Article Text

Abstract
Objectives To investigate the impact of transitions out of marriage (separation, widowhood) on the self reported mental health of men and women, and examine whether perceptions of social support play an intervening role.
Methods The analysis used six waves (2001–06) of an Australian population based panel study, with an analytical sample of 3017 men and 3225 women. Mental health was measured using the MHI-5 scale scored 0–100 (α=0.97), with a higher score indicating better mental health. Perceptions of social support were measured using a 10-item scale ranging from 10 to 70 (α=0.79), with a higher score indicating higher perceived social support. A linear mixed model for longitudinal data was used, with lags for marital status, mental health and social support.
Results After adjustment for social characteristics there was a decline in mental health for men who separated (−5.79 points) or widowed (−7.63 points), compared to men who remained married. Similar declines in mental health were found for women who separated (−6.65 points) or became widowed (−9.28 points). The inclusion of perceived social support in the models suggested a small mediation effect of social support for mental health with marital loss. Interactions between perceived social support and marital transitions showed a strong moderating effect for men who became widowed. No significant interactions were found for women.
Conclusion Marital loss significantly decreased mental health. Increasing, or maintaining, high levels of social support has the potential to improve widowed men's mental health immediately after the death of their spouse.
- Mental health
- marital status
- marital loss
- life course
- gender
- gender inequalities
- longitud surveys SI
- mental health DI
- social factors IN
- sociology FQ
Statistics from Altmetric.com
- Mental health
- marital status
- marital loss
- life course
- gender
- gender inequalities
- longitud surveys SI
- mental health DI
- social factors IN
- sociology FQ
Previous longitudinal research shows that marital loss, due to either separation or widowhood, significantly increases levels of psychological distress1–3 and the likelihood of common mental disorders, such as anxiety and depression,4–10 and decreases overall mental well-being and happiness.11–14 These declines in mental health differ for men and women, where women who experience a marital loss have worse mental health than men.5 6 8 11 12 Poorer mental health and well-being after marital loss have also been found to be more acute and prolonged for the separated compared to the widowed.4 14 15 In this article we argue that the consequences of marital loss for mental health are also likely to differ depending on social circumstances around the event, in particular perceptions of social support.
To date, few studies have examined the intervening role of social support for the mental health of people who experienced a marital loss.6 9 16 This is surprising given that social relationships and high levels of social support are important for a range of mental health outcomes.16–21 People who are not married tend to have lower levels of social support, which may contribute to their lower levels of mental health relative to the married20; this suggests that social support has a mediating effect on mental health with a marital loss.22 For example, in a cross-sectional study Turner and Marino found that social support explained around 50% of the difference in depression between the married and previously married (separated, divorced and widowed).19 Social support however, might also have a moderating effect against psychological distress when persons are faced with an adverse life event such as marital loss.18 21 A moderating effect suggests that the negative consequences of marital loss through either widowhood or separation on mental health could vary depending on the level of social support. We might expect, for example, that with the loss of a marital partner having higher levels of social support means having people around to talk to, who offer comfort and practical support, which would help with the coping process and therefore lessen the negative consequences of marital loss19 21; whereas lower levels of social support may generate feelings of isolation and loneliness and exacerbate the negative consequences.
Previous cross-sectional and longitudinal studies of marital status, social support and mental health have several limitations which make it difficult to ascertain the exact role played by social support in moderating or mediating the effects of marital loss on mental health. The cross-sectional studies were unable to take into account social support and mental health prior to marital loss.15 16 19 The longitudinal studies had time-lags of several years between data collections and their results therefore represent the aggregate effects of marital loss on mental health over several years, not the immediate effects of the event.6 9
In this study we use data on 3017 men and 3225 women who were legally married in wave 1 (2001) of an annual nationally representative Australian panel study and follow them over the subsequent five waves (2002–06) to examine the short-term effects of marital loss on mental health, and the moderating and mediating role of perceptions of social support. We address three key questions:
Is marital loss associated with a decline in mental health?
Does perceived social support explain some or all of the mental health differences for those who experience marital loss?
Does the relationship between marital loss and mental health vary depending on the level of perceived social support?
In addressing each question we consider whether the associations between marital loss, mental health and perceived social support vary for men and women. We adopt this approach because previous research finds gender differences in the relationship between social support and health, where the health benefits of higher levels of social integration and social support associated with marriage are greater for men than for women.23 24 Research also suggests that gender differences in the effect of marital loss on mental health may exist, where women who separate or become widowed have worse mental health than men.5 6 8 11 12
Materials and methods
Study population
The data were compiled from the Households Income and Labour Dynamics in Australia (HILDA) survey. Wave 1 was collected in 2001 and comprised 7682 households and 13 969 individuals. Households were selected using a multi-stage sampling approach, and a 66% response rate was achieved.25 Within households, data were collected from each person aged over 15 years using face-to-face interviews and self-completed questionnaires which achieved a 92% response rate of household members.25 Waves 2–6 achieved within-household response rates of 86.8%, 90.4%, 91.6%, 94.4% and 94.9%, respectively. In the current study we focused on all participants who were legally married in their first marriage at wave 1 and follow them through to wave 6. The analytical sample comprised 3017 men with an average of 4.5 observations, and 3225 women with an average of 4.6 observations.
Measures
At each wave of the HILDA survey participants were asked about their health, marital status, perceived social support and a range of social and demographic characteristics using identically worded questions.
Marital transitions
The participant's current marital status at each wave indicated whether they were legally married, cohabiting, separated, legally divorced, widowed or never married. For this present analysis we categorised marital status as: 1=married; 2=separated; 3=divorced; 4=widowed; 5=repartnered (ie, cohabiting or remarried). We differentiate between separation and divorce, and refer to separation as the point at which marital loss occurred because Australian law requires a couple to be separated for at least 1 year before they can apply for legal divorce and many couples do not divorce for several years after separation.26 We also distinguish those who have repartnered from those who remained separated or widowed because repartnering is associated with improvements in mental health and well-being.6 11
Given that all participants were married in wave 1, we follow them over subsequent waves and observe a number of participants who transition out of marriage (table 1). The number for each marital status refers to the number of person-year observations for each marital state summed over the six waves. Each row indicates the number of people who were in that marital status over the six waves and the columns indicate the number of people who transitioned out of that marital status into another state over the six waves. For men, we observe 11 470 person-years where men were stably married, 140 men transitioned from married to separated, one from married to divorced, and 47 from married to widowed. (Note that while participants were interviewed each year, some interviews may take place up to 16 months after their previous wave interview, which explains why we observe one transition from married to divorced despite the legal requirement in Australia of being separated for 1 year.) For women, there were 12 339 person-years for those who were stably married, 150 women transitioned from married to separated, one transitioned from married to divorced, and 103 from married to widowed. These transitions could have occurred any time over the six waves and the numbers will not necessarily add up due to missing data.
Number of transitions out of marriage; Households Income and Labour Dynamics in Australia (HILDA), waves 1–6 for men and women
Perceived social support
Our measure of social support does not describe the relational content of a participant's network; rather it captures their perceptions of support available from other people.18 21 27 Perceptions of social support have been found to be as important for health outcomes as relational content.16 21 We compiled a scale by summing responses to 10 items: ‘people don't come to visit me as often as I would like’; ‘I often need help from other people but can't get it’; ‘I seem to have a lot of friends’; ‘I don't have anyone that I can confide in’; ‘I have no one to lean on in times of trouble’; ‘there is someone who can always cheer me up when I am down’; ‘I often feel very lonely’; ‘I enjoy the time I spend with the people who are important to me’; ‘when something's on my mind, just talking with the people I know can make me feel better’; and ‘when I need someone to help me out, I can usually find someone’. The items were scaled using Likert-type response options that ranged from 1 ‘strongly disagree’ to 7 ‘strongly agree’. Negatively worded items were reverse-scored. The scale had a Cronbach's α of 0.79, indicating an acceptable level of internal reliability. Our approach to compiling the social support scale is similar to that used elsewhere.28
Covariates
We adjust for various factors found in previous studies to be associated with basic demographic variation in mental health.2 5 14 Marriage duration in years and months at wave 1 was included as a continuous measure. The participant's age was included as a continuous measure. Education had four groups: 1=year 12 or less (high school or less); 2=trade qualifications; 3=diploma; 4=bachelor degree or higher. Income was annual household income, as a continuous measure. Employment status was: 1=full time; 2=part time; 3=unemployed; 4=not in the labour force (NILF).
Mental health
Our measure is the 5-item mental health subscale (MHI-5) derived from the Short-Form 36 (SF-36). The SF-36 is a self-completion measure of health status comprising 36 items that measure eight dimensions of functional health and well-being.29 The MHI-5 is a well-validated measure for common mental disorders such as anxiety and depression,30 and has been found to be a good predictor of clinical mental health problems, including psychiatric illness,31–33 and other health outcomes, such as stroke.34 Scale scores ranged from 0 to 100, with a lower score indicating higher levels of nervousness and depression and higher scores indicating that a person feels peaceful, happy and calm.29 The MHI-5 had a Cronbach's α of 0.97, indicating a high level of internal reliability. Table 2 presents the descriptive statistics for the covariates, mental health and social support measures.
Descriptive statistics for model covariates pooled panel, by gender
Analytical strategy
Change in mental health with marital loss was examined using a linear mixed model that takes into consideration the clustering of observations within persons and has the capacity to handle unbalanced panel designs (inconsistent numbers of observations per person).1 35 The models were fitted using xtreg in STATA V.10.1.36
To exploit the longitudinal nature of the data and to best capture the effect of marital loss on mental health, several lagged effects were included in our models. We included a 1-year lag for marital status (t−1) with six categories: 0=stably married (reference group); 1=married in the previous wave, but experienced marital loss; 2=separated; 3=divorced; 4=widowed, and 5=repartnered. To interpret our model results the main effect and lagged effect of marital status need to be interpreted together. The coefficient for the original marital status variable indicates the effect of current marital status on mental health (t0). The coefficient for the lagged marital status measure indicates the effect of marital status in the previous wave on mental health (t−1). Thus, the combination of the main effect and the lagged effect captures whether or not mental health significantly declines for those who go from being married in the previous wave (t−1) to being separated or widowed in the current wave (t0). We also include measures for lagged mental health and lagged social support. These lagged measures helped control for unobserved heterogeneity between individuals and reduced the potential for reverse causality. Unobserved factors, for example, could be associated with low levels of perceived social support, poorer mental health and a marital loss. Our models therefore captured the effects of separation or widowhood on mental health, taking into account prior mental health and changes in social support as a result of marital loss.
Analysis proceeded in three stages. First, we estimated a baseline model of the associations between marital status and marital loss and mental health, including covariates (model A). In our second model, we included perceptions of social support to see if this accounted for any mental health differences for those who experienced marital loss (model B). Prior to estimating our second model we established that marital loss was also associated with perceptions of social support. In our final model (model C) we test for linear moderation effects and include interactions between perceived social support and marital status and lagged marital status.22 This enabled us to investigate the extent to which higher levels of social support buffer, or lower levels exacerbate, any adverse mental health affects due to transitions out of marriage. Although the final models are presented separately for men and women, in preliminary analysis we estimated models using the pooled sample of men and women with gender interactions to establish whether any gender differences were statistically significant.
Results
Table 3 presents the results for men. Men who transitioned from married to separated between waves had mental health scores 5.79 points (−3.79 + −2.00=−5.79), or 18% lower (5.79/31.95×100) than stably married men (table 2, model A). Compared to stably married men, those who transitioned from married to widowed had mental health scores 7.63 points (23.9%) lower.
Linear mixed models of the associations between marital loss, social support and mental health*, for men (n=3017)
There was a positive association between perceptions of social support and mental health for men (table 2, model B). Social support in the previous wave was not strongly associated with men's mental health in the present wave. For men, social support explained some, although not all of the difference in mental health between those who separated or widowed and the stably married. The lagged coefficient for previously married was no longer statistically significant and the coefficient for separated men was only marginally significant. In this model men who transitioned from married to separated had mental health scores 4.43 points (−3.09 + −1.34=−4.43), or 11.8% lower than stably married men; the gap was 8% lower than in the first model not adjusting for social support. Findings are similar for widowed men: while the effect of being widowed was significant, the difference between their mental health and that of stably married men is 7.06 points lower (18.8%), compared to 23.9% in model A.
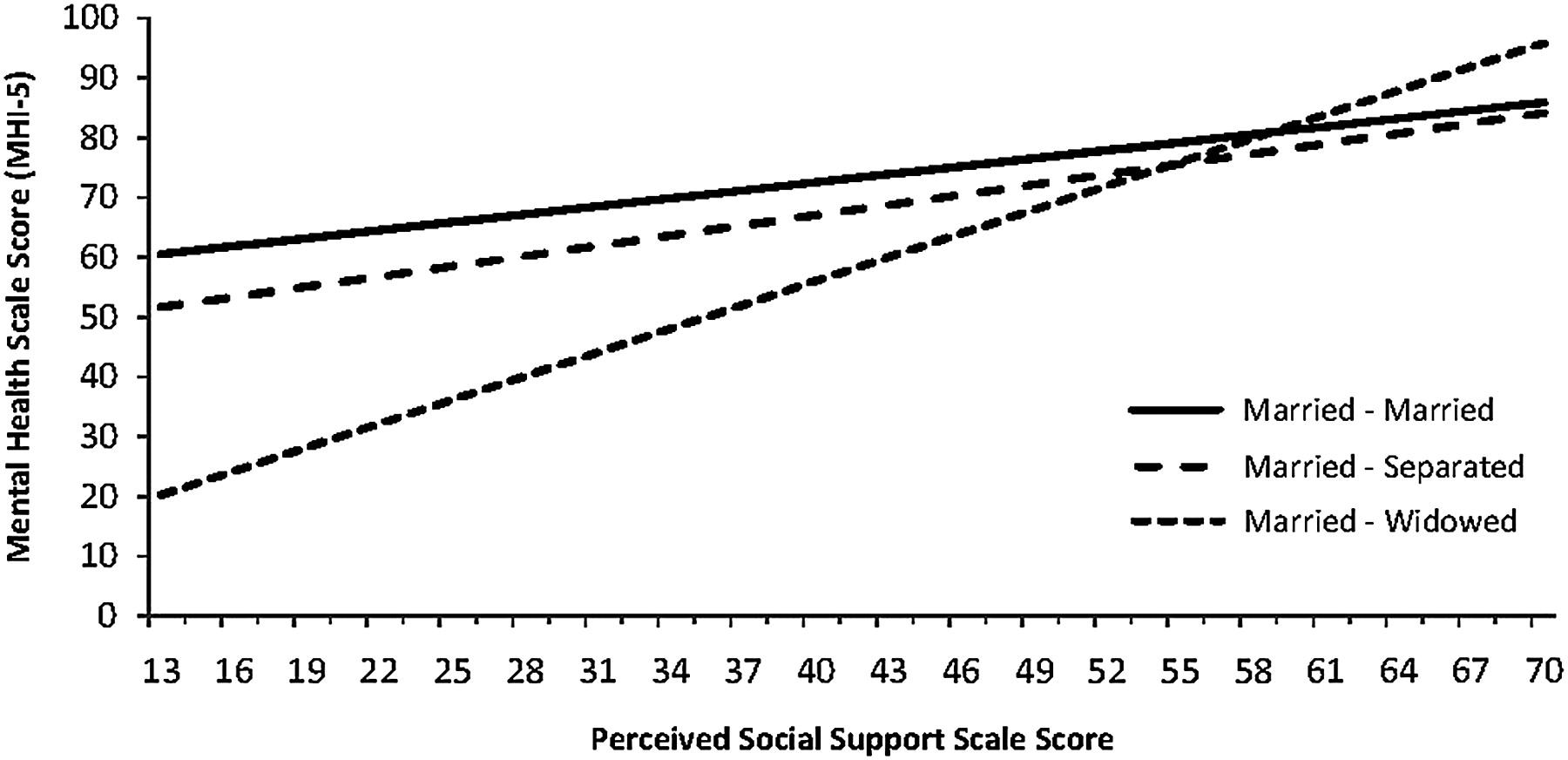
The final column in table 3 (model C) adds interactions between perceived social support and marital status and lagged marital status to the model. For men, high levels of social support were associated with better mental health (figure 1); however, the only significant interaction term was for those who transitioned from married to widowed. Consistent with the expected moderating effect on mental health, higher social support lessens the negative consequences of becoming widowed and lower social support exacerbates the consequences. A transition to divorce, which, as shown in table 1, typically occurs after separation, is not associated with mental health. Additionally, repartnering is not significantly associated with mental health for men.
{kind=link}
Marital loss, perceived social support and mental health for men (table 3, model C). Controls are held constant at mean or modal responses. Plot scores are for men with year 12 or less education, no children <18, Australian born, employed full time, aged 50.04, marriage duration of 21 years, and a mean household income of $62 974 pa.
Table 4 presents the results for women. Model A indicates that transitions out of marriage had a similar impact on women's mental health as men's. Compared to stably married women, those who transitioned from married to separated had mental health scores 6.65 points (21.4%) lower, and widowed women had mental health scores 9.28 points (29.9%) lower. The magnitude of the decline in mental health was larger for women, but none of the gender differences were statistically significant.
Linear mixed models of the associations between marital loss, social support and mental health*, for women (n=3225)
The results of model B for women indicate a significant negative association for lagged social support, suggesting that higher levels of social support in the previous wave reduced mental health in the current wave, although the magnitude of the association was small. Compared to the men, there was less change in the significance and magnitude of the associations for transitions into separation and widowhood when controlling for the effect of perceptions of social support on mental health for women. Women who separated had mental health scores 6.71 points (18.7%) lower than stably married women, compared to 21.4% in model A. Women who were widowed had mental health scores 9.07 points (25.3%) lower, down from 29.9% in model A. None of the gender differences were significant. In the final model (model C) for women the results show that higher levels of perceived social support were associated with better mental health. Unlike men, however, the association between social support and mental health was similar irrespective of the type of transition. These differences in perceived social support for men and women who became widowed were statistically significant. The transition from separated to divorced is not significantly associated with mental health for women. Repartnering is negatively associated with women's mental health.
Discussion
Six waves of an Australian panel study (2001–06) were used to investigate the relationships between marital loss, mental health and perceptions of social support. The first stage of our analysis examined whether marital loss was associated with a decline in mental health. The results provided good evidence that a transition to separation or widowhood significantly decreased levels of mental health relative to staying married. This is consistent with previous longitudinal research.14 Our study also indicated that separation was the crisis point for mental health, not divorce: studies that collapse the separated and divorced may therefore be overlooking some important differences between the groups. This finding, however, may also be specific to the Australian situation due to divorce laws that require couples to be formally separated for at least 1 year before they can apply for legal divorce. In addition, repartnering was negatively associated with mental health for women, which contrasts with previous studies that concluded that repartnering improved mental health.13 Our finding however, should be viewed circumspectly due to the small number of repartnering transitions.
Our modelling approach and the inclusion of time varying covariates meant the results were net of mental health prior to the event, and adjusted for any changes in economic circumstances surrounding the event. The magnitude of these associations was larger for women than for men, but we found no significant gender differences. This was broadly consistent with previous research investigating gender differences in mental health with marital loss where the findings have been mixed. Some studies find no significant gender differences,1–4 9 14 however when gender differences are found women who separated or became widowed typically had worse mental health than men.5 6 8 11 12
Stage two of our study investigated whether perceived social support explained some or all of the mental health differences for those who experienced a marital loss. Social support did not account for all of the differences in mental health between those who remain stably married and those who separated or divorced. The results of our second model indicated that social support attenuated the magnitude of the effects of marital loss on mental health; however, with the exception of separated men, the association between marital loss and mental health remained significant. We therefore find little evidence of a strong mediation effect of social support on mental health with a marital loss. This is consistent with earlier longitudinal studies which found little or no change in mental health, taking into account differences in social support.6
The final stage of our analysis examined whether the relationship between marital loss and mental health varied depending on the level of perceived social support. We found that high levels of social support weakened the negative mental health consequences of a transition to widowhood for men, and lower levels of social support magnified the negative consequences of the transition. Social support may be particularly important for widowed men, because as our data showed it is a relatively uncommon transition for them to experience.
Study limitations
Even in a large national population sample we only observe a relatively small number of transitions from married to separated (n=290) or widowed (n=150). In addition, those who transitioned out of marriage have higher rates of attrition in the HILDA survey than those who are stably married.37 These two factors increased the SE and therefore increased the risk of making a type II error; our results are therefore somewhat conservative.
While our models controlled for levels of social support prior to the transition as well as after, the direction of the association is still not clear. We find that participants' perceptions of social support change with some transitions. Additional analysis (results not shown) indicated that the level of social support was different for the stably married compared to those who transitioned to separation or widowhood: married men had significantly higher levels of social support than men who separated, and married women had significantly higher levels of social support than widowed women. We only examined the relationship between mental health and social support in the year of the marital loss, and do not consider the medium and longer term effects of being separated or widowed over multiple waves or the role of social support on the longer term mental health consequences of a marital loss. Previous studies that have examined the longer term mental health consequences find that the negative effects of marital loss on mental health tend to reduce with time.14 It is possible that changes in social support may explain some of this improvement in mental health.
Finally, the measure of social support used in this study was general and did not differentiate between sources of support, such as from family, friends or neighbours. Different sources may vary in their effect on mental health with marital loss, and knowing the source and type of social support could provide insights that further our understanding of the mechanisms. In the event of separation, for example, support from family may increase, but support from friends (who are more likely to be divided by the breakup) may decrease. An important direction for future research is to use more specific measures of social support to assess the role of different sources in buffering or exacerbating the negative mental health effects of a marital loss.
Conclusion
Marital loss decreased short term mental well-being net of mental health prior to the event and any changes in social and economic circumstances due to the event. There was little evidence that perceptions of social support play a mediating role in the association between marital loss and mental health. In contrast, perceptions of social support play a significant moderating role for widowed men's mental health, which suggested that increasing or maintaining high levels of social support can potentially improve men's short term mental health and well-being when they become widowed. Investigating changes in social support, different sources of social support and the medium-term effects of social support on mental health after marital loss, are important directions for future research.
What is already known on this subject
The negative association between marital loss and mental health is well established.
Less research has investigated the social contexts and mechanisms that might explain this association.
What this study adds
A transition from married to separated or widowed negatively impacts mental health.
Separation, not divorce is the crisis point for mental health.
Social support does not account for all of the differences in mental health between the stably married and the separated and widowed.
Interactions between social support and marital transitions indicated that high levels of social support lessened the negative mental health consequences for men who became widowed.
Acknowledgments
We thank Michele Haynes for statistical advice, and Ruth Weston, participants at the HILDA conference 2009 and three anonymous reviewers for valuable feedback on earlier drafts.
References
Footnotes
Funding This work was supported by funding to BH from the Australian Research Council (grant number DP0770586) and University of Queensland New Staff Research Start-up grant. GT is supported by an Australian National Health and Medical Research Council (NHMRC) Senior Research Fellowship (ID 390109). This research uses unit record data from the Households Income and Labour Dynamics in Australia (HILDA) survey funded by the Commonwealth Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) and conducted by the Melbourne Institute for Social and Economic Research (MISER) at the University of Melbourne. The research findings are the product of the researcher and should not be attributed to FaHCSIA or MISER.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.