Article Text

Abstract
Background Many patients visit the accident and emergency department (AED) on their own initiative, although their medical problem can be adequately treated by a general practitioner (GP).
Objective To evaluate the cost-effectiveness of addition of a GP to the AED (new care method) in comparison with usual care (usual care method).
Methods This study followed a before/after design. Patients attending the AED without a referral on weekdays from 10:00 to 17:00 were invited to participate. Main outcome measures were process time, patient satisfaction and number of correct diagnoses. Costs were measured from a societal perspective. Bootstrapping was used to estimate uncertainty around differences in costs and incremental cost-effectiveness ratios. Cost-effectiveness planes and acceptability curves were presented.
Results Addition of a GP to the AED resulted in significantly lower process time, significantly higher patient satisfaction and no statistically significant difference in the number of correct diagnoses. Total costs per patient were €217 in the new care period and €288 in the usual care period (mean difference −€71, 95% CI −121 to −23). The cost-effectiveness analysis showed that the new care method was dominant (more effective, less expensive) in comparison with the usual care method for process time and patient satisfaction. The new care method was considered cost-effective in comparison with the usual care method for ceiling ratios between €0 and €1363 for the number of correct diagnoses.
Conclusion The new care method consisting of addition of a GP to the AED is cost-effective in comparison with usual care for all outcome parameters measured.
- Cost effectiveness
- emergency care systems
- emergency care systems
- primary care
Statistics from Altmetric.com
Introduction
Accident and emergency departments (AEDs) are equipped to manage patients needing acute specialist care. However, many patients visit the AED on their own initiative, although their medical problem can be adequately treated by the general practitioner (GP). A recent review showed that prevalence of inappropriate use of AED services ranged from 20% to 40% and that most inappropriate AED use occurs during working hours.1 High rates of inappropriate AED users may lead to overcrowded AEDs and increased waiting times.2 3
The large majority of self-referrers regard the AED as the most appropriate place to present their problem due to its diagnostic and therapeutic potentialities.3 4 This may explain why interventions aimed at changing patient behaviour have not been particularly effective.5–8 However, employment of GPs in the AED may be an effective means of managing inappropriate AED users with no consequences for safety or patient satisfaction, and with reduced rates of resource utilisation and lower costs.9–12
At the VU University Medical Center a new care method was implemented consisting of addition of a GP to the AED and triage by nurses to allocate patients to either the GP or the AED physician. In this study, we investigated whether this new care method was cost-effective in comparison with usual care using process time, patient satisfaction and number of correct diagnoses as outcomes. We previously reported that this new care method had positive effects on patient satisfaction while maintaining quality.13
Methods
This study followed a before/after design and was executed at a busy AED of an academic hospital (VU University Medical Center, Amsterdam). A randomised controlled trial was not possible, because this would have disturbed daily practice too much. The study was approved by the Human Medical Ethics Committee (METC) of the VU University Medical Center, Amsterdam.
Population
Self-referrers who attended the AED on weekdays during the day (10:00–17:00) from 1 November 2006 to 30 April 2007 were invited to participate. Exclusion criteria were: referral by a GP, brought in by ambulance, less than 16 years of age with no legal guardian present, insufficient knowledge of the Dutch language, and mental impairment. During the reference period, 1 November 2006 to 1 February 2007, 832 patients were enrolled in the study, and during the experimental period, 1 February 2007 to 30 April 2007, 695 patients were enrolled.
Usual care method
In the usual care period, self-referrers checked in at the reception desk. The receptionist determined whether there was an acute life-threatening health problem. If so, a nurse immediately accompanied the patient to see a doctor. If not, the patient was invited to participate in the study by the receptionist, received oral and written information, and was asked to give informed consent. All patients were treated as usual by the AED team (one surgeon and two residents).
New care method
In the new care period, the self-referrer checked in at the reception desk and was immediately directed to the triage nurse. A nurse allocated patients to either the GP or the AED physician according to the Netherlands Triage System.14 Patients who needed immediate treatment were directly referred to the AED physician. All patients who were not immediately in need of emergency help were asked to participate in the study by the triage nurse and to give informed consent. Patients referred to the AED physician were treated similarly as in the usual care period. Patients allocated to the GP were seen by either a GP or a GP trainee. The GP trainee was in his third training year and was supervised by the GP.
Outcome measures
Data on the reason for the AED visit, the symptoms and the medical history were recorded on a standardised form by the receptionist. Data on age, gender, ethnicity, level of education, comorbidity and other visits to the AED during the trial period were also collected by the receptionist.
The primary outcomes of this economic evaluation were patient satisfaction and process time. Normally, quality of life is also included as a primary outcome in an economic evaluation. However, we expect that the most important effects of the intervention are on patient satisfaction and process time and do not expect an effect on quality of life. Patient satisfaction was measured using a patient questionnaire developed by the Erasmus University Medical Center in Rotterdam.15 Patients could fill in this questionnaire immediately or take the questionnaire home and return it by mail. Process time was defined as the time between the patient's arrival to and departure from the AED. Administrative personnel recorded these times in the patients' charts. Secondary outcome was the number of correct diagnoses. The proportion of correct diagnoses was established by requesting the patient's own GP to verify the AED diagnosis 4 weeks after the patient's visit to the AED. If the GP diagnosis was not concordant with the AED diagnosis, two researchers determined (blinded for the intervention category) whether the original AED diagnosis was relevantly incorrect.
Cost measures
The economic evaluation was performed from a societal perspective. Table 1 lists the cost categories included and the measurement methods used to collect these cost data. Medical costs included the costs of diagnostic and therapeutic interventions at the AED, time spent on treatment by AED physicians, and treatments planned after discharge from the AED. Process time costs included the time spent by patients at the AED (waiting and treatment time).
Cost categories, measurement method and prices used in this economic evaluation
Diagnostic and therapeutic interventions were valued using costs from the hospital financial administration. Time spent on treatment by GPs and AED physicians was valued using salary information. Standard costs were used to value treatment after discharge. A shadow price of €8.73, which corresponds to the hourly tariff of a legally employed cleaner, was used to value process time.16 Prices applied in this economic evaluation are listed in table 1. All prices were adjusted to the year 2007 using price index figures.17
Statistical analysis
To be able to detect a difference of 10% (from 65% to 75%) in the number of patients who rate their satisfaction with their AED visit as 6 or higher (scale 1–10), 285 patients per group were needed (one-sided α 5%, power 80%). All analyses were limited to patients with complete follow-up. All participating patients in the new care method (allocated to the GP and AED physician) were included in the analysis.
Costs generally have a highly skewed distribution, because most patients incur relatively low costs and a few patients incur very high costs.18 Therefore, bootstrapping with 5000 replications was used to estimate 95% CIs around the differences in costs between the new care method and the usual care method.
Incremental cost-effectiveness ratios (ICERs) were calculated by dividing the difference in costs between the new care method and the usual care method by the difference in effects between the two care models. To avoid double counting the numerator did not include total costs for all ICERs (see table 2). Bootstrapping with 5000 replications was used to estimate the uncertainty surrounding the ICERs. The bootstrapped cost–effect pairs were plotted on cost-effectiveness planes (CE planes)19 and used to estimate cost-effectiveness acceptability curves (CEA curves).20
Calculation of incremental cost-effectiveness ratios (ICERs) for the new care method versus usual care method
Results
During the study period 2102 self-referring patients visited the AED, of whom 1150 visited during the usual care period and 952 during the new care period. Thirteen per cent of the patients in the usual care period and 14% of the patients in the new care period were excluded from the study, because of language problems, the patient being younger than 16 years and no adult present, mental problems, or the patient being no self-referrer. Of the 996 eligible patients in the usual care period, 832 (84%) were willing to participate as were 695 (84%) of the 827 eligible patients in the new care period. Reasons for non-participation were pain, unwillingness, and leaving the AED prematurely. During the new care period, 584 (84%) patients were allocated to the GP after triage and 111 (16%) were allocated to the AED physician.
Table 3 shows the baseline characteristics of patients receiving the new care method and patients receiving the usual care method. There were no relevant differences in sex, age, ethnicity, education or medical history between patients in both periods.
Baseline characteristics for patients in the new care method and usual care method patients
Complete cost data were available for all patients. Data on process time were available for 96% of the patients, data on patient satisfaction for 64%, and data on correct diagnoses for 72%. There were no relevant differences in baseline characteristics or costs between patients with and without complete follow-up.
Outcome measures
Mean process time in the new care period was 69 min (SD 59) versus 93 min (SD 59) in the usual care period. This difference in process time of 24 min was statistically significant (95% CI −30 to −18). Patients in the new care period graded their AED visit on average as 7.7 (SD 1.2), and patients in the usual care period as 7.3 (SD 1.3). Patient satisfaction in the new care period was significantly higher than in the usual care period (mean difference 0.4, 95% CI 0.3 to 0.6). The diagnosis was unchanged by the GP in 97% of the patients in the new care period and in 98% of the patients in the usual care period. This difference was not statistically significant (95% CI −0.03 to 0.01).
Costs
Table 4 presents the costs in the two care periods. Total mean costs per patient in the new care period were statistically significantly lower than in the usual care period (mean difference −€71, 95% CI −121 to −23). Medical costs were the largest contributor to this difference in total costs (mean difference −€68, 96% of total cost difference). Costs of therapeutic interventions were also statistically significantly lower in the new care period than in the usual care period. The difference in costs of diagnostic interventions was also substantial, but not statistically significant. Process time costs in the new care period were statistically significantly lower than in the usual care period (mean difference −€4, 95% CI −4 to −3).
Mean (SD) costs (€, 2007) per patient for new care method and usual care method patients
Cost-effectiveness
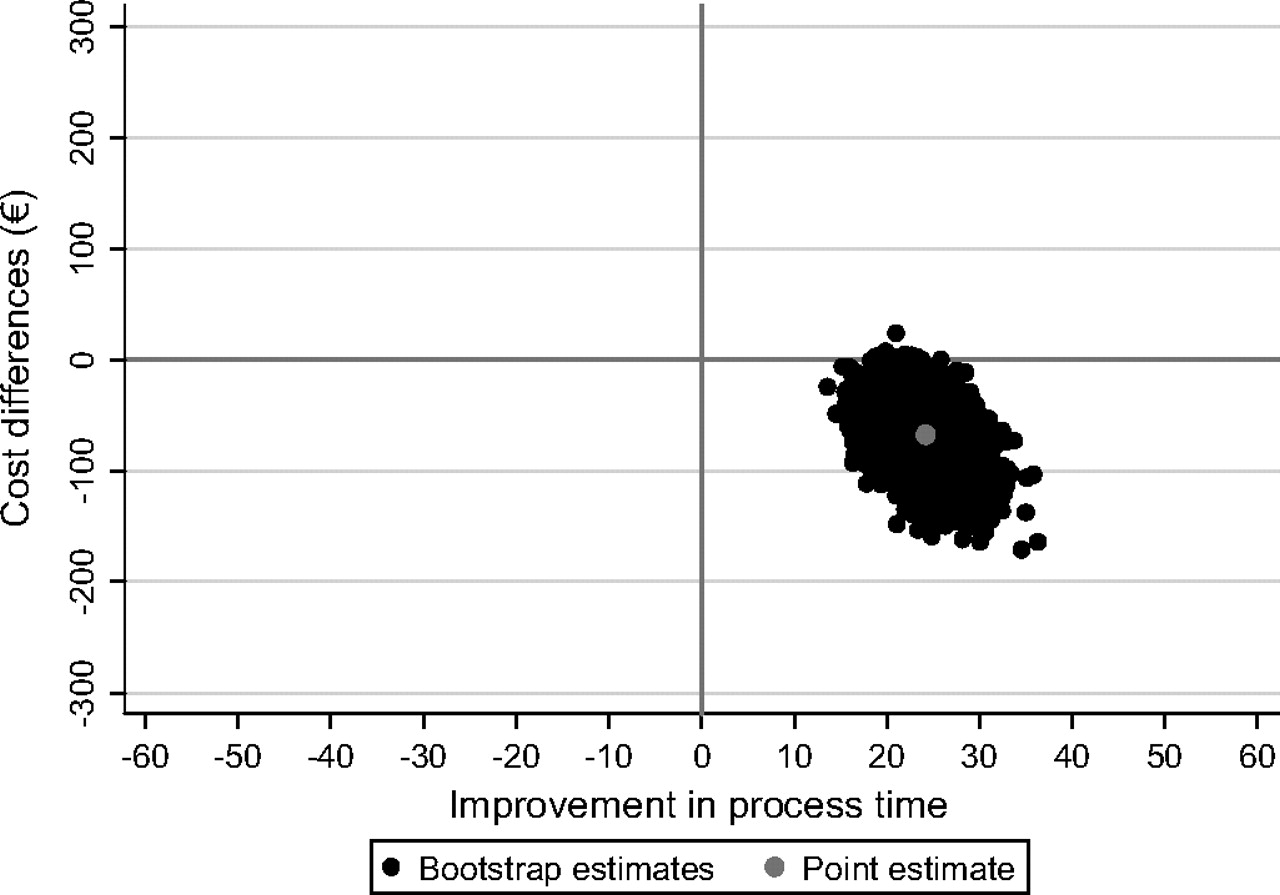
Figure 1 shows the cost-effectiveness plane for process time. The cost-effectiveness plane confirms the findings of significantly lower process time and lower costs in the new care period in comparison with the usual care period. Almost 100% of the bootstrapped cost–effect pairs was located in the southeast quadrant of the cost-effectiveness plane (lower process time and lower costs), indicating that the new care method was dominant in comparison with the usual care method. The cost-effectiveness acceptability curve shown in figure 2 indicates that for all possible ceiling ratios the new care method was cost-effective in comparison with the usual care method.
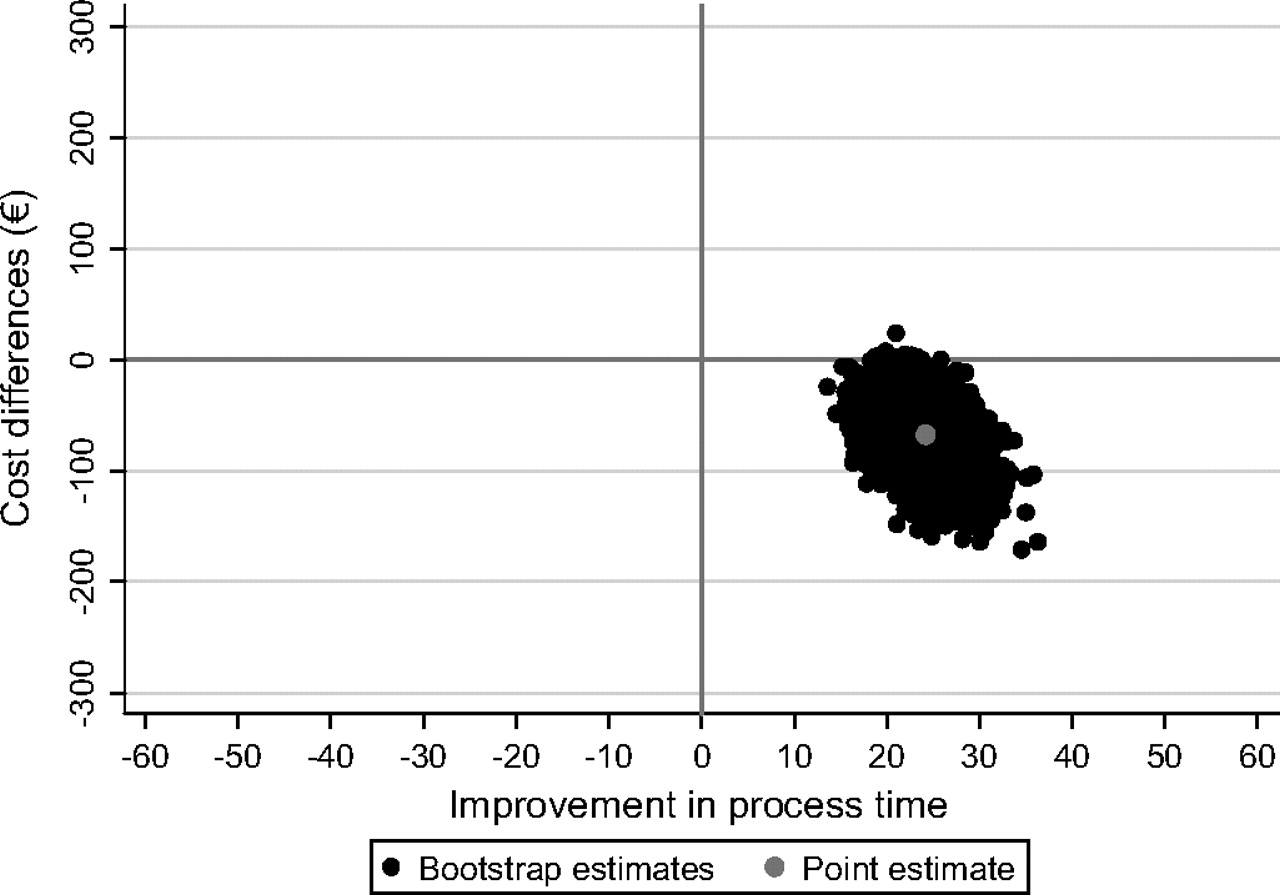
Cost-effectiveness plane for process time (new care method versus usual care method).

{kind=link}
{kind=link}
Cost-effectiveness acceptability curve for process time (new care method versus usual care method).
For patient satisfaction, results were similar: almost 100% of the bootstrapped cost–effect pairs was situated in the southeast quadrant of the cost-effectiveness plane and the probability that the new care method is cost-effective in comparison with usual care was 1 for all possible ceiling ratios (data not shown).
For the number of correct diagnoses, results were slightly different. Around 12% and 88% of the bootstrapped cost–effect pairs were lying in the southeast and southwest quadrant, respectively. This confirms the finding of a non-significant difference in the number of correct diagnoses that is accompanied by significantly lower costs. The cost-effectiveness acceptability curves showed that the probability that the new care method is cost-effective in comparison with usual care was larger than 0.95 for ceiling ratios ranging from €0 to €1363 (data not shown).
Discussion
In this study, we evaluated the cost-effectiveness of involvement of a GP in an AED department (new care method) with usual practice (usual care method) at a busy AED department using a before after design. Our results show that the new care method resulted in significantly lower process time, significantly higher patient satisfaction and significantly lower costs, while there was no difference in the number of correct diagnoses between the two methods. The new care method was considered cost-effective in comparison with the usual care method for all outcomes measures used.
To our knowledge, this is the first cost-effectiveness study of involvement of a GP in an AED. Our study is in line with earlier studies that also showed that management of patients with primary care needs in AEDs by GPs reduced costs,10 11 but these studies did not relate patient outcomes to costs in a formal cost-effectiveness analysis.
There are a number of limitations to this study. First, it was not possible to conduct a randomised controlled trial in the busy setting of an AED, because this would have disturbed daily practice in an unacceptable way. Although a randomised controlled trial is the most appropriate design to demonstrate cost-effectiveness, we tried to limit bias as much as possible. By using a before/after design there was no contamination possible between the two care methods. In both time periods the percentage of eligible and unwilling patients was comparable. More importantly, there was no difference in baseline characteristics between patients in the new care period and patients in the usual care period. Second, the GPs working at the AED were supernumerary to the regular AED staffing. This in itself may have lead to decreased process time. However, the decrease was 25 min, which is larger than the reduction that can be expected by the addition of a GP to the regular staff. The reduced process time may also have increased patient satisfaction in the new care period. However, not only were waiting times reduced, but treatment times were also reduced when a patient was treated by the GP. Therefore, it is realistic to assume that even when the GP is not supernumerary, some time can be gained. Third, additional investigations and procedures requested at the AED were valued using costs from the hospital financial administration. Therefore, the generalisability of these cost data may be limited. However, we do not expect costs to differ greatly between hospitals.
An important strength of this study is the large number of patients that was included. Although we did not have complete follow-up for all outcome measures, follow-up rates were adequate. Moreover, cost data were complete. Another strength is that the use of a before/after design ensured that the study was conducted in a pragmatic fashion. Although process times may be somewhat longer when a GP replaces a member of the AED staff, we think that this study gives a good estimate of the true effect and cost consequences of involvement of a GP in the AED. Finally, in this study we not only included costs of investigations and procedures in the hospital, but we also valued time spent by patients on visiting the AED and treatments planned after discharge from the AED. In contrast, earlier studies only included the use of hospital resources.10 11
In conclusion, this study shows that involvement of a GP in the AED is cost-effective in comparison with usual care at the AED. Since earlier research has shown that interventions aimed at changing patient behaviour are not particularly effective,5–8 future research should focus on integration of primary care in the AED. Employment of a GP in the AED is a cost-effective option as shown by this study, but it is unclear whether these benefits can also be seen in other AEDs. The benefits may be smaller in rural areas where people have to travel longer to reach an AED. Another promising means to organise emergency care more efficiently is the integration of GP cooperatives for out-of-hours primary healthcare and AEDs.21 Further research is needed to clarify these issues.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Human Medical Ethics Committee (METC) of the VU University Medical Center, Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey