently, proposed changes have been agreed by the General Practitioners Committee of the British Medical Association and the Department of Health. Negotiations over revisions to the General Medical Services contract in England having stalled, the Department of Health recently announced that it intends to impose changes to the QOF in 2013-14. These include:
Raising the upper threshold for the percentage of patients receiving the relevant interventions in order to achieve maximum points, and therefore payment
Discontinuing the organisational domain
Implementing the National Institute for Health and Clinical Excellence (NICE) recommendations for new clinical indicators.3
The effects of the QOF on quality of care have generated considerable debate. Do payments reflect better recording rather than better care, and do practices achieve high scores by “gaming” the system?4 5 Drawing firm conclusions about the effects of the QOF is difficult because it was implemented across the UK, leaving no comparator practices. Improved processes (such as treating hypertension) may not always translate into improved outcomes (such as stroke prevention) because of other powerful influences on outcomes such as differential access to care, non-modifiable risk factors (genetic), or patterns of comorbidity. Nevertheless, the debate is now being informed by an accumulating body of research into both the benefits and costs of the QOF.6 We consider the implications of the government’s proposed changes, whether the QOF is likely to have improved the population’s health, and how its effect could be augmented.
How the QOF is constructed
Clinical areas are prioritised by an advisory committee at NICE and then undergo a formal consensus procedure followed by piloting in representative practices across England. The architects of this process have described the concept of “QOFability”: reasons why certain issues can or cannot be made into QOF indicators.7 These include the prevalence of the clinical condition, the accuracy of data extraction from general practice clinical systems, the clarity of diagnosis, the relevance of incentivised actions, how directly change can be attributed to primary care staff, and consideration of any possible unintended consequences of introducing the proposed indicator.
The process is transparent, systematic, and robust—an impressive testimony to the experience and dedication of NICE and various associated institutions. It has also been separated from the thorny process of contractual renegotiation. However, this elaborate filtering process inevitably prioritises straightforward technical and drug interventions. It mitigates against community based interventions that take primary healthcare teams beyond the surgery door to promote their practice populations’ health.
Reliance on the randomised controlled trial or systematic review does not preclude indicators where the desired clinical action proves to be of questionable benefit. The incentive to reduce glycated haemoglobin concentrations below 7% in diabetic patients was revoked when subsequent research suggested this was associated with higher mortality than more liberal targets.8 The requirement to monitor people with depression using the patient health questionnaire PHQ-9 has also been reviewed with regard to the evidence for its benefit, and because it did not promote a holistic approach to assessing severity of depression.9
An added complication is that clinical commissioning groups will shortly be working to the imperatives of the CCG Outcome Indicator Set. Commissioners could find themselves promoting activities in the interests of health gain (for example, to tackle obesity) that have been rejected as QOF indicators.
Has the QOF improved population health?
The short answer is that we don’t know. Bunker calculated that better healthcare had contributed about half of the 7.5 year increase in life expectancy observed over the second half of the 20th century.10 QOF does promote important preventive activities but, against a background of many interacting determinants, we are unlikely ever to be able to attribute declines in death rates to a multifaceted intervention like the QOF.
The nationwide implementation of the QOF means that there is no natural control population with which to compare population health. However, there may have been modest cost effective reductions in mortality and hospital admissions in some areas (such as epilepsy11), and modelling studies can shed some light on possible health gain. Fleetcroft et al modelled a potential saving of 11 lives per 100 000 people per year aggregated across all clinical indicators and domains in the first year of the contract, with no further gain in the second year as performance for a typical practice already exceeded the target payment levels.12
Cost effectiveness can be modelled for only a minority of indicators (table⇓). Walker et al concluded that some QOF incentive payments were cost effective, even with only modest improvements in care, although they took no account of the costs of administering the QOF scheme. They found average indicator payments ranged from £0.63 to £40.61 per patient, and the percentage of eligible patients treated ranged from 63% to 90%.13 However, there is no relation between the size of payments in a clinical domain and the likely health gain resulting.
Cost effectiveness of Quality and Outcomes Framework indicators, 2004-0513
Inequalities in processes of care comparing the most and least deprived areas have narrowed. For example, Doran et al found that the gap in median achievement comparing practices from the most deprived and least deprived fifths narrowed from 4% to 0.8% between 2004 and 2007.14
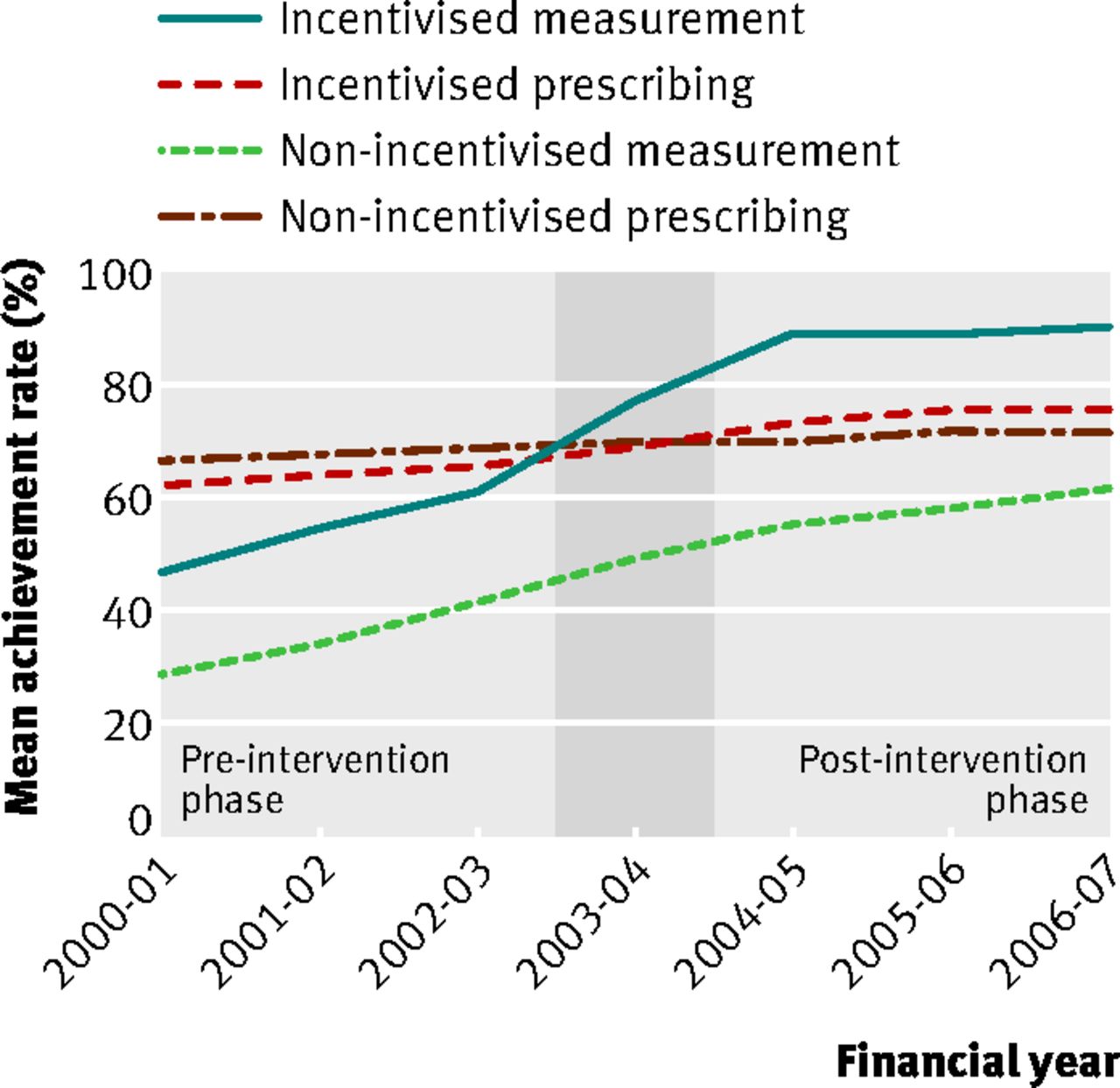
The QOF has helped consolidate evidence based methods for improving care by increasing the use of computers, decision support, provider prompts, and patient reminders and recalls.15 It has resulted in better recorded care, enhanced processes, and improved intermediate outcomes for most conditions. The quality of care for chronic conditions has improved, but the extent to which these improvements track pre-existing trends is contested.16 17 There is broad consensus that there has not been a dramatic effect. For example, measures for incentivised conditions such as cardiovascular disease, diabetes, and asthma improved over the first years of the framework at a faster rate than the pre-intervention trend and returned to prior rates of improvement in subsequent years (fig 1⇓).16 The QOF seems to have reinforced smoking cessation activities in general practice. Achievement for conditions outside the framework was lower initially and has worsened in relative terms since (fig 2⇓).5

Fig 1 Mean achievement rates of 148 general practices for quality of care indicators from 2000-01 to 2006-07. Performance indicators grouped by activity and whether they were incentivised under the QOF scheme, which came into force from 2004-0516
{kind=link}

Fig 2 Achievement for incentivised and unincentivised quality indicators in 2003 and 2005. Adapted from Steel et al5
{kind=link}
Educational interventions and community development activities are not easily measured in the QOF. As a consequence 20% of indicators refer directly to drugs, and many others will require drug treatment in order for the targets to be met. The QOF therefore contributes to polypharmacy and rising treatment costs. Prescription rates for antidepressants, statins, and other drugs have risen.18
Doctors report improved data recording and team working, and nurses enhanced specialist skills. The same interview based studies suggest that the person centredness of consultations and continuity has been negatively affected.19 20 These sometimes conflicting findings, of course, reflect the way the QOF has been designed and developed.
Doctors’ dilemmas
Some of the QOF’s design flaws are inherent to pay for performance schemes,21 and little can be done about these. For example, there is growing acceptance that rewards can undermine motivation and worsen performance of complex cognitive tasks.22 Economic research suggests that although financial incentives promote simple repetitive tasks, they can be counterproductive for tasks requiring more complex mental processes.23 Financial incentives may encourage delivery of care that follows a simple algorithm, but algorithms are hard to apply meaningfully in the real world of individuals with a variety of symptoms, diagnoses, and expectations. This research implies that the complicated conceptual process of integrating suitable care for people with chronic conditions may not be enhanced by financial incentives.
These practical concerns chime with the ethical concerns of many clinicians that a reductionist approach to managing markers of chronic disease is incompatible with the humanitarian values of general practice. Health professionals need to place biomedical care in the context of their patients’ concerns and life experience.24 The algorithm approach to healthcare exemplified by the QOF is not the best way to achieve optimum disease management for individual patients. Even NICE guidelines may have limitations when applied to populations in primary care.25 It may be possible to adapt guidelines to cater for people with multimorbidities—for example, through systematic cross referencing26—but they will always have shortcomings.27
So we are faced with conflicting conclusions about the QOF. It may have improved technical care for chronic conditions and has reduced inequalities in care. At the same time it may inhibit personalised care for the individual patient and complicate the management of multiple conditions over time. This does not diminish the ethical imperative to practise in the light of best evidence. The challenge is to deliver good quality technical care for medical conditions while simultaneously considering what is in the best interests of the whole person.
Making progress
Much valuable experience has been accumulated since 2004 that can be used to inform decisions about how the QOF could be amended to maximise benefits and minimise harms. Changes to QOF are controversial because they represent a substantial proportion of general practitioners’ incomes. Setting the political machinations to one side (the Department of Health has been clawing back from the original settlement since 2004), we believe that the incentive payments in the QOF comprise too large a proportion of general practice income. Money should be taken out of the QOF and redirected to supporting general practice in other ways. There is no link between the size of the financial incentive and likely health gain from the activity incentivised,28 and the improvements that the QOF has delivered could have been achieved with smaller incentives. The downsides of the QOF may remain with smaller incentives, but at least untied funding for general practices may help redress the imbalance it imposes.
What about thresholds? Given that average baseline performance has been above the level for maximum remuneration for all conditions since 2005, it is hard to argue against raising thresholds, as long as general practitioners can still exempt patients who may not benefit from the incentivised care.12 29
The QOF’s emphasis on single diseases does not best meet the needs of the two thirds of people over 65 who have multiple conditions. QOF targets will no doubt continue to be used for simple comorbidity, but the complex nature of managing multiple comorbidities means that payment for performance is only part of their solution.
Few indicators deal with major determinants of health such as obesity or physical activity. It has been proposed that a fixed proportion of QOF payments be dedicated to public health activities. How this would work is unclear. It would be hard to justify loosening the standards of admissible evidence—and even harder to sell to practitioners already wary of being used as tools for social engineering. However, greater discretion to set local public health related targets—for example, to support local obesity management programmes or promote exercise—could be one solution.
Our principal concern has been with clinical indicators; the effect of organisational indicators has not been evaluated. However, the indirect effects of good medicines management, enhanced education, and training on health outcomes may nevertheless be substantial. We cannot assume that performance will be sustained if these indicators are abolished. Imaginative incentives—for example, for staff training in motivational interviewing and behaviour change techniques—might promote population health. Shared decision making can take account of patient preferences and reduce healthcare costs.30 Decision aids have the potential to be incorporated in the QOF.
Finally, there is a strong argument for differential pricing that rewards practices serving more deprived populations in areas where practice population turnover is high and medical recruitment is difficult.31
Conclusion
The variation in pay for performance schemes between countries reflects different historical and organisational contexts. The burgeoning research literature shows us that benefits to patient care are at best modest, and, with so much uncertainty regarding the effects of performance related pay, policy makers are well advised to reduce the proportion of general practice income commanded by QOF.6 32 33 34 The continued evolution of indicators and payment thresholds is likely to become integrated with other quality improvement activities in general practice and with commissioning activity. Future incentives for general practices might include balanced sanctions for poorly performing practices, as there is some evidence to support the use of penalties alongside rewards.35 The evolution of the QOF, given its scale and sophistication, will attract continuing scrutiny from policy makers across the globe.
Notes
Cite this as: BMJ 2013;346:f659
Footnotes
We thank Bob Fleetcroft for his comments.
Competing interests: All authors have completed the ICMJE unified declaration form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. SG is a GP principal and both authors are members (unpaid) of the QOF advisory committee for NICE. The views expressed are not those of the NICE advisory committee.
Provenance and peer review: Not commissioned; externally peer reviewed.