Article Text

Abstract
Introduction Medication discrepancies are associated with adverse drug events. Electronic health records (EHRs) may reduce discrepancies, especially if integrated with pharmacy dispensing. We determined the prevalence of discrepancies within a national healthcare system with EHR–pharmacy linkage to characterise the medications involved and to identify factors associated with discrepancies.
Methods We conducted a retrospective cohort study of ambulatory care patients at Veterans Affairs Boston Healthcare System, April 2010–July 2011. The primary outcome was the presence of any medication discrepancy or specific types of discrepancies: commission—present in the record but not taken by patient; omission—not present in the record; duplication—present more than once; or alteration in dose or frequency—present but taken differently than documented.
Results Sixty-two patients (60%) had at least one medication discrepancy. Prevalence of commissions, omissions, duplications and alterations were 36%, 27%, 11% and 19%, respectively. The involved medications differed by type of discrepancy, but non-opioid analgesics and herbal therapies were common among commissions and omissions. In adjusted analyses, an increasing number of medications was associated with more commissions (OR 1.2; 95% CI 1.1 to 1.3) and duplications (OR 1.2; 95% CI 1.1 to 1.4) and fewer omissions (OR 0.9; 95% CI 0.8 to 1.0).
Discussion In a system with a well established EHR linked to pharmacy dispensing, medication discrepancies occurred in 60% of ambulatory clinic patients. Patients with a greater number of medications were more likely to have errors of commission and duplication, but less likely to have errors of omission. Our findings highlight that relying on EHRs alone will not ensure an accurate medication list and stress the need to review medication taking thoroughly with patients to capitalise on the full potential of EHRs.
- Medication reconciliation
- Information technology
- Adverse events, epidemiology and detection
- Ambulatory care
Statistics from Altmetric.com
- Medication reconciliation
- Information technology
- Adverse events, epidemiology and detection
- Ambulatory care
Introduction
With care that is fractured among various sites and healthcare providers, medical information is subject to incomplete transmission between patients, providers and discrete healthcare systems.1 This fragmentation can result in medication discrepancies, which are unintentional differences found in the patient's medical record compared with the patient's medication information.2 Discrepancies may be commissions, omissions, duplications or alterations. They are associated with adverse drug events (ADEs), which are broadly defined as ‘injury resulting from the use of a drug’.3 Research on ADEs and medication discrepancies has predominantly focused on the inpatient setting or on care transitions. However, studies of ambulatory settings have estimated that 25% of patients have experienced ADEs,4 while as many as 60% of patient records contain medication discrepancies.5 ,6
Recognising the large role of medications in patient care and safety, the Joint Commission introduced medication reconciliation as a National Patient Safety Goal in 2005, with updated recommendations in 2012, to ‘maintain and communicate accurate patient medication information’.7 ,8 This consists of an accurate and complete medication list including all medications that a patient is currently taking, including over the counter medications, nutritional supplements, herbal products and anything classified as a drug by the Food and Drug Administration. In addition to the medication names, there should be documentation of dosage, frequency and formulation. Many healthcare organisations, including the Veterans Health Affairs, have initiated processes to encourage and document medication reconciliation.2 ,9
Health information technologies (HITs) are frequently cited as a promising solution to healthcare inefficiencies and as a modality to improve quality and safety, but thus far, these expectations have been minimally realised.10 ,11 One method by which HITs could improve care is through robust clinical decision support systems. These systems function to warn clinicians of potentially dangerous medication prescribing due to drug–disease or drug–drug interactions, and they can also provide reminders for healthcare that might be beneficial to the patient. Such systems will not perform to their maximum potential if the medication information in the record differs from what the patient is actually taking. With the Health Information Technology for Economic and Clinical Health Act's allocation of more than $48 billion to the adoption and meaningful use of HITs,12 it is critical to implement electronic health records (EHRs) that are effective and efficient in improving patient safety and appropriate medication prescribing. Before this can be accomplished, it is necessary to understand the magnitude and characteristics of current inadequacies in medication reconciliation in ambulatory care within a healthcare system that has a mature EHR with direct linkage to pharmacy dispensing, a feature that provides an added level of integration. Therefore, our objectives were to quantify medication discrepancies, categorise discrepancy types, determine the medications involved in each type of discrepancy, and identify patient-level and system-level factors associated with the presence of medication discrepancies within the EHR of the Veterans Affairs (VA).
Methods
Study design and setting
We conducted a retrospective cohort study of a convenience sample of patients from ambulatory care clinics, including Primary Care, Rheumatology and Heart Failure, at VA Boston Healthcare System from April 2010 until July 2011. The VA has an integrated EHR, the Computerised Patient Record System (CPRS), introduced in 1997, which includes computerised provider order entry, pharmacy records, laboratory and radiology results, and visit documentation. Prescriptions that are entered, changed or discontinued within CPRS are directly linked to pharmacy dispensing so that medications prescribed by a VA provider cannot be filled if the order is no longer active within the EHR. Decision support within CPRS identifies drug–drug interactions and duplications within a VA drug class. Any prescribing provider or pharmacist can enter, modify or discontinue prescriptions for any patient, and prescriptions typically expire automatically after 1 year. Medications obtained from non-VA sources (eg, over-the-counter medications or prescriptions filled at one or more community pharmacies) need to be manually entered by clinicians and do not automatically populate or update. Medications prescribed at remote VA locations (ie, a VA other than the local site) cannot be altered or discontinued by local providers; to enact these changes a provider or pharmacist at the remote location needs to be contacted.
Data source
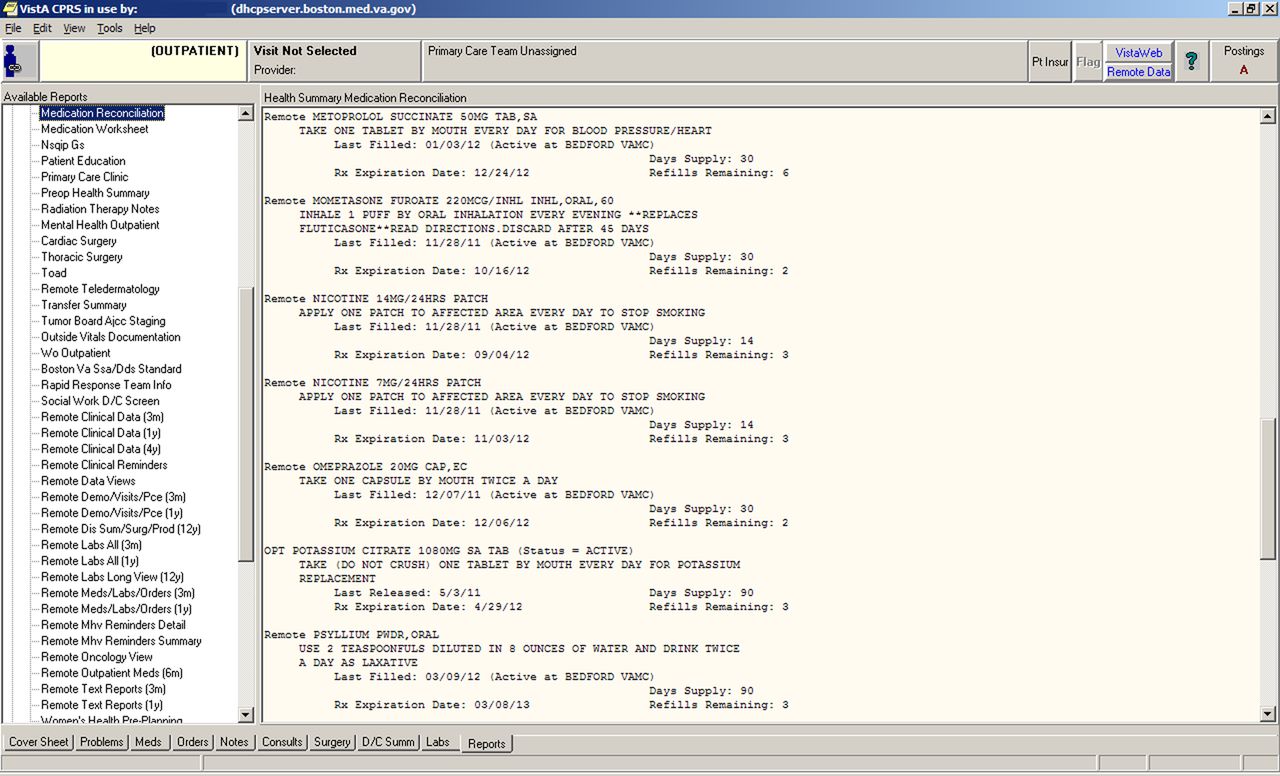
The data were collected by 13 4th-year medical students as part of their Ambulatory Medicine Quality Improvement rotation. At the beginning of each 4-week rotation, students were individually instructed on project goals and processes. Then, each student performed medication reconciliation. As recommended by the VA Boston Healthcare System Directive,2 the CPRS Reports Tab: Health Summary Medication Reconciliation List (hereafter referred to as the ‘List’) was the source of all medications, each of which is labelled with the prescribing location as local-VA, non-VA, or Remote (ie, prescribed at a VA other than Boston) (figure 1). This list includes all medications except those documented within unstructured free text of progress notes. Students interviewed patients at the beginning of the clinical encounter to ascertain the medications they were currently using. They then documented all discrepancies between what the patient reported and what was documented in the EHR on a printed version of the List, and all omitted medications were elicited verbally and then handwritten as additions. Because the data collection was part of usual care and intended as a quality improvement educational project, informed consent was not obtained at the time of medication reconciliation.

{kind=link}
Screenshot of computer-generated medication reconciliation list.
One of us (AL) entered all data into an Excel database, and we analysed only the first chronological encounter for each Veteran. We included all entries on the List, including topical and inhaled medications, herbals and over-the-counter medications, consistent with recommendations from the Joint Commission.8 Medical supplies were not counted. Entries were spot checked at random and any uncertainties were resolved by both members of the research team.
Study variables
Consistent with Veterans Health Administration Directive descriptions, each medication discrepancy was classified as one of four types: commission—a medication listed as active in the EHR but the patient reported they were not currently using it; omission—a medication that the patient reported using but was not listed as active in the EHR; duplication—more than one active listing for the same medication or medication class; and alteration in dose or frequency—when the patient reported taking a medication at a different dose or frequency than recorded in the EHR.9 Discrepancy types are not mutually exclusive (eg, a medication can be both a commission and a duplication) and more than one discrepancy can occur per EHR-generated List.
The medication for each discrepancy was also classified into medication class using VA drug class codes. Other data extracted from the List included patient sex; age at visit; number of actively prescribed medications; whether each medication was prescribed locally, remotely or obtained in a non-VA setting; and whether allergies were documented at other VA sites (as a proxy variable to indicate the Veteran had received remote care at some point prior to the ambulatory clinic visit).
The five pre-planned outcome variables were each of the four types of discrepancies and a composite outcome of omissions, commissions, duplications and alterations (ie, ‘any’ discrepancy).
Statistical analyses
We first determined the prevalence of each outcome for the study population. Frequency counts identified the medication classes involved in each type of discrepancy, and because a patient could have multiple discrepancies, the unit of analysis was the medication for this objective. We used single-predictor logistic regression to associate the presence of any and specific types of discrepancies within a participant's record with each of the patient-level and system-level characteristics. Finally, we adjusted for all measured covariates with separate multivariable logistic models for each of the five outcomes. To maintain uniformity with the five separate models, we chose to keep all covariates in each model.
All analyses were performed with SAS V.9.2 or Microsoft Excel. Statistical significance was set at α<0.05. This study protocol was approved by the Institutional Review Board of the VA Boston Healthcare System.
Results
Of the 106 medication reconciliations performed, we eliminated one because it was a patient's second encounter and one because the number of duplication-type discrepancies present in the patient's record (nine) was a statistical outlier. The remaining medication reconciliations yielded our study cohort of 104 participants, each with one encounter. This Veteran cohort included predominantly men (95%), and 59 (57%) were age 65 years or older (table 1). Lists contained a mean of nine medications (SD 5.7). Sixteen patients (15%) had evidence of care in other VA systems, and 50 (48%) had documentation of non-locally dispensed medications.
Baseline characteristics of veteran cohort (n=104)
Prevalence of discrepancies within the electronic health record
Sixty-two patients (60%) had at least one medication discrepancy, with a total of 232 distinct discrepancies (mean of 3.7 among those with at least one discrepancy). Prevalence of commissions, omissions, duplications and alterations in dose or frequency among all 104 participants were 37 (36%), 28 (27%), 11 (11%) and 20 (19%), respectively. The frequencies with which selected medication classes and medications comprise specific types of discrepancies can be seen in Table 2. (The complete list of discrepancies can be found in the online appendix.)
Selected medication classes and medications comprising specific types of discrepancies*
Factors associated with discrepancies
In unadjusted analyses, each additional medication was associated with a higher likelihood of commissions (OR 1.1; 95% CI 1.1 to 1.2) and duplications (OR 1.2; 95% CI 1.1 to 1.4) and a lower likelihood of omissions (OR 0.9; 95% CI 0.8 to 1.0). Non-locally dispensed medications were associated with increased odds of duplications (OR 5.7; 95% CI 1.2 to 27.9). In adjusted analyses, an increasing number of medications remained associated with a greater number of commissions (OR 1.2; 95% CI 1.1 to 1.3) and duplications (OR 1.2; 95% CI 1.1 to 1.4) and fewer omissions (OR 0.9; 95% CI 0.8 to 1.0) (table 3). Patients age 65 and older were more likely to have omissions (OR 3.6; 95% CI 1.2 to 10.4).
Factors associated with medication discrepancies in the electronic health record†
Discussion
We found that 60% of patients visiting ambulatory care clinics in a healthcare system with a well established and broadly integrated EHR had one or more medication discrepancies. Discrepancies have been associated with ADEs, which lead to increases in healthcare utilisation, costs and morbidity.3 Further, the presence of discrepancies in the medical record reduces the ability of clinical decision support systems to operate at their maximum potential, limiting many HIT efforts to improve patient safety and health outcomes.
Specific types of medication discrepancies may have different aetiologies and effects on healthcare quality. We found that 36% of patients had an error of commission, when a medication appeared active in the record yet the patient reported not taking it. This discrepancy could lead to unnecessary alerts for drug–drug interactions, adding to known concerns with alert fatigue.13 It may also contribute to polypharmacy if a clinician, under the impression that a patient is not reaching treatment targets with the current documented regimen, initiates another medication or to overmedication upon admission to the hospital if the only source of medications is the EHR and the patient is unable to report which drugs they are actually taking. Conversely, and perhaps more importantly, 27% of the patients reported taking one or more medications that did not appear on the active medication list. These omissions may have resulted from a patient's neglect to report these medications or from a failure of the provider to enter them manually into the appropriate fields in the EHR. Such omissions would not be included in any potential computerised drug–drug interaction alerts, and they would not be appreciated by a clinician depending on the EHR's medication list for an accurate summary of the patient's current medications. Among the commonly omitted medications in this study were aspirin, herbals and supplements, all agents known to have physiological effects and to interact with other prescribed medications.14 The need to manually enter these agents, along with possible under-appreciation of their physiological effects, may explain these findings. Duplications, especially of medications within the same class, could lead to unintentional overdose with adverse consequences.
In studies spanning the past decade, the reported prevalence of discrepancies within EHRs ranges from 26% to 60%, consistent with our findings.5 ,6 Although 10–15 years may be needed before improvements in quality are seen after EHR deployment,15 our study reports the prevalence of discrepancies 14 years after the introduction of the VA's EHR. With regard to type of discrepancy, some studies have found that the most common error found on medication lists is omission of a regularly used medication,5 ,16 while others have reported that the most common discrepancy is the presence of a medication that the patient was no longer using (eg, commission).17 We found that commissions were most common, followed by omissions, alterations and then duplications. These variations may be due to patient medication taking behaviours, characteristics of the EHR or other unidentified causes.
Studies comparing the accuracy of EHRs to paper records have demonstrated similar results. Boockvar and colleagues evaluated the presence of discrepancies during transitions in care within the VA compared with those seen in a non-VA setting without an EHR and found no difference in prevalence of discrepancies between a system with an EHR compared with one without.18 Another study of patients calling a nurse triage line within a large healthcare system found an average of 2.7 medication discrepancies per patient.17
While researchers and policymakers have focused considerable attention on medication-related safety in inpatient settings and during transitions in care, fewer studies have emphasised ambulatory care. The majority of chronic medication prescribing occurs in the outpatient setting, making it an ideal location to address and improve deficiencies in safe medication prescribing. In this study, we were able to evaluate an EHR that is directly linked to pharmacy dispensing. This integration ensures that the linked pharmacy cannot refill a medication that the clinician has discontinued, because the electronic prescribing and discontinuation information is seamlessly connected to the pharmacy's dispensing system. In contrast, in a setting without such linkage, as in a community pharmacy, a patient may continue to refill a prescription long after the clinician has ‘discontinued’ the medication in the EHR; in such settings, there are few, if any, mechanisms in place for providers to discontinue a medication once the prescription has been given to the patient. Despite the linkage in our system, a feature not present in most healthcare systems and EHRs, we did not see a reduction in the presence of medication discrepancies compared with reported prevalence in other settings.
Our findings suggest that efforts are needed to improve medication reconciliation in general. Approaches could include HIT-related interventions, such as use of clinical decision support systems that flag medications without an appropriate indication on the problem list, or systems that engage the patient with secure electronic messaging to send information from home about currently used medications.19 Establishing linkage to non-VA pharmacies may lead to reductions in omissions, and flagging providers when prescriptions are not filled in a timely manner may identify commissions. Interventions not requiring information technologies include use of other healthcare team members to perform what often is a time-intensive task, fitting well with efforts to expand the patient-centered medical home.
These findings should be interpreted in light of several limitations. First, this was a small population within a single site of the larger healthcare system and may not represent all VA or non-VA ambulatory care practices. The presence of the clinics within a large urban community may mean more patients receive care from non-VA providers, adding another level of complexity to their care. Using documented allergies as a proxy may have also underestimated the complexity of care within the VA. Our findings underscore the need to conduct broader analyses to yield more generalisable results. As is the case with any medication reconciliation, we relied on the patient to accurately report adherence to prescriptions and to recall omitted medications. Likewise, we are also unable to determine whether the discrepancies are clinically appropriate (ie, a commission medication remains on the list because the provider believes it is in the patient's interest to continue taking it). Also, while we did not perform audits of students, it is likely that a less thorough medication reconciliation would have failed to identify discrepancies and our results would then be an underestimate of the true prevalence. We had no information on patient comorbidities, but others have found that length or composition of medication lists can adequately represent comorbidity.20 Because this was a retrospective observational study, we are unable to compare our findings directly to a system without EHR linkage to pharmacy dispensing, yet others have shown no difference between electronic and paper records.17 ,18 Finally, we have no information on actual ADEs resulting from discrepancies, but others have demonstrated their association.21
In our study, an increasing number of medications on the List were associated with errors of commission, omission and duplications. While it is possible that the increased documentation of medications allows for more commissions and duplications, and conversely makes it less likely to have an omission, the known association between discrepancies and ADEs highlights the importance of maintaining an accurate record. Further, previous literature demonstrates that a greater number of medications is associated with risk of ADEs,4 ,22 emphasising the value in reducing the presence of medications that may be outdated, not indicated, or of limited benefit relative to risk. Excess medications on the List may reflect inadequacies in documentation (ie, failing to remove a medication from the list) or inertia in prescribing (ie, renewing a medication without giving formal thought to its continued benefit). Additional research is necessary to determine how medication regimens can best be evaluated for potential discontinuations, how this decision can be communicated to the patient, and how interventions can facilitate appropriate proactive medication discontinuation.
In conclusion, as mandates directing implementation and demonstration of successful HIT continue, it is essential to recognise that simply using an electronic record, even one with direct linkage to pharmacy dispensing records, does not ensure accurate and complete documentation. Without correct data elements, benefits of clinical decision support systems similarly will be hampered, leading to missed opportunities to improve patient safety and efficiencies in healthcare. Providers must be cognisant of these issues and continue to perform detailed medication review and reconciliation with their patients.
Acknowledgments
We thank Anand Kartha and Pamela Bellino, VA Boston Healthcare System for the opportunity to engage medical students, and all medical students who participated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors AL had full access to all of the data in the study and takes responsibility for the integrity and accuracy of the data analysis. AL: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; administrative, technical or material support; study supervision. SRS: analysis and interpretation of data; critical revision of the manuscript for important intellectual content; administrative, technical, or material support.
-
Funding The study was conducted using resources of the VA Boston Healthcare System. The work was initiated while Dr Linsky was a fellow supported by Boston Medical Center and the Center for Organisation, Leadership, and Management Research at VA Boston Healthcare System.
-
Competing interests None.
-
Ethics approval VA Boston IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.