Article Text

Abstract
Diagnosis and treatment of latent tuberculosis infection (LTBI) is important to reduce risk of progression to active tuberculosis (TB) disease. For the past century the tuberculin skin test (TST) has been used as a measure of exposure to Mycobacterium tuberculosis (MTB), but this test has limitations in test performance, sensitivity and specificity. Interferon γ release assays (IGRA), like TST, measure host immune response to MTB. IGRA are designed to be more specific for the diagnosis of LTBI than TST in patients with previous BCG or exposure to non-tuberculous mycobacteria, detecting interferon γ generated by T cells in response to antigens more specific to MTB. Although developed as an alternative to TST, recent data, particularly in children, suggest IGRA have their own limitations. Superiority to TST as a diagnostic test in children has not been demonstrated. Neither test discriminates between current or past MTB infection, or between latent infection and active disease. This article reviews the current literature on sensitivity and specificity of IGRA in the diagnosis of LTBI, and summarises current NICE recommendations for the use of IGRA in combination with TST. Although not developed for this purpose, in clinical practice IGRA have also been used as a diagnostic test for active TB. The gold standard for diagnosis of active TB disease is microbiological confirmation by culture of MTB. This article discusses the utility of IGRA as an adjunct to diagnosis of active TB disease, but emphasises that IGRA do not have sufficient sensitivity or specificity to exclude or confirm active TB disease.
- Evidence Based Medicine
- General Paediatrics
- Infectious Diseases
- Respiratory
- Immunology
Statistics from Altmetric.com
Introduction
In 2011 there were an estimated 8.7million new tuberculosis (TB) cases, and 1.4 million TB deaths worldwide.1 Although large parts of the UK do not qualify as an endemic setting for TB, the overall incidence of TB is 14.4/100 000 population with areas in London with as high as 43/100 000 population—and 5% of all cases were reported in children less than 15-years-old.2 Paediatricians in the UK are therefore likely to come across families affected by TB on a regular basis and ought to be familiar with the latest recommendations for diagnosis and management. In this article, we review the utility of interferon γ release assays (IGRA) for the diagnosis of childhood TB.
Only around 30% of all individuals exposed to Mycobacterium tuberculosis (MTB) develop latent infection,3 with a 5%–10% lifetime risk of progression to active TB disease.4 However, young children are particularly vulnerable to progression to active disease, and to disseminated forms of TB. If untreated, the risk of progression from latent infection to active pulmonary disease in infants is 30%–40%, while the risk of severe forms of disease such as TB meningitis or miliary disease is 10%–20%.5 Treatment of latent infection reduces this risk by 60% or more and is therefore recommended.6
How do we identify the ‘right’ patients for treatment of LTBI?
There is no gold standard for diagnosis of latent TB infection (LTBI). For the past century, the tuberculin skin test (TST) has been used as a measure of exposure to MTB, but this test has well-recognised limitations in test performance, sensitivity and specificity. IGRA were developed as an alternative to TST: early adult studies appeared promising, but more recent data, particularly in children, suggest that IGRA have their own limitations (table 1). Superiority to TST as a diagnostic test in children has not been demonstrated. Nevertheless, several national guidelines now recommend the use of IGRA, alone or in combination with TST, in screening algorithms for LTBI.7 ,8
Comparison between TST and IGRA
Although not developed for this purpose, in clinical practice IGRA have also been used as a diagnostic test for active TB. It is important to emphasise that the gold standard for diagnosis of active TB disease is microbiological confirmation by culture of MTB. However, due to the paucibacillary nature of childhood TB, even with ideal diagnostic techniques as few as 16% of paediatric TB cases are culture positive.9 Unfortunately, IGRA do not provide the solution as they do not discriminate between LTBI and TB, and lack the sensitivity and specificity required to confirm or exclude active disease.
Physiological background
Essentially, the same principles underlie TST and IGRA: both are tests of host immune responses and neither can directly measure the presence or absence of mycobacteria.
In TST, a small amount of tuberculin, which is a mixture of mycobacterial purified protein derivatives containing proteins from all kinds of mycobacteria, including BCG purified proteins, is injected intradermally into the skin of the forearm. Once the injected tuberculin antigens are processed by the antigen-presenting cells in the skin and following interaction with T cells, a delayed-type memory response occurs at the site of injection, which implies that the hosts’ immune system has previously been sensitised to the antigen injected. The induration is caused by the recruitment of sensitised T cells to the site of injection and the release of lymphokines, which induce induration through vasodilatation, oedema and recruitment of additional pro-inflammatory cells and cytokines to the area. TST can be positive if someone currently has TB, if they were exposed to MTB in the past or if they received the BCG vaccine.
In contrast, the antigens used for IGRA are much more specific for MTB. The blood-based IGRA currently exist in two commercially available preparations: T-SPOT.TB (Oxford Immunotec) and QFG-IT (Qiagen).
A period of between 2 and 12 weeks postexposure to MTB is usually necessary in order for TST to become positive. The same is likely to be true for IGRA.
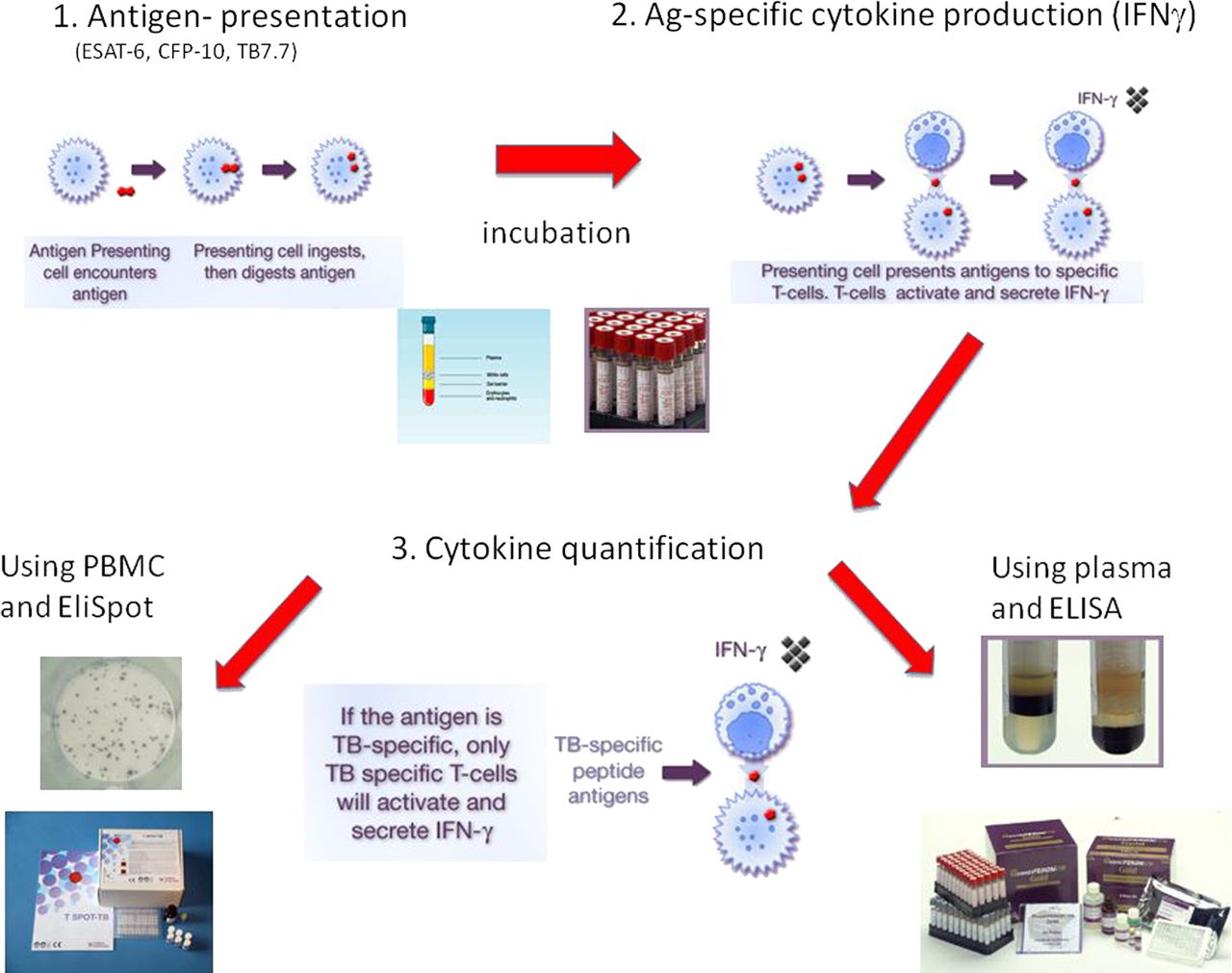
The specific antigens contained in IGRA are early-secretory protein 6 (ESAT-6) and culture-filtrate protein (CFP)-10 for the T-SPOT.TB plus an additional antigen called TB 7.7 in the QuantiFERON-TB Gold In-tube test (QFG-IT).
The improved specificity of IGRA compared with TST is due to the fact that ESAT-6 is not expressed by BCG, which makes it possible to distinguish between a TST which is positive due to BCG vaccination and a TST which is positive due to sensitisation to MTB. ESAT-6 is also expressed by Mycobacterium bovis, Mycobacterium leprae, Mycobacterium africanum, Mycobacterium kansasii, Mycobacterium marinum, Mycobacterium szulgai and Mycobacterium smegmatis, but these play less of a role in the context of screening of children or adults for LTBI in a UK setting and in immunocompetent hosts.
Technological background
The immunological principles of both IGRA tests are summarised in figure 1. Some technical tips are summarised in table 2. Cost varies, but is usually in the region of £15–£60 per assay, with QFG-IT being the cheaper assay. Both tests require special blood bottles and reagents preordered from the manufacturer. Dependent on local arrangements, tests may be performed by either NHS Trust or Health Protection Agency laboratories, usually within immunology or microbiology laboratories. Although results can be available within 24 h if needed, in practice, many labs batch samples to conduct one or two runs per week, depending on demand. Close liaison with the providing laboratory is recommended to ensure efficient timing of the test.
Technical tips for IGRA

{kind=link}
Immunological principles of commercially available interferon γ release assays.
The QFG-IT test requires 3 ml of venous blood, which is drawn into three 1 ml tubes, which are precoated with no antigen (negative control), specific MTB antigens or phytohaemaglutinin (positive control). Careful mixing by inverting the sample bottles up to 10 times is recommended. Overfilling or underfilling or vigorous shaking of the tubes can lead to unreliable results. Tubes should be sent to the lab within 12 h, the sooner the better. In the lab, samples are incubated at 37°C for 18–24 h. Plasma is then separated by centrifugation. The plasma sample can either be analysed immediately or frozen or refrigerated for a specified period of time. Tests can then be run in batches depending on urgency of results and individual lab protocols. The read-out is the level of the key cytokine interferon γ produced during the incubation and secreted into the supernatant, measured using an enzyme-linked immunoassay. The software-generated results are presented as an equation, which integrates the antigen-specific result with the values for the positive and negative controls. The end result is reported as negative, positive or indeterminate. Indeterminate tests are not interpretable clinically and should be repeated.
The T-SPOT.TB test ideally requires 5 ml of venous blood, which is collected in a single tube designed for the preparation of peripheral blood mononuclear cells in the laboratory. Blood should reach the lab as soon as possible to be separated by skilled personnel. The cells are collected following centrifugation steps and washes, counted and then plated out in precoated special tissue culture plates containing no antigen (negative control), MTB-specific antigens or phytohaemaglutinin (positive control). The plates are incubated overnight at 37°C, washed and the assay then developed with additional reagents to finally visualise the number of antigen-specific T cells producing the key cytokine (interferon γ). These are then enumerated in comparison with the negative and positive controls using an Elispot reader instrument. The results are reported as negative, positive or uninterpretable, which can happen due to technical problems, such as high background in the Elispot. Such assays ought to be repeated.
Indications and limitations
How sensitive are IGRA in identifying children with LTBI?
Assessing the sensitivity IGRA in LTBI is problematic, since there is no gold standard diagnostic test for comparison. A number of studies measure sensitivity in populations with culture confirmed active TB as a surrogate for latent infection, but this approach is methodologically flawed, since populations with latent infection and active disease are epidemiologically, clinically and immunologically distinct. Sensitivity of IGRA in active TB is discussed below. Other studies compare IGRA with TST to assess performance. While such studies may provide useful information about concordance between TST and IGRA results, they cannot be used to estimate diagnostic sensitivity since neither test is a gold standard for LTBI.
An alternative approach is to assess the correlation of IGRA results and known exposure to MTB. Since risk of TB infection increases with increased exposure, a test strongly correlated with exposure would be expected to identify patients at the highest risk. A meta-analysis of such studies in children found that the odds of a positive QFG-IT (or an earlier version QuantiFERON Gold (QFG)) test were higher in children who were exposed, than those unexposed, to TB (OR 3.51, 95% CI 1.85 to 6.66). In these studies, QFG-IT/QFG appeared to be more accurate than T-SPOT.TB or TST (10 mm cut-off) (OR 1.31, 95% CI 0.76 to 2.27 and OR 1.93, 95% CI 0.98 to 3.77, respectively); however, the reviewers concluded that due to significant heterogeneity between studies, and wide CI, the evidence was not sufficient to establish superiority of any of the three tests.10
A third approach is taken in longitudinal studies which evaluate the proportion of IGRA positive or negative subjects who develop active TB disease over time. Although such studies do not directly measure LTBI, this approach is the most relevant to the important clinical question: ‘how accurately does this test identify subjects who would benefit from treatment?’ Two published studies which included child TB contacts in Japan11 and Germany12 reported variable but low positive predictive value (0% (95% CI 0 to 35), 43% (95% CI 16 to 75)) but high negative predictive value (100% (95% CI 0 to 1.5), 100% (95% CI 0 to 3)), respectively. Both studies had major limitations. In the Japanese study only 41/313 children were close contacts of the index case. The remainder were defined as ‘casual contacts’ with less than 18 h potential exposure. Only 9/313 had a positive IGRA. In the German study only 66/601 participants were children under 16, and only 18 of these were under 6-years-old. Only three children had a positive IGRA. Both studies were limited by short follow-up periods and by the confounding effect of interventions such as prophylactic treatment.
In the absence of a gold standard for comparison, or reliable surrogate data, a meaningful ‘sensitivity’ figure for IGRA in the diagnosis of LTBI cannot be given at present. There is currently insufficient evidence that IGRA are sufficiently sensitive for a negative test to ‘rule out’ LTBI in children.
How specific are IGRA in identifying children with LTBI?
Estimating the specificity of IGRA is similarly problematic. Studies undertaken in healthy individuals at low risk of LTBI in low incidence settings have been used to model a population of ‘true negatives and false positives’. A systematic review and meta-analysis of specificity studies (which included both adults and children) reported pooled specificity for QFG-IT from four studies of 99.4% (95% CI 97.9% to 99.9%), and a single study reporting specificity for T-SPOT.TB of 98% (95% CI 86.8% to 99.9%).13 Three studies reported specificity of TST to be lower than IGRA, with a pooled specificity of 88.7% (95% CI 84.6 to 92.0).13
In summary, a positive IGRA is highly suggestive of infection with MTB. However, false positives do occur. In clinical settings where the likelihood of TB infection is low, the risk that a positive test is actually ‘false positive’ is higher. Results should always be considered in a clinical context.
LTBI and IGRA in clinical context
IGRA should only be used and interpreted in the wider context of a clinical assessment of risk of TB. National Institute for Clinical Excellence (NICE) clinical guideline 117 includes detailed algorithms for the investigation and management of children of children at risk of LTBI.7 This guideline is under review, but current recommendations are summarised in box 1.
Summary of NICE guidelines for use of IGRA in children at risk of LTBI
-
1. Children who have been in close contact with patients with active TB disease
-
a. Neonates
-
Neonates are at the highest risk of progression to active disease and of severe forms of TB.
-
All neonates should commence prophylactic Isoniazid treatment for 3 months.
-
At 3 months check TST. If positive, exclude active TB and complete a further 3 months Isoniazid. If negative, check IGRA and repeat TST. If either is positive exclude active TB and complete a further 3 months Isoniazid.
-
b. Children under 5 years
-
These children are also at high risk. Children under 2 years are particularly vulnerable. There are separate NICE algorithms for children age 4 weeks to 2 years, and age 2–5 years, and for children with and without prior BCG vaccination.
-
Children age 4 weeks to 2 years without prior BCG should start Isoniazid prophylaxis while investigations are ongoing. NICE guidelines do not recommend immediate prophylaxis for children with prior BCG, or those age 2–5 years.
-
Check TST. If positive, exclude active TB and treat for LTBI with 6 months Isoniazid, or 3 months Isoniazid/Rifampicin.
-
If initial TST is negative, repeat TST and check IGRA after 6 weeks. If either is positive exclude active TB and consider treatment for LTBI, with treatment strongly recommended for children under 2 years.
-
c. Children over 5 years
-
The risk of progression to active disease is relatively low in the 5–10 years age group, although in adolescence the risk of adult-type pulmonary disease increases.
-
Isoniazid prophylaxis during investigation is not recommended.
-
Check TST. If positive, check IGRA.
-
If initial TST is negative, repeat after 6 weeks. IGRA can be considered if results of TST are thought to be unreliable.
-
If either IGRA or TST is positive at any stage active TB should be excluded. However, treatment for LTBI is only recommended if both tests are positive.
-
2. Children who are recent arrivals from high prevalence countries
-
In the UK, 74% of reported TB cases occur in individuals who were born in other countries.2 Child migrants arriving in the UK from countries with a TB incidence of more than 40/100 000 (most of the world) should be screened for LTBI in an approach similar to that described in child contacts above.
-
3. Children with immune suppression
-
Children with immune suppression are at a higher risk of progression of LTBI to active TB and of atypical TB disease. Both TST and IGRA are less sensitive in immune suppressed individuals.
-
Check both TST and IGRA. If either is positive, refer to specialist to exclude active TB and treat for LTBI.
IGRA, interferon γ release assays; LTBI, latent TB infection; TB, tuberculosis; TST, tuberculin skin test.
What about indeterminate results?
A systematic review of IGRA studies in children reported average rates of indeterminate results across all studies of 6.5% for QFT-GIT and 3.5% for T-SPOT.TB.10 A number of studies report higher rates of indeterminate results associated with younger age,14 helminth co-infection and immune suppression, but a significant correlation of indeterminate results with specific risk factors was not demonstrated in meta-analyses.10
Indeterminate results may be due to technical laboratory factors or individual variation and should not be accorded any clinical significance. The test should be repeated.
Can IGRA be used to diagnose active TB disease?
IGRA are not recommended for diagnosis of active TB disease. Like TST they cannot distinguish between LTBI and active disease. Reviews of the published literature on their utility in paediatric TB are limited by the heterogeneity of case definitions, relatively small numbers of microbiologically confirmed (‘gold-standard’) TB cases and diverse methodologies.
Sensitivity for definite and/or probable TB disease in children shows no significant difference between TST and IGRA with pooled sensitivities of 80% for TST (95% CI 70 to 90), 83% for QFT-GIT (95% CI 75 to 92) and 84% for T-SPOT.TB (95% CI 63 to 100). In stratified analyses, sensitivity for all three tests is reduced in low or middle income countries, where the average age of children was under 5 years, in HIV-infected populations and when BCG vaccination was >50%.10 Indeed, there is a reduced IGRA sensitivity of 55% (95% CI 37% to 73%) in high incidence settings compared with low incidence settings, and 70% (95% CI 53% to 84%) in another meta-analysis.15 The combination of young children (less than 3-years-old) in a high incidence country (South Africa) gave a sensitivity for definite or probable TB of 35% for TST>10 mm (95% CI 22 to 49) and 42% for QFT-GIT (95% CI 26 to 59).16
When comparing cases of probable or definite TB with paediatric household contacts or suspected TB cases where active TB was systematically excluded, the CI for each test overlap, with pooled specificity of 85% for TST (95% CI 63 to 100), 91% for QFT-GIT (95% CI 78 to 100) and 94% for T-SPOT.TB (95% CI 87 to 100).10
It is important to note that the sensitivity and specificity of TST are dependent on the cut-off measurement used for a positive test. In the UK, the thresholds used are ≥6 and ≥15 mm for individuals with and without BCG vaccination, respectively, but a threshold of ≥10 mm is commonly used internationally. In stratified analysis, the sensitivity of TST decreased from 91% using a 5 mm threshold to 67% using a 15 mm threshold, while specificity increased from 70% to 92%, although this analysis was not corrected for BCG status.10 The apparent advantages in specificity in IGRA over TST are to some extent dependent on context and TST threshold used.
Overall, although IGRA can serve as a useful adjunct in the evaluation of children suspected of TB disease, they are not superior to TST.17 ,18 They are not sensitive enough for a negative result to act as a ‘rule out’ nor specific enough for a positive test to definitely confirm TB.
Topics for further research
Sadly, neither IGRA nor new molecular bacteriological diagnostics hold ‘the’ answer for diagnosing either latent infection or TB disease in childhood.9 Greater understanding of the strengths and limitations of IGRA can only come about through prospective cohort studies assessing their positive and negative predictive values. Studies of positive predictive value will always be confounded by appropriate treatment of young children with LTBI, as internationally recommended. A multi-centre study based in the NHS in the UK—the NIHR-funded IGRA in Kids Study—is currently ongoing to determine the negative predictive value of IGRA in children. Prospective data collection tools which can relate index cases to their contacts and capture previous results for diagnostics for LTBI and subsequent management are also required.
Gene expression profiling has yielded potential diagnostic signatures for TB disease in adults that may also track response to treatment, but the ability to reliably distinguish LTBI from controls remains elusive at present.19 In any discovery approach, it is of critical importance that children of all ages are included in research to discover and validate novel markers for active and latent TB to ensure that our standards of diagnosis and care of children with TB do not lag behind that of adults.
Clinical summary
-
Diagnosis and treatment of latent tuberculosis (TB) infection (LTBI) is important to reduce risk of progression to active TB disease.
-
There is no gold standard diagnostic test for LTBI. Interferon γ release assays (IGRA), like tuberculin skin test (TST), measure host immune response to Mycobacterium tuberculosis (MTB) antigens. Neither test discriminates between current or past MTB infection, or between latent infection and active disease.
-
IGRA are designed to be more specific for the diagnosis of LTBI than TST in children with previous BCG or exposure to non-tuberculous mycobacteria.
-
Neither TST nor IGRA have been demonstrated to be superior in the diagnosis of LTBI in children.
-
The gold standard diagnostic test for active TB disease is microbiological confirmation by culture of MTB. IGRA do not have sufficient sensitivity or specificity to confirm or exclude a diagnosis of active TB disease.
Test your knowledge
QUESTION 1
The risk of progression of latent tuberculosis (TB) infection (LTBI) to active TB disease is…
-
Highest in infants under 1 year
-
Highest in adolescence
-
Highest in the 5–10-year age group
-
Highest in the 2–5-year age group
QUESTION 2
In the diagnosis of LTBI in children…
-
IGRA are more sensitive than tuberculin skin test (TST)
-
TST are more sensitive than interferon γ release assays (IGRA)
-
IGRA are more specific than TST in individuals with previous BCG vaccination
-
IGRA are more specific than TST in infants
QUESTION 3
In active TB disease in children…
-
A negative IGRA can be used to rule out active TB
-
A positive IGRA can be used to confirm active TB
-
A negative sputum culture rules out active TB
-
The majority of children have paucibacillary disease
QUESTION 4
In the management of child contacts of patients with sputum positive TB…
-
Neonates should receive BCG vaccination as soon as possible after birth
-
Children aged 2–5 years with a negative initial TST should have a repeat TST and IGRA after 6 weeks
-
Children aged 5–15 years with a negative initial TST can be discharged with no further follow-up
-
A TST of 8 mm in a child with previous BCG should be considered positive
QUESTION 5
According to NICE guidelines treatment of LTBI should be considered…
-
In a child migrant age 3 years with a positive TST and negative IGRA
-
In a child with HIV age 12 years with a positive TST and cavitation on chest x-ray
-
In a child contact of sputum+TB aged 8 years with a positive TST and negative IGRA
-
In a child contact of sputum+TB aged 6 years with a negative TST and negative IGRA
-
See page 105 for the answers.
Answers to the quiz on page 104
-
a
-
c
-
d
-
b
-
a
References
Footnotes
-
Contributors LP led the project. All authors reviewed the relevant literature, contributed to and revised the text and agreed on the final draft.
-
Funding We would like to acknowledge our research funding from NIHR grant number SRF-2009-02-07 (BK, RBR), the BRC at Imperial College (BK, LP) and the Medical Research Council grant number MR/K011944/1 (BK, LP).
-
Competing interests Our laboratory has received discounted consumables for interferon γ release assays from both companies that market the commercially available IGRA. None of the companies has ever been involved in the design of our research studies using IGRA or interpretation of the results.
-
Provenance and peer review Commissioned; externally peer reviewed.