Article Text

Abstract
Introduction Compared with heterosexual, cisgender populations, sexual and gender minority (SGM) people are more likely to suffer from serious health conditions and insufficient access to health services. Primary care is at the frontlines of healthcare delivery; yet, few clinics have resources or mechanisms in place to meet SGM patient needs. This developmental study protocol focuses on reducing health disparities among SGM patients by identifying, adapting and developing SGM practice guidelines/recommendations and implementation strategies for primary care clinics in urban and rural New Mexico. Using input from patients, healthcare advocates and providers, and researchers, the study will pilot a practice parameter and implementation toolkit to promote SGM-specific cultural competence at multiple service delivery levels.
Methods and analysis We will recruit providers/staff from four Federally Qualified Health Centers (FQHCs) serving ethnically and geographically diverse communities. Incorporating the Implementation of Change Model and an intersectionality perspective, data collection includes a systematic review of SGM-specific practice guidelines/recommendations, focus groups and semistructured interviews, quantitative surveys and the Nominal Group Technique (NGT) with providers/staff. We will categorise guidelines/recommendations identified through the review by shared elements, use iterative processes of open and focused coding to analyse qualitative data from focus groups, interviews and the NGT, and apply descriptive statistics to assess survey data. Findings will provide the foundation for the toolkit. Focus groups with SGM patients will yield supplemental information for toolkit refinement. To investigate changes in primary care contexts following the toolkit’s pilot, we will undertake systematic walkthroughs and document review at the FQHCs, analysing these data qualitatively to examine SGM inclusiveness. The structured data-informed Plan-Do-Study-Act method will enable further revision of the toolkit. Finally, focus groups, interviews and quantitative surveys with providers/staff will highlight changes made in the FQHCs to address SGM patient needs, barriers to sustainment of changes, satisfaction, acceptability, usability and feasibility of the toolkit.
Ethics and dissemination The study has been reviewed and approved by the Pacific Institute for Research and Evaluation Institutional Review Board. Informed consent will be obtained from all participants before their involvement in research activities begins. Study results will be actively disseminated through peer-reviewed journals, conference presentations, social media and the internet, and community/stakeholder engagement activities.
- cultural competency
- health status disparities
- implementation science
- minority health
- primary health care
- sexual and gender minorities
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- cultural competency
- health status disparities
- implementation science
- minority health
- primary health care
- sexual and gender minorities
Strengths and limitations of this study
This developmental study addresses healthcare disparities among sexual and gender minority (SGM) populations as guided by a Scientific Advisory Board of SGM patients, healthcare advocates and providers, and researchers.
The study facilitates an examination and prioritisation of organisational and clinical practice guidelines, resulting in a triangulated and analysed set of guidelines approved by a diverse group of stakeholders representing SGM communities and healthcare advocates and providers.
The prioritised guidelines and practical implementation strategies will be integrated into a comprehensive user-friendly toolkit.
The study will explore implementation strategies to introduce the toolkit into primary care practices, and advance pragmatic recommendations for improving services for SGM people from the perspectives of FQHC providers, staff and patients.
The study is limited to four FQHCs in a single state, which may limit generalisability of findings and the toolkit; the small sample sizes also preclude implementation of a randomised controlled trial design to assess organisational and practice changes enabled by the toolkit.
Introduction
Reducing health disparities for sexual and gender minority (SGM) populations, including persons who are lesbian, gay, bisexual, transgender and/or queer (LGBTQ), is a public health priority in the USA.1–3 Compared with heterosexual, cisgender people, SGM individuals are more likely to suffer from poorer mental health, substance misuse, inadequate diet and exercise, and sexually transmitted infections that are often first identified in primary care.4–7 They are also less likely to access preventive services, cancer screening and treatment for cardiovascular disease, diabetes, hypertension and other serious conditions.1 5 6 8 9 Many experience ‘minority stress’ from chronic exposure to stigma and discrimination.10 11 Intersecting minority identities may compound these effects, disproportionately impacting gender-diverse persons,12 ethnic and racial minorities,13 individuals of low income or educational attainment,14 15 and rural residents.16 17
Health disparities for SGM people are deepened by ongoing provision of suboptimal services in healthcare systems with histories of promoting stigma around sexuality and gender atypicality (eg, denying services to persons with HIV/AIDS or who are transgender, conversion therapies).1 6 18–22 Stigma denigrating sexual/gender difference enables discriminatory attitudes and behaviour among healthcare providers/staff that contribute to minority stress.23 Persons suffering from minority stress may internalise anti-SGM sentiment, accept discrimination and microaggressions, and anticipate recurrence of negative experiences.10 11 24 Minority stress may lead to perceptions of provider bias or incompetence, inhibiting patients from revealing SGM status and health risk behaviours.25
Primary care, particularly in Federally Qualified Health Centers (FQHCs), is an ideal target for SGM healthcare intervention due to its person-centred approach, the access it offers to patients of varied social backgrounds,26 and the prevention, screening and treatment services it affords to patients across their lifespan.27–29 Yet, primary care often lacks sufficient resources or mechanisms to ensure that practice settings and service delivery are attentive to SGM patients.30 31 Environmental/structural elements (eg, décor, forms, mission statements) contribute to SGM invisibility, and staff attitudes, language and behaviours may exacerbate feelings of marginalisation.30–34 Insufficient SGM-specific competence among providers inhibits disclosure of SGM status in clinical encounters, undermining patient satisfaction.35 This invisibility can underpin provider beliefs that SGM status is unimportant to patients. Failure among providers to ask relevant questions in attempts to present neutral attitudes towards SGM patients36 37 may also factor into misdiagnoses of health concerns, ineffective treatment and subpar care.38 39 Adequate medical education/training on SGM care is also wanting.40 41
Implementing practice guidelines for SGM competent care that draw from national policies, recommendations for SGM-inclusive medical education curricula42–45 and organisational contexts is imperative to rectify these gaps at provider/staff, practice and service-system levels.8 31 33 46 Although current guidelines/recommendations (henceforth ‘guidelines’) contain critical information about SGM patient-centred clinical environments and interactions, they are fragmented, not based in primary care research, and neglect population-based intersectional attributes (eg, race/ethnicity, culture, rurality) and input from both service providers and SGM patients.31 While a 2010 systematic review identified six philosophically and practically consistent guidelines for SGM patient care (table 1), they lack sufficient evidence and mechanisms for implementation in primary care.31 Such findings for patient care were reproduced in a 2018 review,47 and a 2017 review found no articles evaluating organisational change for care of SGM people.42 This study responds to these gaps, as its goals include (1) developing and triangulating clinical and organisational SGM practice guidelines that can be feasibility implemented in primary care; (2) curating a practice parameter and implementation toolkit by collaborating with providers/staff and SGM patients; and (3) creating measurable implementation strategies and resources to integrate guideline-specific and tool-specific innovations to enable organisational and practice change in primary care for SGM individuals.48
Synthesised recommendations for primary care from existing guidelines appraised by McNair and Hegarty
Study aims
Participatory methods are critical to evaluating guidelines and implementation strategies to improve primary care for SGM people.49 This developmental study attempts to reduce SGM disparities by partnering with FQHCs in the majority–minority state of New Mexico (NM). We will employ the Nominal Group Technique (NGT), an efficient participatory priority-setting process,50 51 to ground SGM practice guidelines in primary care and advance theory-based implementation strategies to promote guideline adherence. Providers/staff from four FQHCs will deploy the Plan-Do-Study-Act (PDSA) approach to pilot the toolkit.52–55 The Implementation of Change Model (IoCM)56 and an intersectionality lens1 57–59 will assist in developing implementation strategies that are optimally relevant to local communities.60 Both perspectives thus comprise the conceptual basis for data collection, guideline adoption and implementation strategy development and testing. This study has three specific aims:
Prioritise SGM practice guidelines and adapt and develop implementation strategies for primary care settings with attention to the intersections of race/ethnicity, rurality and socioeconomic conditions.
Develop/refine a comprehensive toolkit of SGM practice guidelines and implementation strategies to provide FQHCs with resources to promote and evaluate SGM-specific competence at multiple service delivery levels.
Evaluate toolkit implementation at (1) individual provider/staff, (2) social/practice setting and (3) organisational context levels in supporting SGM-specific primary care in FQHCs.
This study responds to national calls to address SGM health disparities by spearheading an approach to implement critical and feasible primary care practice guidelines to promote the well-being of SGM patients with intersecting minority identities.1–3 It also responds to research priorities in the USA to enhance SGM health in under-resourced, understaffed primary care clinics that are stretched to form a crucial safety net.2 61–63 Finally, the study is an essential start for continued research using a type 2 hybrid effectiveness-implementation design for dual testing of the effectiveness of SGM guidelines and implementation strategies specific to primary care.64 65
Methods
Study design and overview
This study features a systematic review of guidelines for SGM-inclusive culturally competent primary care, focus groups and semistructured interviews, quantitative surveys and use of the NGT to facilitate uptake of SGM practice guidelines in primary care. Our 10-person Scientific Advisory Board (SAB), a panel of SGM patients, healthcare advocates and providers, and researchers, will play critical roles in interpreting data from these sources and creating the toolkit. Our study has two phases. Phase 1 engages the SAB and providers/staff from the participating FQHCs in prioritising/assessing guidelines and implementation strategies (aim 1) for the toolkit (aim 2). Phase 2 (aim 3) pilots the toolkit in FQHCs to obtain feasibility, acceptability, usability, fidelity and satisfaction data. The iterative nature of study findings allows for ongoing feedback from participants and accuracy checks to increase internal validity and credibility, reducing possibilities of biassing results.66 Participatory methods will enhance the toolkit’s relevance to a diverse clientele. Finally, implementation experts emphasise selecting or tailoring implementation strategies based on theory, barrier assessments or other rationale.67 This study will generate insights into implementation strategies to overcome barriers to toolkit adoption for different settings and stakeholders.67 68 A timeline of study activities appears in table 2.
Timeline of study activities by quarter
Patient and public involvement
This study protocol emerged through a lengthy SGM patient and participant engagement process initiated in 2014 with funding from the Patient-Centred Outcomes Research Institute. With this funding, we conducted a series of town hall meetings with SGM people in ethnically and geographically diverse regions of NM regarding their health and healthcare needs. We then developed a statewide SGM health collaborative of SGM patients, healthcare advocates and providers, and researchers to analyse findings from these meetings. This collaborative next created a research agenda for improving SGM healthcare and organised a series of now annual SGM health summits that allow for broader patient and public input into this agenda.
Findings from the town halls and the collaborative’s deliberations led to the identification of primary care as a key site for research-based intervention,35 particularly in rural and otherwise medically underserved communities, and to development of participatory procedures for conducting health-related research with SGM populations.69 The collaborative also identified two major barriers limiting the capacity of primary care clinics to improve services for SGM patients: (1) lack of comprehensive sets of guidelines based in primary care research; and (2) insufficient implementation supports (eg, access to education, training, data on SGM patients) that might assist providers/staff in bustling yet under-resourced clinics in taking part in organisational change efforts to advance quality care for SGM patients. Of note, patients in the SGM health collaborative and/or attending the summit have also provided critical feedback into the design of this study protocol, sharing their ideas for recruitment and the overall conduct of this research. Convening the SAB represents step 1 of our conceptual model; patients on the SAB will continue to offer feedback into study instrumentation, interpretation of findings and dissemination strategies. We will share research results with patients and study participants through online briefs, the annual summit and on-site presentations in communities where the participating FQHCs are located.
Conceptual framework
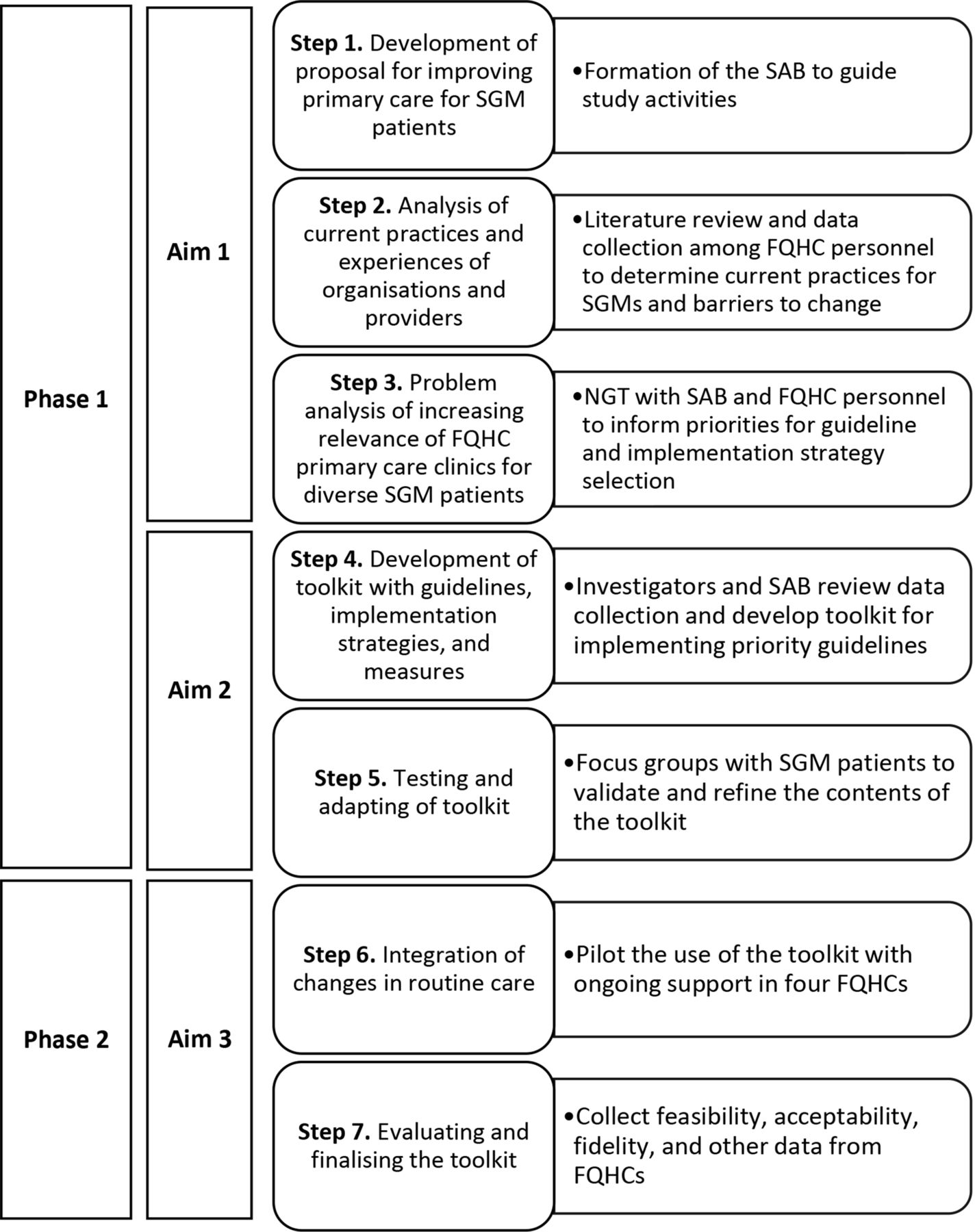
Implementing innovations, including guidelines and toolkits, in primary care is complex. We will draw from the IoCM56 and use an intersectionality lens1 57–59 to prioritise/assess guidelines and incorporate targeted implementation strategies to aid their translation into everyday clinical work. The IoCM (figure 1) is a systematic approach to plan, organise and implement change, and considers a range of factors impacting implementation.56 For example, an FQHC’s climate and organisational capacity can affect the willingness of providers/staff to engage in new practices,70 as do their individual characteristics (eg, job tenure, professional development level).71 Leadership is also key.72 Persons leading implementation must be effective change agents; their ability to motivate and interact with employees shapes provider/staff attitudes towards new practices.73 Addressing readiness to change, provider/staff attitudes (eg, SGM-negativity) and misinformation,74 and engaging FQHC workers as agents of change via the IoCM will allow them to emerge as champions in deepening capacity to improve primary care for SGM patients.
{kind=link}
Adapted implementation of change model by study phase, aim and step. FQHC, Federally Qualified Health Center; NGT, Nominal Group Technique; SAB, Scientific Advisory Board; SGM, sexual and gender minority.
Given our focus on intersectionality, we recognise that gender and sexuality are only two of several factors affecting the social identities, circumstances and health/healthcare outcomes of SGMs.1 58 59 Data collection, analysis and toolkit planning must thus consider the racial/ethnic, socioeconomic and geographical diversity found in places like NM, where structures of oppression and privilege beget unequal healthcare opportunities for specific populations.58 75 By integrating the IoCM and intersectionality theory, this study is among the first to move beyond assessing SGM healthcare needs and barriers to developing and testing strategies based on understanding the particular experiences of provider/staff and patients of multiple minority statuses, and both organisational and worker capacity to implement innovations in primary care.76
In addition to the IoCM and an intersectionality perspective, we turn to theories of change in public health (table 3)77 and data from the systematic review, qualitative focus groups/interviews, surveys and the NGT to design implementation strategies targeting multiple healthcare levels: (1) individual provider/staff (eg, knowledge, attitudes); (2) social/practice setting (eg, teamwork, opinion leaders, leadership); and (3) organisational context (eg, administrative, structural and cultural factors shaping the workplace).77 78 With the SAB and FQHC stakeholders, we will consider relevant change theories to articulate both rationale and processes by which the strategies will lead to greater SGM competence and higher quality care for SGM patients.
Sample theories of change based on the IoCM to inform SGM practice guideline implementation strategies
Study context
Our setting is NM, a state ranking 47th in median household income,79 with the second largest percentage of residents below the poverty level (19.7%).80 Hispanic/Latinx and Native American people are 60% of residents.81 About 3% of adults82 and 15.1% of high-school students identify as sexual minorities83; 0.75% of adults84 and 3.4% of high-school students identify as gender minorities.85 Access barriers and cultural competence deficits in care contribute to SGM health disparities.35 82 86 Aims 1 and 2 involve participants from two rural and two urban FQHCs serving racial/ethnic minority communities. Because numerous health disparity populations (eg, Hispanic/Latinx, Native American, socioeconomically disadvantaged, rural) are key FQHC consumers, our study’s FQHC context supports wider applicability to intersectional SGM people.
FQHC samples and recruitment
We will use purposive sampling to represent the range of views/experiences of individual and organisational factors related to prioritising/assessing and implementing guidelines.87 We will include six to eight providers/staff per focus group at each FQHC; one to three clinic administrators per FQHC will take part in interviews. We will work closely with clinic administrators to recruit FQHC employees for the on-site focus groups/interviews. Clinic administrators will advertise focus groups/interviews on FQHC listservs and in employee common areas. Our team will present the study purpose and design at staff meetings. Recruitment may attract persons already sensitive to issues in SGM care; however, these sensitivities may also heighten their ability to perceive and discuss issues in SGM care. Thus, such sensitivities will neither negate their advice for introducing and enacting the guidelines in primary care nor perceptions of implementation barriers/facilitators. Eligible providers/staff must have worked at the FQHC for one or more year(s) for an average of at least 20 hours per week to ensure familiarity with clinical procedures and context-specific healthcare needs. Eligible administrators include persons responsible for professional leadership and the overall management and operation of the FQHC. We will recruit a subset of this sample of FQHC personnel for the NGT, as described below. Following the NGT, we will work with the SAB to develop our toolkit, which will be presented to two additional focus groups (one rural, one urban) of six to eight SGM patients recruited from the FQHC catchment areas. Inclusion criteria include being age ≥18, self-identifying as SGM, and service utilisation at the FQHC in the past 5 years. The challenges of research with SGM people include lack of identification with externally imposed social categories (eg, gay, transgender), and the problem of recruiting ‘hidden’ populations for studies on sensitive topics.88 89 We will deploy purposive sampling methods to overcome these challenges: (1) snowballing (members of the population of interest link researchers with candidates); (2) outcropping (soliciting candidates at places they are known to frequent); and (3) advertising (newspapers, websites).88
Data collection
Document reviews/systematic walkthroughs (phase 1; aim 1; IoCM step 2)
We will analyse documentation to assess for changes in organisational context related to SGM inclusiveness at baseline and on piloting the toolkit (aim 3). Documents of interest are derived from the Healthcare Equality Index (HEI), a national benchmarking tool used in over 1600 healthcare facilities to evaluate policies/practices related to equity and inclusion of SGM patients, visitors and employees.90 Documents requested of clinic administrators will be compiled into an inventory, and analysed using HEI scoring criteria that centre on (1) employment non-discrimination/staff training, (2) patient services/support, (3) employee benefits/policies and (4) patient/community engagement.91 Two researchers will also apply a checklist based on the criteria of the Gay and Lesbian Medical Association during systematic walkthroughs of the FQHCs to observe evidence of visual clues, or décor, suggesting the site is safe for SGM patients, that is, public display of non-discrimination statements and SGM-oriented brochures, educational materials and posters.92 The walkthroughs will also address whether visual clues pertain to patients of intersecting identities in FQHC catchment areas.
Systematic review of SGM-specific guidelines (phase 1; aim1; IoCM step 2)
Our systematic review of the literature will lend insight into current guidelines for culturally competent primary care for SGM patients. We will consult with academic librarians and the SAB to identify appropriate terms and databases for the review. The databases will likely include: CINAHL, PsycARTICLES/PsycINFO, Mental Measurements, SPORTDiscus, SocINDEX, PubMed/MEDLINE, Web of Science and Cochrane Collaboration. We will employ two searches, each consisting of three sections of keywords (see online supplementary file for a detailed list of possible search terms). For the first search, the sections will comprise keywords identifying SGM populations, keywords pertaining to primary care medical services and keywords concerning guidelines and recommendations. We will limit the keyword search to only abstracts and keywords, exclusively English-language results and without restriction of publication date. After this first search, we will conduct a second search, expanding to all healthcare settings, rather than narrowly focus on primary care, as helpful practice guidelines for culturally competent care for SGM patients may present in other service milieus. We will undertake this second search using the same three sections of keywords and criteria used in the first search. We will perform the first search over a 2-month period; the second search will occur over 1 month. On completing the searches in each database, we will import all results into EndNote X8 and cull duplicates.93
Supplemental material
We will review the titles/abstracts, then full texts, of the publications iteratively, removing those not meeting inclusion criteria and inputting the remaining texts into an Excel worksheet. Multiple content experts will independently review each guideline to identify major thematic areas. They will convene regularly to agree on the content of thematic areas, assigning each guideline into these areas. The full study team will review the exhaustive list of guidelines, eliminating redundancies for condensation purposes. Each included publication will be rated on the extent to which it meets criteria across multiple domains encompassing scope/purpose, stakeholder involvement, rigour of development, conflict of interest, external review and clarity of presentation.31 47 The shortened list will be presented to the SAB wherein we will gather member perceptions regarding the importance of, and feasibility of, implementing the items it contains.
FQHC focus groups/interviews with surveys (phase 1; aim 1; IoCM step 2)
We will assess current practices/experiences of FQHC stakeholders related to primary care for SGM people. Participants will complete brief (20 min) surveys prior to focus groups/interviews on individual, social/practice setting and organisational factors relevant to implementing guidelines.94 The measures include: Attitudes toward Lesbians and Gays Scale (α>0.80)95; Bisexualities: Indiana Attitudes Scale (α=0.91)96; Attitudes toward Transgender Individuals Scale (α=0.95)97; Lesbian, Gay, Bisexual, and Transgender Development of Clinical Skills Scale (a=0.86)98; Context (α=0.85, eg, culture, opinion leaders) and Facilitation (α=0.95, eg, senior leadership, leadership implementation) modules of the Organisational Readiness to Change Assessment 99; Implementation Climate Scale (α=0.91)100; and the Evidence-Based Practice Attitude Scale (α=0.76).101 102 The focus groups/interviews will pose open-ended questions to study in-depth organisational attributes of FQHCs and attitudinal factors, behaviours and experiences at varying levels affecting SGM care.78 Questions will centre on general knowledge/experience with SGM patients, adopting guidelines in primary care, and implementation barriers/facilitators. By tapping into provider/staff and administrator perspectives, we can understand how different levels (eg, provider/staff, social and practice setting, organisation) align to ensure optimal care for SGM people, enabling us to identify targets for and potential impediments to practice innovation. The 60-min to 90-min focus groups/interviews will be digitally recorded, transcribed and reviewed for accuracy.
Qualitative/quantitative data analysis (phase 1; aim 1; IoCM step 2)
We will import transcripts into a password-protected NVivo V.12 database for iterative analysis, first using open coding to locate themes/issues, assign codes to segments of text based a priori on topics in the focus group/interview guides, and identify and define new codes.103–105 We will also create codes based on key sensitising concepts from intersectionality theory (eg, intersecting identities, structural factors)57–59 106 and implementation science (eg, leadership, climate)94 107 that help establish ‘a general sense of reference’ for analysis.66 Second, we will use focused coding to discern codes that recur or represent unusual issues.104 105 We will cross-reference statements of interest (eg, text coded with ‘welcoming environment’ and ‘discrimination exemplar’”) to ascertain relationships in data both in and across FQHCs, and group codes with similar content into broad themes linked to retrievable text segments.104 108 We will enter the survey data into the Statistical Package for the Social Sciences V.25(SPSS) for descriptive analyses aggregated at the FQHC level,109 comparing qualitative and survey data across organisations to ascertain areas of strength and weakness regarding factors likely to affect guideline implementation in primary care. Products will include a summary of key issues to consider in prioritising/assessing guidelines and jumpstarting implementation strategy development via the NGT.
Nominal Group Technique (phase 1; aim 1; IoCM step 3)
After developing a list of guidelines and implementation strategies from the empirical literature and focus groups/interviews, we will use the NGT to prioritise them. The NGT has been fruitfully applied in direction setting in health services research and implementation science.50 110 111 The NGT convenes small groups of diverse stakeholders to generate ideas, develop consensus and set priorities for standards or guidelines, particularly in situations where the research base is inconclusive.51 110 While the NGT occurs in groups, emphasis is less on sample size and more on involving people of different roles/social locations to ensure heterogeneity of viewpoints.50 111 We will use the NGT to prioritise strategies to implement the guidelines, inviting a subset (n=8–12) of focus group/interview participants to a 2-hour NGT session held in a central location. Participants will be given the list and preprinted ‘Nominal Group Task Statement Forms’ specifying exploratory questions resembling: (1) “What are likely the most impactful and feasible guidelines or recommendations to improve care for your SGM patients?” (2) “List the strategies or steps that would best help your organisation implement and sustain guidelines and recommendations to improve care for SGM patients.” Participants will have the opportunity to select, adapt and suggest additional guidelines or implementation strategies for toolkit inclusion. They will first independently strategise in silence, then engage in a serial discussion of each idea, group ranking and vetting of priorities, and re-ranking until reaching consensus using the 70/30 consensus voting procedure that entails respectful conversation of dissenting opinions.112
Toolkit development and refinement (phase 1; aim 2; IoCM step 4)
Focus group/interview, survey and NGT data will inform the integration of existing guidelines with implementation strategies into the toolkit (table 4), with increased attention to issues of organisational context and intersectionality.1 58 59 We will work with the SAB to refine the toolkit and develop fidelity measures by reviewing outlines for each module and arriving at agreement via the 70/30 consensus method.112 We will draft easy-to-follow materials and procedures to promote change in healthcare and policies concerning SGM patients of multiple minority statuses using accessible language and drawing on examples from the above research to illustrate potential barriers/facilitators to change at the individual, social/practice setting and organisational levels. For each module, we will include tools to assess attitudes, practices and competencies; select implementation strategies to match the local context; develop feasible priorities and goals; create action plans; and then evaluate progress towards goals.
Preliminary outline of the comprehensive toolkit
SGM patient focus groups (phase 1; aim 2; IoCM step 5)
Patient input is essential to interventions to improve primary care for SGMs.69 Community perspectives and community-identified competencies, such as being comfortable with SGM patients and shared medical decision-making between providers and patients, improve care by ensuring that community member priorities are not neglected. Community input is also crucial to determining the expertise that providers/staff may require to best care for diverse SGM patients, many of whom can articulate their experiences of minority stress in healthcare encounters.113 For this study, two focus groups (one rural, one urban) of six to eight SGM patients of varying races/ethnicities from the FQHC catchment areas will provide feedback into the toolkit’s validity and refinement. Participants will be given a copy of the toolkit to review prior to the focus group. During the first 20 min of the group, they will draft a list of toolkit gaps, acceptability and strengths/limitations. Questions asked subsequently will centre on these issues, experiences with primary care and the extent to which the toolkit addresses issues of race/ethnicity, culture, rurality and other intersections of SGM population attributes. We will analyse transcripts using the procedures described above, sharing results with the SAB to update the toolkit prior to piloting. Finally, we will share the toolkit with FQHC participants for final input before testing begins.
Toolkit pilot test (phase 2; aim 3; IoCM steps 5–7)
The FQHCs will implement the refined toolkit with ongoing coaching and assessment over 1 year. An SGM-specialist coach who is well-versed in the toolkit will meet with each FQHC’s leadership to develop an implementation resource team (IRT) that meets monthly to develop goals and action plans and monitor progress in carrying out the prioritised guidelines and implementation strategies using the PDSA method, a four-stage cyclic, iterative learning approach to test a change implemented in a clinical milieu.52–55 The IRTs are small stakeholder groups of three to five persons that will lead integration of guidelines into routine care, and may include clinic administrators, providers/staff and patient advocates. Per the first cycle—Plan—the IRT drafts a concise statement regarding a guideline to put into practice, and then an action plan describing the goal/outcome to accomplish via this guideline and associated measures. The IRT articulates the implementation strategies or steps to promote adoption of the guideline, while establishing a relatively short-term timeline for completion. For the second cycle—Do—the IRT sets the action plan into motion, observing, collecting data and documenting what happens when the strategies are executed. During this cycle, the IRT asks, “Did everything go as planned?” and determines whether the plan must be modified.54 During the third cycle—Study—the IRT examines the results of its efforts, identifying lessons learnt, whether the goal/outcome was attained with fidelity to the action plan and how well the implementation strategies worked. For the fourth cycle—Act—the IRT delineates its conclusions regarding the success of the change, clarifying what worked and did not work, and what it may do differently to facilitate productive implementation, as well as potential adaptations and next steps for scale up or a new cycle.54 55
We do not expect FQHCs to move forward with all guidelines in the toolkit at once, but to evaluate its content and proceed to implement guidelines incrementally via the PDSA method, improving on efforts to advance SGM practice changes with each successive cycle. The IRTs will also examine implementation needs and troubleshoot barriers using PDSA planning templates included in the toolkit. Thus, for instance, an IRT wanting to include SGM data in an FQHC’s electronic health record system might focus on empowering hesitant providers/staff to ask relevant questions of patients or revise patient intake forms with non-stigmatising elicitation terminology. The toolkit will include guidance and model examples related to these and other topics.
The IRTs will facilitate team collaboration to instantiate new practices and will benefit from the implementation strategy of coaching when applying the toolkit.114 115 The SGM-specialist coach will strive to build confidence in IRT members during the PDSA process, emphasising how to motivate positive behaviour change among FQHC stakeholders to foster successful implementation and fidelity or adherence to guidelines included in the toolkit.116–119 For action planning, the coach can advise on prioritising guidelines and using theory-based implementation strategies via toolkit materials (eg, assessments, checklists and examples).120
We will evaluate guideline implementation progress by undertaking walkthroughs in each FQHC and collecting and analysing minutes from (1) IRT meetings, (2) copies of completed action plans and fidelity measures in the toolkit and (3) and other organisational context documentation (eg, intake forms, brochures, policies at start and when changed). We will administer a final round of focus groups/interviews with providers/staff and administrators of each FQHC using the same sample sizes and procedures described earlier, focusing on toolkit implementation at (1) individual provider/staff, (2) social/practice setting and (3) organisational context levels. A complementary set of small group interviews with IRT members will examine changes made to address SGM patient needs, barriers to sustainment, as well as toolkit satisfaction, acceptability, usability and feasibility.121 More specifically, questions asked in focus group/interview formats will centre on how use of the toolkit influences care for SGM patients, its contributions to patient and provider/staff satisfaction, difficulties involved in applying the toolkit in real-world practice, constraints experienced by the organisation and providers/staff during implementation, overall utility and ease of employing featured implementation strategies, and the range of positive and negative factors ultimately affecting the toolkit’s uptake and perceived impacts. These data will inform final revisions to the toolkit to be agreed on by the SAB.
Limitations
The study is limited to four FQHCs in a single state, which may limit generalisability of findings and the toolkit. The purposeful sampling strategy may lead to an over-representation of clinic personnel concerned about care for SGM patients, or with vested interests in portraying themselves and the FQHCs positively. The small sample sizes also preclude implementation of a randomised controlled trial design to assess organisational and practice changes resulting from the toolkit.
Ethics and dissemination
The Pacific Institute for Research and Evaluation Institutional Review Board has reviewed and approved the study’s procedures. All FQHC employees who take part in data collection activities, such as a focus group, interview, or an NGT session, will sign an informed consent form prior to their participation. The consent form will explain that the information they share will remain confidential and will not be disclosed with anyone outside the research team. Participants will be randomly assigned identification numbers to assure confidentiality and reminded that they can leave the study at any time and for any reason without penalty. Results and products from this study will be disseminated via local/state/national presentations and peer-reviewed publications, and through social media and community/stakeholder engagement activities.
Next steps and dissemination
After advancing SGM practice guidelines, implementation strategies and indicators of guideline/implementation fidelity, we are planning a future study with a hybrid type 2 effectiveness-implementation experimental design and a larger number of FQHCs.64 65 We will assign FQHCs to (1) guidelines without implementation support, (2) guidelines with implementation support, (3) services as usual without implementation support and (4) services as usual with implementation support. Both studies will provide methods to transform how FQHCs care for racially, ethnically, socioeconomically, and geographically diverse SGM patients.
Acknowledgments
We thank the members of the New Mexico LGBTQ Health Collaborative for making this research possible, namely, Molly Adler, Cameron Crandall, Rebecca Dakota, Paige Duhamel, Edward Fancovic, Jamie Finkelstein, Jonathan Flores, Gregory Gomez, Beverly Gorman, Adrien Lawyer, Benjamin Moser, La Tisha Rico, Crystal Romney, Amber Royster, Denise Ruybal, Nathaniel Sharon and Alma Rosa Silva-Bañuelos. We also thank Patricia Hokanson for assistance with formatting the references.
References
Footnotes
Contributors CW, MK, AEG and RS initiated and conceived of the study in partnership with the New Mexico LGBTQ Health Collaborative. CW, MK and AEG drafted the research protocol and overall study design. MS developed the systematic review protocol. RS, SD and KE reviewed and critically revised the protocol. All authors approved the final version of this protocol.
Funding This work was supported by a grant from the US National Institute of Minority Health and Health Disparities (R21MD011648), and two Pipeline to Proposal awards from the Patient-Centered Outcomes Research Institute.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.