Article Text

Abstract
The COVID-19 pandemic is considered a mass casualty incident of the most severe nature leading to unearthed uncertainties around management, prevention, and care. As of July 2020, more than twelve million people have tested positive for COVID-19 globally and more than 500 000 people have died. Patients with diabetes are among the most severely affected during this pandemic. Healthcare systems have made emergent changes to adapt to this public health crisis, including changes in diabetes care. Adaptations in diabetes care in the hospital (ie, changes in treatment protocols according to clinical status, diabetes technology implementation) and outpatient setting (telemedicine, mail delivery, patient education, risk stratification, monitoring) have been improvised to address this challenge. We describe how to respond to the current public health crisis focused on diabetes care in the USA. We present strategies to address and evaluate transitions in diabetes care occurring in the immediate short-term (ie, response and mitigation), as well as phases to adapt and enhance diabetes care during the months and years to come while also preparing for future pandemics (ie, recovery, surveillance, and preparedness). Implementing multidimensional frameworks may help identify gaps in care, alleviate initial demands, mitigate potential harms, and improve implementation strategies and outcomes in the future.
- diabetes mellitus, type 2
- diabetes complications
- delivery of health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/ .
Statistics from Altmetric.com
Introduction
The emergence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus and the resulting COVID-19 pandemic is considered a mass casualty incident of the highest nature and is associated with newly unearthed uncertainties around management, prevention, and care.1 As of July 10, 2020 more than twelve million people have tested positive for COVID-19 globally.2 Over 3 million cases have been detected in the USA, where more than 130 000 people have died.2 It is expected that many more people will contract the infection during the pandemic and potential new outbreaks are probable after initial lockdown measures are relaxed.3 Among those hospitalized with COVID-19, patients with diabetes are among the most severely affected.4–6 Questions are emerging related to the level of care patients with diabetes are receiving during this time.7–11 In the healthcare system, a lack of personal protective equipment (PPE) and the need to maintain glycemic control while reducing patient contact has led to urgent implementation of improvised protocols for inpatient treatment.11–13 Furthermore, the cancellation of non-emergent procedures and clinical appointments combined with a rapid transition to telemedicine for outpatient care have implications for diabetes care and outcomes. There are also limited data regarding the use of common diabetes medications for the management of those with diabetes and COVID-19 comorbidity, and there are likely to be long-term consequences of SARS-CoV-2 among patients with diabetes who contract the disease.
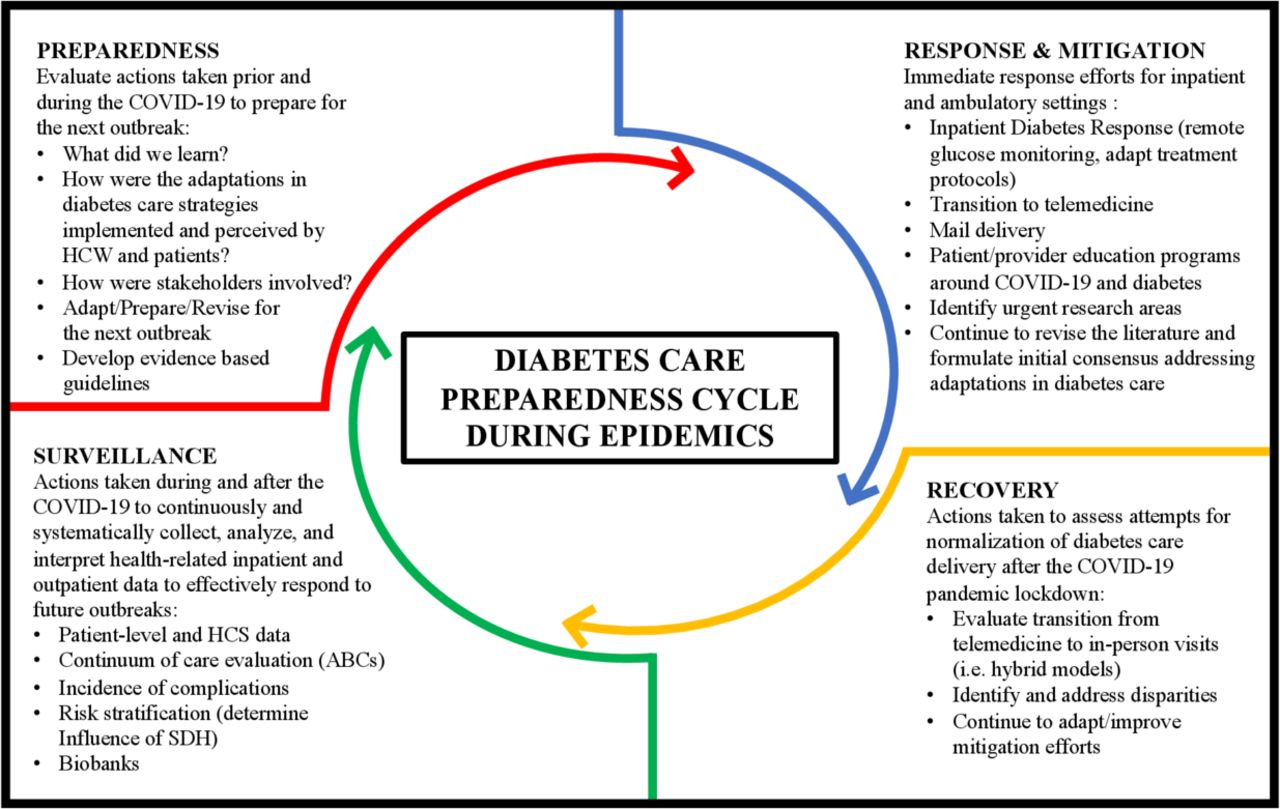
The COVID-19 pandemic has far-reaching political, economic, and social consequences.14 Therefore, we believe a rapid transformation of the approach to public health strategies, research, and clinical care for patients with diabetes, both during this pandemic and in future outbreaks, is needed. Adapting elements of the preparedness cycle, commonly used to address catastrophic natural disasters, acts of terrorism, or viral pandemics,15–19 we describe a framework for an immediate response to the current public health crisis as it affects those with diabetes. We present strategies that can involve multiple stakeholders (patients, healthcare workers (HCWs), researchers, payers, members of industry, and policy-makers) in the planning processes during current transformations in diabetes care in the immediate short term (ie, response and mitigation) and during the months and years to come while also preparing for future pandemics (ie, recovery, surveillance, and preparedness). Figure 1 illustrates the overlapping cycle phases and their corresponding strategies, presenting a long-term approach to strengthening pandemic preparedness for a comprehensive diabetes care response.

{kind=link}
Diabetes care preparedness cycle framework to address transitions in care during the COVID-19 pandemic and future outbreaks. ABC, A: hemoglobin A1c, B: blood pressure, and C: cholesterol; HCS, healthcare systems; HCW, healthcare worker; SDH, social determinants of health.
Response and mitigation
Large volumes of patients presenting to hospitals with COVID-19, overburdened HCWs, and the lack of healthcare resources have revealed vulnerabilities in the US healthcare system to adequately care for patients. Furthermore, the presence of diabetes presents additional challenges in thinking about the COVID-19 response. Urgent action to mitigate poor outcomes is therefore needed in both inpatient and outpatient settings.
Inpatient care
Prior to the COVID-19 pandemic, it was well established that inpatient hyperglycemia contributes to a significant increase in morbidity, mortality, and healthcare costs.20 Recent evidence clearly indicates that diabetes and hyperglycemia are associated with severity of disease and poor outcomes in patients with COVID-19.5 21–26 Therefore, glycemic control in those with diabetes and COVID-19 is paramount.11 27 28 Insulin therapy is commonly used in the hospital setting, and although US professional associations recommend insulin as the therapy of choice in the hospital, the use of non-insulin agents is not uncommon.29 Opinion-based recommendations suggest non-insulin agents should be implemented carefully in patients with diabetes and COVID-19.11 30 31 Standardized insulin regimens with multiple-dose injections are complex, require frequent point-of-care (POC) glucose testing, and are associated with iatrogenic hypoglycemia.29 In the intensive care unit, insulin therapy is even less convenient, with patients requiring hourly POC testing when treated with intravenous continuous insulin infusion.20 Therefore, to simplify therapy, preserve PPE, and limit bedside interactions, academic centers and hospitals around the nation are adapting their inpatient diabetes care strategies in response to COVID-19.12 To reduce interactions between patients and healthcare providers, limit exposure to COVID-19, and reduce the waste of PPE, the Food and Drug Administration (FDA) allowed the use of home-use blood glucose meters as an option to provide relief and support to healthcare professionals in the hospital.32 In addition, the FDA did not object to the use of continuous glucose monitoring (CGM) devices in this setting.11 Furthermore, both medical device companies Dexcom and Abbott have made efforts to supply CGM devices for emergent inpatient use, even though CGM has not yet been approved in this setting.11 Certain CGM devices, such as the Freestyle Libre (Abbott) or G6 (Dexcom), are factory-calibrated and do not require additional POC glucose testing to ensure accuracy in the outpatient setting. However, there is limited inpatient clinical experience with the two factory-calibrated CGM devices currently being implemented in hospitals to reduce bedside POC glucose monitoring.12
During the COVID-19 pandemic, it is also expected that patients with diabetes and COVID-19 comorbidity will experience an increase in diabetic ketoacidosis (DKA) and severe hyperglycemia, resulting in worse outcomes. Novel DKA management protocols have been suggested (www.covidindiabetes.org); however, the safety and efficacy of such protocols during treatment of DKA in patients with COVID-19 is unknown.11 33 Additionally, there is a lack of data reporting on how physicians are implementing, prioritizing, or relying on modified treatment protocols to guide diabetes-related therapy.12 Therefore, it is important that healthcare systems currently adapting protocols to monitor glucose levels or changing diabetes treatment strategies in COVID-19 units systematically evaluate the efficacy of these care adaptions considering quality improvement approaches centered in patients and HCWs.34
Outpatient care
Outpatient clinical practice has changed dramatically to minimize potential exposures to COVID-19 in patients requiring non-urgent medical care, especially those with medical comorbidities (including diabetes). There have been rapid and urgent shifts toward alternative methodologies for patient care, such as virtual encounters (video or phone), and shifts toward mail delivery of medications. However, these changes are being implemented without clear plans or directives for managing other comorbidities often associated with diabetes, such as hypertension and established cardiovascular disease (CVD). There has also been a push toward more patient self-managed care via online structured educational resources,13 yet the reach of such programs is not known. Prior to the COVID-19 pandemic, a meta-analysis including randomized controlled trials (RCTs) that compared telemedicine interventions with usual care found that systems allowing for medication adjustments with or without text messaging or a web portal improved glycated hemoglobin A1c (HbA1C) but not other clinically relevant outcomes in patients with diabetes.35 A more recent meta-analysis, including 42 RCTs (8 studies using teleconsultation and 34 using telemonitoring (device based)), including patients with type 1 and type 2 diabetes showed that telemedicine interventions were more effective than usual care in managing diabetes, especially in older patients with type 2 diabetes.36 However, a recent report indicates that the US healthcare system was not prepared to function under the constraints of lockdown measures related to COVID-19 and the subsequent return to in-person care. Although telehealth visits for diabetes care have increased modestly (~14%) during the COVID-19 pandemic, ambulatory visits remain 30% lower than previously.37
It is also unclear if patients have been able to access diabetes-related medications on time with adequate refills during the COVID-19 pandemic or if there has been an increase in urgent care visits to access medications during and after the initial lockdown. The overall reach of healthcare systems implementing mail orders for medication delivery is not known. Previous observational studies have suggested increased medication adherence in individuals with diabetes who obtained their medications by mail.38 39 Additionally, evidence also indicates that a telephone intervention led by a pharmacist and tailored to the individuals’ needs can significantly increase medication adherence in patients with long-term conditions including diabetes compared with usual care.40
Policy changes are needed to ensure that effective telemedicine capabilities are in place to reach all patients during potential lockdowns, regardless of the health system they attend. In addition, effective systems that ensure patients have access to their medications (ie, mail orders) during lockdowns are needed. Cost analyses of healthcare delivery strategies that incorporate care coordinators to help patients stay out of the hospital or interventions led by pharmacists to ensure appropriate medication supplies are necessary to determine their potential implementation, especially during public health crises requiring social distancing.
In addition, factors related to the economic and social crisis related to COVID-19 may have large indirect impacts on diabetes care. For example, abrupt changes in the economy have left many individuals unemployed or dealing with massive pay cuts, which impact health insurance status and the ability to pay for care. In the USA alone, nearly 10 million people applied for unemployment in the last 2 weeks of March, and an estimated 1.5 million people became newly uninsured.41 By the end of May 2020, the unemployment rate was at 13.3% or 21 million people. Given that in the USA, health insurance is often linked to employment, losses of jobs attributable to the COVID-19 pandemic will thereby increase difficulty in obtaining care. Furthermore, changing or intensifying lockdown orders implemented by many state and local governments may magnify the effect of factors known to impact glycemic control, such as: (1) poor adherence to medications (ie, purchasing power, access to pharmacies); (2) food insecurity and sedentarism (change in nutrition and physical activity behaviors); and (3) mental health (anxiety, depression, post-traumatic stress disorder). However, the full effects of these shifts on short-term and long-term diabetes outcomes have yet to be determined. While adaptions in care are evolving, a simultaneous systematic evaluation of these adaptations, as well as indirect consequences of lockdown orders and economic factors, on the overall health of patients with diabetes is recommended.
Recovery
While social distancing measures are necessary to suppress the spread of the virus, it is unclear how long these measures will need to be enforced. By some estimates, intermittent forms of social distancing may need to be in place until the year 2022.42 After the initial threat of COVID-19 has abated, there will be a process of recovery whereby a new “normal” of diabetes care will have to be designed and assessed. While the restoration of in-person visits is expected, there is the potential for hybrid models of care delivery which may incorporate a combination of telemedicine and in-person visits. However, to formulate new methodologies of diabetes care, postpandemic assessments of the achievements and shortcomings of care during the height of the pandemic must be rigorously evaluated. Clinical diabetes care benchmarks (including glucose, HbA1C, blood pressure, and lipid levels) and cardiovascular outcomes before, during, and after the immediate crisis will need to be examined to assess the impact of rapid shifts to telemedicine on clinical parameters.
Furthermore, there is a need to collect qualitative data to better understand the patient and provider experience during the COVID-19 pandemic. This will serve to provide a more nuanced description of diabetes care and management challenges, successes, acceptability, and suggestions for improvement. This will also provide valuable information as to the impacts of and changes in important factors such as depression, diabetes distress, insurance status, isolation/loneliness, and stress that occurred due to COVID-19-related factors. As a result, we will be able delineate: (1) unforeseen consequences of the pandemic on clinical care, (2) care gaps and difficulties, and (3) potential benefits toward diabetes management as the result of moving rapidly to a telemedicine-based approach. Review of these data will help guide the creation of new models of diabetes care to best serve patients and improve diabetes-related outcomes moving forward. As care models may shift to a more telemedicine-centric approach in the USA, policy changes are needed to further integrate electronic healthcare records from different healthcare systems, pharmacies, and external laboratories to facilitate: (1) access to documentation from multiple providers and healthcare systems, (2) monitoring access/adherence to medications and supplies, and (3) access to results of relevant biomarkers to monitor for complications and provide comprehensive diabetes management and control. In addition, obtaining patients’ perspectives about their preferences during these transitions is essential.
Surveillance
Due to the rapidly infectious nature of SARS-CoV-2, healthcare systems had to abruptly improvise care delivery during an unexpected and prolonged lockdown, both in the outpatient and inpatient settings. Seemingly overnight, outpatient care for people with diabetes was changed from face-to-face consultations to “telemedicine” or virtual consultations via phone or video call.43 However, proper outpatient diabetes management requires a complex and demanding behavioral and risk reduction treatment regimen. This involves the daily monitoring of symptoms, adherence to medications, and attention to CVD risk factors, including blood pressure and lipid management. Appropriate diabetes care also includes screening for microvascular complications (ie, diabetic kidney disease, retinopathy, neuropathy) 33 44 45 as well as the assessment of significant changes in diet and physical activity level.45 Poor control of diabetes can lead to severe complications and comorbidities such as kidney failure, lower-limb amputations, blindness, and major cardiovascular events.46 ,47 Different care settings will have varying capabilities to care for patients with diabetes remotely. The impact of the sudden disruption in the cascade of care for patients with diabetes during the COVID-19 pandemic is currently unknown. It is possible that the future of diabetes care may shift toward a hybrid model combining in-person visits and telemedicine. Therefore, it is important for the research community to gather information on the impacts of virtual care on diabetes treatment and outcomes to improve shortfalls in the system. This will also help prepare for a future pandemic, where widespread emergent telehealth-based care may be needed (figure 1).
To more completely evaluate what new models of care should entail, data are also needed to assess the changes in inpatient clinical care practice for individuals with diabetes during the pandemic. These include changes in diabetes management protocols, the implementation of diabetes technology,11 12 48 the role of medications known to affect glucose metabolism and cardiac conduction (ie, hydroxychloroquine), and practice changes related to speculations about medication effects on SARS-CoV-2 (ie, renin-angiotensin-aldosterone system blockers, dipeptidyl peptidase 4 inhibitors, sodium glucose co-transporter 2 inhibitors).49–51 While data suggest that diabetes increases the risk for COVID-19 mortality,4 the long-term consequences of SARS-CoV-2 on non-fatal cases of COVID-19 among patients with diabetes are also not known. Therefore, data registries for the continuous, systematic collection, analysis, and interpretation of outcomes in patients with diabetes and COVID-19 comorbidity are necessary. Individual-level data on demographics, anthropometrics, inpatient laboratory values, and medication use prior to and during inpatient treatment should be recorded and analyzed. Once released from the inpatient setting, patients should be followed over time to assess the risk of the development of pulmonary and diabetes-related comorbidities, the risk of future infections, and overall mortality. Longitudinal data may better help us understand the impact of this pandemic among patients with diabetes, both with and without COVID-19. This information would be helpful to design prevention strategies to better care for our patients in the inpatient and outpatient setting in the future.
Preparedness and preparation for the next outbreak
As the number of new COVID-19 cases continues to grow globally, evidence indicates that healthcare systems and governments are not prepared or equipped to deal with a pandemic of this scale.52 Around the world, countries are transitioning similarly to alternative forms of diabetes care delivery, with local cultural adaptations.13 Understanding the full range of the perception of preparedness by clinicians and healthcare administrators, the processes involved during the implementation of new strategies to deliver care (ie, inpatient and ambulatory protocols, telemedicine, patient education), and assessments of the impact of those transitions on diabetes care benchmarks (ie, glycemic control, blood pressure, cholesterol targets, screening for diabetes-related complications) and patient-centered outcomes will help us design strategies to be better prepared for the next outbreak. For example, at the population level, the extent to which patients had adequate medications and supplies to monitor glucose levels and blood pressure or possessed the technology (smartphones/personal computers/internet connection) for virtual visits and access to urgent online education programs is not yet known. In addition, the effects of the pandemic on changes in the prevalence/severity of diabetes risk factors, such as: (1) sedentary behaviors, (2) food insecurity, (3) availability of professional support, (4) increased alcohol consumption, (5) deterioration in mental health, (6) failure to monitor kidney function or blood pressure, (7) delays in the care of foot ulcers or sight threatening retinopathy, (8) inappropriate continuation of discontinuation of medications, (9) level of education (diabetes emergencies, insulin dose adjustments); or (10) changes in insurance status are also not well understood.13 Information about these changes is extremely valuable as it can inform the design of strategies to improve care delivery in the future.
Understanding the perspectives of stakeholders in outpatient and inpatient care is also important to assess transitions in diabetes care delivery including: (1) preparedness to deliver appropriate care via telemedicine, (2) preparation for billing/reimbursement, (3) pharmacy delivery and payment changes, (4) frequency of virtual or in-person contacts with different staff members, (5) scheduling and deployment, (6) Health Insurance Portability and Accountability Act (HIPAA)regulations; and (7) provider satisfaction and privacy concerns. Lessons learned from response and mitigation, recovery, and surveillance studies can be implemented to improve future models of diabetes care to ensure a more prepared and seamless response in dealing with future outbreaks (figure 1).
Conclusions and recommendations
The proposed preparedness cycle of response and mitigation, recovery, surveillance, and preparedness offers a framework for adjusting and improving diabetes care during the current healthcare crisis and beyond. For example, to better care for patients with diabetes in inpatient settings, response and mitigation strategies are necessary to ensure HCW can monitor glucose levels safely, make appropriate adjustments of medications, and ensure good glycemic control to avoid additional complications. Technology to monitor glucose levels remotely is improving and research efforts are showing significant progress in the inpatient setting.11 53 54 In the outpatient setting, ideal mitigation strategies are those that ensure effective transitions to telemedicine with systems that integrate patient glucometric data, as well as strategies that ensure patients access to medications. During recovery periods (ie, post-lockdowns), strategies that ensure effective transitions back to in-person visits (if needed) should considering risk stratifying those that need to be seen in-person (eg, patients with diabetic foot infections needing surgical interventions, patients new to insulin without access to video) while the risk of infection persists. Further research is urgently needed to also understand and identify the most effective care delivery strategies centered on patients’ needs and preferences.
In addition, surveillance efforts that address and monitor disparities to identify the most vulnerable patients are needed to guide implementation of strategies that ensure appropriate access to diabetes care and COVID-19 infection prevention. A COVID-19 Health Equity Dashboard (https://COVID-19.emory.edu) was recently developed to fill the gaps in county-level data about the virus and underlying social determinants of health. Identifying patients with diabetes at the highest risk for infection, as well as those at the highest risk for complications related to fragmentations in care are needed to design strategies that ensure access to appropriate prevention and management interventions.
For better preparedness for future epidemics, policy changes that address inpatient and outpatient care of patients with diabetes and other chronic conditions are urgently needed.
Policies that ensure telemedicine capabilities are in place across healthcare centers may help accelerate the implementation of such systems during emergencies. In addition, policy changes that help patients access technology with less barriers will also be helpful. Transferring glucose data remotely to providers is becoming increasingly common. It is also time to consider changes in regulatory decisions incorporating advances in diabetes technology and not only A1c levels. The diabetes community (ie, Beyond A1c movement) has been promoting changes in regulations based on glycemic outcomes beyond A1c.55 Recently, the centers for medicare and medicaid services (CMS) announced it “will not enforce certain clinical criteria in local coverage determinations that limit access to therapeutic continuous glucose monitors for beneficiaries with diabetes.”56 To continue to address the consequences of this pandemic and potential outbreaks in the future, combined efforts between patients, researchers, public and private policy-makers and payers, and members of industry are needed to accelerate further research and implementation of technologies proven to improve care in patients with diabetes. Risk stratification tools (ie, “polysocial risk score”)57 that identify those at the highest risk may help direct prevention and intervention efforts prioritizing those at the highest risk for infection, complications, or fragmentations in care during different phases of disasters.
There is clear evidence indicating that those at the highest risk for poor outcomes during COVID-19 (eg, minorities, lower socioeconomic status) are the least likely to receive vaccinations for preventable infections.58 Once a vaccine is available (against SARS-CoV-2 or other pathogens in the future) efforts that ensure widespread vaccination of patients with diabetes including the most vulnerable will be necessary. Such planning should start immediately.
We believe that unique challenges require unique solutions to address the burdens of COVID-19 on the healthcare system, HCWs and people living with diabetes. Implementing multidimensional frameworks may help identify gaps in care, alleviate initial demands, mitigate potential harms, and improve implementation strategies and outcomes in the future. More importantly, such approach could comprehensibly guide urgent policy changes in the near future to better prepare the diabetes community for the next disaster.
References
Footnotes
Contributors UPG, LJ, and FJP conceptualized the article and designed Figure 1. UPG and FJP wrote the first draft of the manuscript. JN and MBW wrote and edited sections of the manuscript. PV, JSH, and GMD critically reviewed the approach and edited successive drafts. FJP created the concept and designed the approaches for the framework. All authors approved the final version.
Funding This project was supported in part by National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) grant number P30-DK-111024. PV is supported in part by National Institutes of Health (NIH) grant 1K23DK113241. FJP is supported in part by NIH grant 1K23GM128221-01A1.
Competing interests PV has received consulting fees from Merck and Boehringer Ingelheim. FJP has received unrestricted research support from Merck and Dexcom and consulting fees from Merck, Boehringer Ingelheim, Sanofi, Lilly, and AstraZeneca.
Patient consent for publication Not required.
Ethics approval We did not obtain ethics approval for this manuscript as it is a review article and did not require working with human subjects.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.