Article Text

Abstract
Objective: To investigate the impact of tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) on the risk of first acute myocardial infarction (MI).
Design: Case–control analysis and a self controlled case series.
Setting: 644 general practices throughout England, Scotland, Wales, and Northern Ireland.
Patients: Over 60 000 cases of MI and 360 000 age, sex, and practice matched controls randomly selected from the UK General Practice Research Database.
Main outcome measures: Matched odds ratios and incidence rate ratios estimating whether there is an acute or prolonged increased risk of MI after exposure to TCA and SSRI drugs and individual drugs within these families.
Results: Case–control analysis found an initial increased risk of MI after TCA exposure (for example, at 1–7 days after the first dothiepin prescription: odds ratio (OR) 1.90, 95% confidence interval (CI) 1.15 to 3.14) or SSRI exposure (for example, at 1–7 days after first fluoxetine prescription: OR 2.59, 95% CI 1.44 to 4.66). In the self controlled analysis the equivalent risk estimates were an incidence rate ratio of 1.43, 95% CI 0.92 to 2.22 for dothiepin and an incidence rate ratio of 1.66, 95% CI 1.01 to 2.71 for fluoxetine.
Conclusions: Antidepressant prescriptions are associated with an increased risk of MI. The size of these effects is similar for TCA and SSRI exposures; however, the lack of specificity between types of antidepressants and the lower risks found in the self controlled analysis suggest that these associations are more likely due to factors relating to underlying depression and health services utilisation than to specific adverse drug effects.
- CI, confidence interval
- GPRD, General Practice Research Database
- IHD, ischaemic heart disease
- MI, myocardial infarction
- SSRI, selective serotonin reuptake inhibitor
- TCA, tricyclic antidepressant
- myocardial infarction
- tricyclic antidepressant
- TCA
- selective serotonin reuptake inhibitor
- SSRI
- case–control study
- self controlled case series
Statistics from Altmetric.com
- CI, confidence interval
- GPRD, General Practice Research Database
- IHD, ischaemic heart disease
- MI, myocardial infarction
- SSRI, selective serotonin reuptake inhibitor
- TCA, tricyclic antidepressant
- myocardial infarction
- tricyclic antidepressant
- TCA
- selective serotonin reuptake inhibitor
- SSRI
- case–control study
- self controlled case series
More than 10% of older people in the UK are prescribed an antidepressant each year. While tricyclic antidepressants (TCAs) are most often prescribed, prescription rates for selective serotonin reuptake inhibitors (SSRIs) have increased rapidly over the past 10 years.1–4 The two families of antidepressant have a similar efficacy for the treatment of depression but SSRI antidepressants appear to be better tolerated.2,4–7 With respect to the cardiovascular system, TCAs are associated with decreased heart rate variability8 and are cardiotoxic in overdose,9 whereas the antiplatelet effects of SSRI antidepressants mean that they may protect against cardiovascular disease or acute cardiovascular events.10–14 Findings of associations between antidepressant exposure and cardiovascular disease outcomes, however, have been inconsistent13,15–21 and TCA drugs are still commonly prescribed to people at high cardiovascular risk.17,22 One explanation for these different findings is that some studies have not been adequately powered to investigate the association of common individual antidepressants with the risk of acute myocardial infarction (MI). Furthermore, the possibility of additional confounding by depression as the underlying risk factor cannot be excluded, since depression has also been linked with ischaemic heart disease (IHD) and acute MI.21,23–26 Results of a previous case–control study of both TCA and SSRI drugs showed an increased risk of IHD with TCA exposure that was mostly attributable to dothiepin.20 Since IHD remains the most common cause of death in the UK and 5% of the elderly are prescribed dothiepin each year, there is a pressing need to define more clearly the nature of these associations.
We analysed data from over 60 000 cases of acute MI and over 360 000 age, sex, and practice matched controls from the UK General Practice Research Database (GPRD) to determine whether there is an increased risk of first MI after exposure to antidepressant drugs, whether any effects differ between types of individual antidepressant drugs, and whether the risk in an acute period after initial exposure differs from the remaining treatment period. We coupled the classic case–control analysis with the self controlled case series method to investigate and correct for the potential effect of bias and confounding in the classic approach.
METHODS
The UK GPRD
The UK GPRD contains the computerised longitudinal medical records for more than eight million people registered at over 700 general practices.27,28 The data are anonymised and regularly audited. Participating general practices record over 95% of prescriptions.29 Independent studies have consistently found the validity of diagnoses, including acute MI, to be high.30–33
Case–control analysis
We identified all cases of first acute MI diagnosed between 1 August 1988 and 30 November 2001 in the GPRD records (diagnostic code list available from authors) and defined the date of this event as the index date. Patients were 18 years of age or older at the index date. For each case, we identified up to six controls who were contributing data at the case patient’s index date and who were also matched by sex, age, and general practice. We then extracted information on all prescriptions for antidepressant drugs before the index date. Antidepressant drugs were divided into SSRIs, TCAs, monoamine oxidase inhibitors, and “other antidepressants” drug families. We used conditional logistic regression (Stata release 8.0, StataCorp, College Station, Texas, USA) to estimate the effect of ever being exposed to an antidepressant drug on the risk of a first MI. We then assessed the impact of new exposures to the more common antidepressants with at least 1% exposure prevalence in the control group, TCAs, and SSRIs by obtaining odds ratios for first MI in relation to first prescription on the index date and at 1–7 days, 8–14 days, 15–21 days, 22–28 days, and more than 28 days before the index date. In multivariable analyses we examined the impact of possible confounding by body mass index, cigarette smoking, systolic blood pressure, diastolic blood pressure, antihypertensive drug exposure, hyperlipidaemic drug exposure, and a diagnosis of diabetes, retaining only those covariates that changed the estimated odds ratio by 5% or more. Multivariable analyses were repeated for individual antidepressant drugs with an exposure prevalence of at least 1% in the control group.
Case series analysis
The self controlled case series design estimates relative incidence of an outcome in high risk compared with low risk periods within person based only on data from cases. Originally developed to assess vaccine safety, it is useful for investigating the short term impact of drug exposures on the risk of acute outcomes, since it eliminates problems of interindividual confounding, such as the extent of coronary artery disease.34
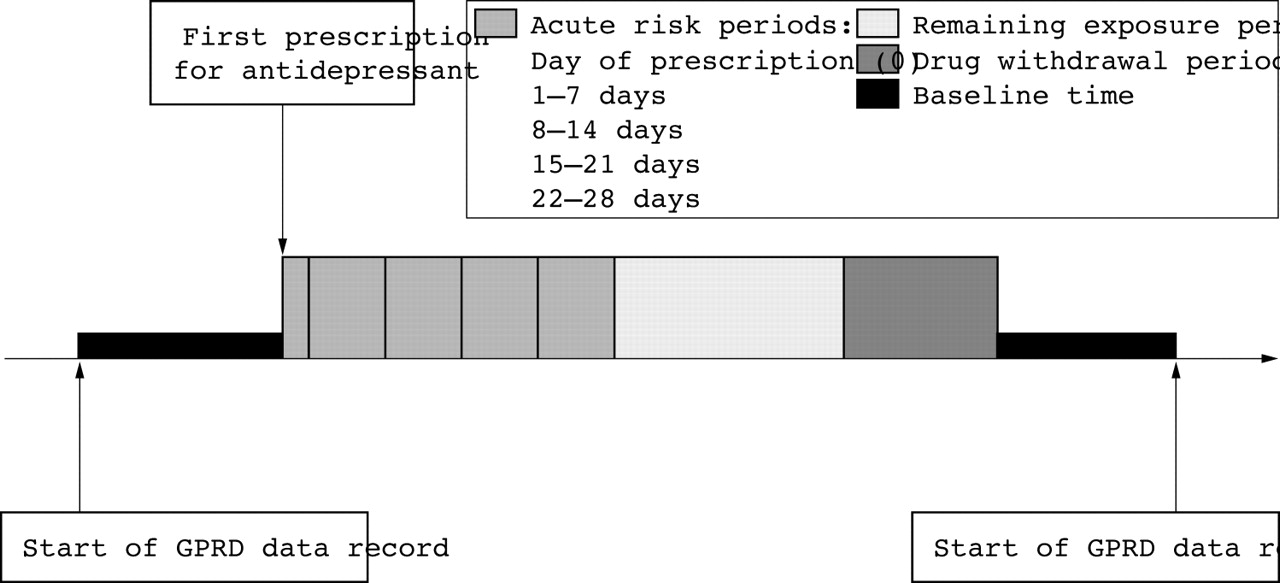
Considering only cases with at least one exposure to antidepressant drugs, we extracted all prescriptions for antidepressants before and after their first MI. We assessed the acute, prolonged, and withdrawal effects of antidepressant drugs by quantifying the relative incidence of first acute MI in predefined risk periods of drug exposure, compared with the patient’s unexposed time (fig 1). Periods of acute risk were defined as the day of first prescription (0), 1–7 days, 8–14 days, 15–21 days, and 22–28 days after first prescriptions to mimic the case–control analysis. A period of remaining exposure was defined as 29 days after the patient’s first prescription until 28 days after the last prescription, during which time patients never had more than 58 days between prescriptions (twice the median time between prescriptions). The last risk period of 29–56 days after the last prescription was designed to represent a period of drug withdrawal. All remaining person-time, when the patient was not exposed to an antidepressant drug, contributed to the baseline incidence.

{kind=link}
Division of time within the General Practice Research Database (GPRD) record of each person included in the case series approach to assess incidence of first acute myocardial infarction in relation to time of first prescription for an antidepressant.
With GLIM version 4.09 software, we conducted conditional Poisson regression to estimate incidence rate ratios, adjusted for age at first MI in five year bands. We assessed the impact of SSRI and TCA drugs and the individual drugs within these families as investigated in the case–control analysis.
RESULTS
We identified 63 512 cases of first MI and 378 886 controls. Cases and controls contributed a median of 2.4 years (interquartile range 0.5–13.3 years) of data before the case patient’s first MI. The mean (SD) age of the cases at first MI was 70.9 (12.4) years, 72% were between 50–80 years of age, and the majority of cases (61%) were men (table 1). Current smokers accounted for 27% of cases compared with 18% of controls, and first MI was associated with smoking habit in a test for trend comparing current, former, and non-smokers (p < 0.01). Increased body mass index and systolic and diastolic blood pressures were all risk factors for first MI. Cases were more likely to have a prescription for antihypertensive or hyperlipidaemic drugs prescribed before their first MI and to have diabetes diagnosed (table 1).
Characteristics of cases and controls
The prevalence of SSRI and TCA prescribing was 2.8% and 8.9%, respectively, for the controls, whereas it was only 0.1% and 0.6% for monoamine oxidase inhibitors and other antidepressants, respectively. Cases were more likely than controls to be exposed to an antidepressant drug in any drug family before the index date (table 2). This effect was marginally greater for exposure to an SSRI (crude odds ratio (OR) 1.49, 95% confidence interval (CI) 1.43 to 1.56) than for exposure to a TCA (crude OR 1.41, 95% CI 1.37 to 1.45). Exposure to individual drugs within the SSRI and TCA families before the index date was also associated with an increased risk of first MI. Effects were similar between drugs—for example, the highest crude odds ratio was for fluoxetine exposure (OR 1.54, 95% CI 1.45 to 1.64) and the lowest crude odds ratio was for dothiepin exposure (OR 1.33, 95% CI 1.27 to 1.38). Inclusion of the possible confounding variables measured did not change the odds ratios by 5% or greater so only crude odds ratios are presented.
Case–control analysis: association between antidepressant exposure and first MI
In our more detailed timing analysis of exposure, SSRI and TCA drugs were associated with acute increased risk of first MI when the first prescription was given less than 28 days before the index date (table 3). All five individual drugs were associated with acute increased risk of first MI when first prescribed on the index date and within 1–7, 8–14, 15–21, and 22–28 days of the index date; however, 95% CIs for some odds ratios included 1. Odds ratios were unaffected when we conducted sensitivity analyses by excluding patients with a prior history of vascular disease from the dataset and by excluding patients exposed to more than one antidepressant drug family (data not shown).
Case–control analysis: association between new antidepressant exposure and first MI
In the case series analysis, we identified 4132 (6.5%) cases first exposed to an SSRI antidepressant and 6735 (10.6%) cases first exposed to a TCA at some time point before or after their first MI (table 4). Of these, 1832 (44.3%) SSRI exposed patients had only one SSRI prescription and 3291 (48.9%) TCA exposed patients had only one TCA prescription. Mean age at first MI for these patients was similar to that of the whole population (63 512 cases). Cases exposed to at least one SSRI contributed a median of 7.0 years (interquartile range 4.9–9.0) of data and those exposed to at least one TCA contributed a median of 5.9 years (interquartile range 3.7–8.5). Risk of first MI was increased during the acute risk periods (the day of first prescription and 1–7, 8–14, 15–21, and 22–28 days after first prescription) for both SSRI and TCA drug families and for each individual drug (table 4), although the CIs for many incidence rate ratios included 1. During the remaining exposure period all incidence rate ratios were close to 1 for both SSRI and TCA exposure, suggesting no evidence of an increased risk of first MI. During the withdrawal period (29–56 days after the last prescription) there was an increased risk of first MI for both SSRI and TCA drugs and this effect was similar across individual drugs.
Case series analysis: association between new antidepressant exposure episode and first MI
DISCUSSION
In this large general population based sample, the results of our case–control analysis show that the use of antidepressants is associated with a transient increased risk of acute MI in the first 28 days after new antidepressant exposure. In the self controlled case series analysis, these increases were also present, but smaller, suggesting the presence of residual interperson confounding in the case–control analysis. The observed increases were not specific to SSRI or TCA exposure or to any individual drugs within these families in the results of either analysis strategy. Reassuringly, the self controlled method showed that there was no increased risk of MI with prolonged antidepressant exposure. This method also showed an increased risk of MI on withdrawal from antidepressant drugs, which may be a specific drug effect or may alternatively be due to discontinuing treatment as a result of worsening cardiovascular symptoms and development of other new illnesses.
Strengths and limitations of the study
Our use of the GPRD allowed us to study a real life clinical setting, rather than an experimental one, and provided considerable statistical power to detect possible small effects of individual antidepressant drugs, as well as the impact of exposure during short time periods after new exposure. Exposure misclassification in our study is unlikely, since GPRD practices record at least 95% of prescriptions, which are mostly computer generated.29 Our finding of TCA drugs being more commonly prescribed than SSRIs was not surprising, considering that our case ascertainment spanned from 1988 to 2001 and that prescriptions shifted towards SSRI drugs over the late 1990s. We also found that, despite a suggested contraindication of TCA drugs after an MI event, both TCAs and SSRIs were prescribed after these events, which has also been found elsewhere.18
The validity of acute vascular outcomes, including acute MI, has also been found to be high in previous studies of GPRD data.30,35 By using criteria based on the results of ECGs and cardiac enzyme assays, characteristic history, or the receipt of fibrinolytic drugs, a recorded diagnosis of MI was confirmed in over 90% of 450 cases of MI recorded in the GPRD.30–32 It is possible, however, that there is some random misclassification of the event date, since the majority of MI events are diagnosed in hospital. There may also be some systematic misclassification of event date, since a patient consulting for depression provides an opportunity for further questions from the general practitioner and may, therefore, have past diagnoses of MI recorded during the same consultation. This extra recording of MI diagnoses is likely to have the greatest effect on the day of first prescription and shortly after, and it is unlikely to have much effect in the more prolonged remaining exposure period. Thus, if present, this bias may partially explain our findings of a transient increase in risk of acute MI associated with antidepressant use. People experiencing worsening prodromal angina symptoms or post-MI depression may also be more likely to consult the general practitioner and be prescribed an antidepressant in the short period surrounding the MI. Such bias would also lead to a spurious transient association between acute MI and antidepressant exposure.
Another methodological drawback of the classic case–control approach is the issue of missing data in general practice records. When we excluded patients with missing data on health measures (such as smoking status) from the case–control analyses, however, odds ratios were largely unchanged. The presence of missing data does not affect the case series method, however, since it is essentially self controlled. Thus, the case series method has the additional advantage of removing any possible residual confounding by variables that are not included in general practice records such as the severity of depression, extent of coronary artery disease, and socioeconomic status. For this reason, we believe the case series estimates are closer to the true effect size. A limitation of both the case series approach and the case–control approach, however, is that they cannot control for factors when they change with time, such as the improvement of depression with treatment and new co-morbidity. In the acute risk periods after a first prescription (0–28 days) risk estimates are probably independent of any changes in the severity of depression, since depressive symptoms are usually unchanged during this initial exposure period. In the remaining exposure and withdrawal periods, however, we cannot rule out possible confounding by changing severity of depression or cardiovascular health. Therefore, while an independent risk of acute MI may be associated with withdrawal from any antidepressant, an alternative explanation is that people discontinued antidepressant treatment as a result of worsening cardiovascular symptoms or health in general.
Comparison with other studies
Previous studies have found no increased risk of MI with exposure to SSRI antidepressants13,16–19 but some have found an increased risk with TCA exposure.15,17 Our results for TCA drugs in the case–control analysis are similar to results of these studies, but the more conservative case series estimates suggest that part of the explanation for these results is residual confounding. It is likely that such problems were also present in previous studies. In two small case–control studies, Thorogood et al15 found an increased risk of fatal MI in women with prior TCA exposure, whereas Sauer et al13 found a decreased risk of hospitalisation for first MI with previous SSRI exposure but no association with exposure to other antidepressants, which included TCA drugs. A further study by Sauer et al16 found the same conclusions in a larger sample of 1080 cases and 4256 controls, of whom only 223 were taking SSRI antidepressants. A cohort study of hospitalisation and death from MI over four years similarly found an increased risk for TCA exposure but no association with SSRI exposure.17 In contrast, both a database study of prescribing in general practice and a large case–control study found no increased risk of MI associated with antidepressants in either family of drugs.18,19 Most studies of acute MI have been too small to investigate effects of individual drugs. However, these individual effects have been explored with IHD rather than acute MI as an outcome. In a case–control study, Hippisley-Cox et al20 found an increased risk of IHD with TCA drugs but not with SSRIs; within the TCA drug family, the strongest association was found with dothiepin, although there was also an increased risk with lofepramine. In our study, we did not replicate these specific drug effects. The reasons for inconsistent results from studies of MI and IHD are not clear but include limited statistical power in some studies, the presence of depression as a likely confounder,21,23,26 the varying severity of underlying depression, and prescribing bias (or indication bias) resulting from preferential prescribing of certain antidepressants and not others, based on the general practitioner’s assessment of the patient’s cardiovascular risk status.
Clinical implications
We found a transient increased risk of acute MI in the initial 28 days of exposure to antidepressant drugs, which did not persist after this period. This suggests that people now taking antidepressants do not need to stop taking these drugs, as no increased risk is conferred by prolonged exposure. Furthermore, the finding that the transient increased risk was not specific to TCA or SSRI drugs or to individual drugs within these families indicates that the association is unlikely to be a causal drug effect and may be due to underlying depression or health services utilisation. An increase in inflammatory activity for other physiological reasons may lead to both MI and depressive illness. The increased risk of MI on withdrawal from antidepressant drugs, however, warrants further investigation for a clinical explanation. While this may be a specific drug effect, it may reflect a discontinuation of treatment as a result of worsening cardiovascular symptoms or the development of other illness.
Acknowledgments
We thank Dr Julia Hippisley-Cox and Professor Mike Pringle from the Division of Primary Care, University of Nottingham for their valuable advice during the project and comments on the manuscript.
REFERENCES
Footnotes
-
Source of funding: Junior Research Fellowship for L J Tata, School of Community Health Sciences, University of Nottingham