Article Text

Abstract
Background: Most medication error studies come from inpatient settings. There is limited information about medication errors in primary care settings.
Objective: To describe medication errors reported by family physicians and their office staff and to estimate their preventability using currently available electronic prescribing and monitoring tools.
Design, setting, participants and study instrument: In two error reporting studies conducted by the American Academy of Family Physicians (AAFP) National Research Network (NRN), 1265 medical errors were voluntarily reported by >440 primary care clinicians and staff from 52 physician offices. The 194 error reports related to medications were abstracted and analysed using a medication error coding tool—Medication Error Types, Reasons, and Informatics Preventability (METRIP).
Main outcome measures: Type, severity and preventability of medication errors and associated adverse drug events (ADEs).
Results: 126 (70%) of the medication errors were prescribing errors, 17 (10%) were medication administration errors, 17 (10%) documentation errors, 13 (7%) dispensing errors and 5 (3%) were monitoring errors. ADEs resulted from 16% of reported medication errors. The severity of harm from reported errors were: prevented and did not reach patients, (72, 41%), reached patients but did not require monitoring (63, 35%), reached patients and required monitoring (15, 8%), reached patients and required intervention (23, 13%) and reached patients and resulted in hospitalisation (5, 3%). No deaths were reported. Of the errors that were prevented from reaching patients, 29 (40%) were prevented by pharmacists, 14 (19%) by physicians, 12 (17%) by patients and 5 (7%) by nurses. 102 (57%) of the reported errors might have been prevented with enhanced electronic prescribing and monitoring tools.
Conclusions: Most medication errors reported from US family physician offices were related to prescribing errors and more than half of the errors reached patients. The errors were prevented by pharmacists, patients and physicians. More than half of the errors could be prevented by electronic tools.
Statistics from Altmetric.com
More than 7000 inpatient deaths due to medication errors and another 1.5 million preventable adverse drug events are estimated to occur annually in the USA.12 Medication errors and adverse drug events can cause emotional distress, instil distrust and diminished satisfaction with the healthcare system, and lead to lost productivity and increased healthcare costs.12
In its effort to improve medication safety, the Institute of Medicine (IOM) expert committee made several recommendations in 1999 and 2006 which included implementing error reporting programmes, using informatics technology, and encouraging collaborative practices between pharmacists and physicians.12 For years, hospitals have used medication event reporting programmes to better understand medication safety issues in the inpatient setting.3–9 We know a great deal, therefore, about the types of medication error that occur in inpatient settings through these efforts and through the national medication reporting system, the United States Pharmacopeia Medication Event Reporting System.
Little is known, however, about the types and consequences of medication error that occur in the outpatient setting, where at least 3.5 billion medication prescriptions are dispensed each year.10 Error and adverse event reporting programmes in the outpatient setting are one way to help us understand medication safety issues and design effective strategies for error reduction in this practice setting. We have conducted error reporting studies in family medicine offices and found that a considerable proportion of the reported errors were medication errors.1112 Furthermore, we developed a medication error classification tool empirically based on both an intervention framework and on the empirical data we have gathered. The purpose of this report is to describe the type, severity and potential preventability of medication errors and their associated adverse drug events reported from family physicians’ offices in the USA.
METHODS
Data source
Medication errors and adverse drug events analysed in this report came from two error reporting studies conducted by the American Academy of Family Physicians National Research Network (AAFP NRN) and the Robert Graham Center.1314 In the first study 42 family physicians from 42 practices reported errors they observed or committed over a 20-week period in 2000.13 In the second study, 401 clinicians and staff from 10 diverse family medicine offices reported errors over a 10-week period in 2003.14 The 52 practices were located in rural, urban and suburban areas, and included private practices, residency training clinics, and community health centres. Participants were asked to report things that happened in the practice that should not have happened and that they did not want to happen again. They were asked to also report events or processes that did not happen but should have happened. Errors were reported either via a web-based system or on paper.1314 Fields of the reporting instrument included a narrative description of the event, consequences, harms, potential prevention strategies and information about the affected patient. Participants submitted a total of 1265 event reports.
Review process
The reported medication errors from the two datasets were identified by the original research teams using methods previously published.1314 We classified the medication error reports using the Medication Error Types, Reasons, and Informatics Preventability (METRIP) coding tool, described below. One pharmacist researcher (GMK) first reviewed the error reports; the results were then reviewed by two family physician researchers (RP and JH). Discrepancies were discussed until consensus was reached. The error reporting studies were approved by institutional review boards at Georgetown University, the University of Missouri-Kansas City, the AAFP, and by individual site institutional review boards as required. Analysis for this study was also approved by the Baylor College of Medicine institutional review board.
Medication error coding
Study investigators reviewed medication error reports and assessed the type, severity and preventability of medication errors using the METRIP coding tool. Data fields of the METRIP coding tool included a research case number, a brief one to two sentence description of the event by the reporter, and 10 coded variables:
error node, identifying the origin of reported errors in the medication management process;
error type;
reason for the error;
harm severity;
person responsible at the error node;
person preventing errors from reaching patient;
medication class;
use of informatics tool (IT)–yes/no;
IT prevention–yes/no;
IT preventability–potential IT features.
All of the coded variables were based on the error descriptions anonymously provided by the reporters. Questions were not directly asked of the reporters related to these items.
Medication error nodes included prescribing, dispensing, administering, monitoring and documenting nodes. Each event report was assigned one error type and one reason for the error. Codes for error types and reasons were derived from taxonomies reported in the literature and continuously revised during the coding process. All the error reports were re-evaluated after the codes were finalised; changes were made according to the final set of codes. The taxonomies we used include selected elements from the USP MEDMARX, the AAFP International Taxonomy of Medical Errors in Primary Care, and the taxonomy developed at the Brigham and Women’s Hospital.4131516 “Reasons for the error” were grouped pertaining to information related to error types. For example, reasons grouped under prescription error type included illegible prescription, insufficient information on the prescription and unprocessed prescription (prescriptions not sent or misplaced). We used the harm severity categories of the US Pharmacopeia National Coordinating Council for Medication Error Reporting and Prevention to code harm.34 If a report described an adverse outcome that was not caused by a medication error, we did not include the event in our study analysis.
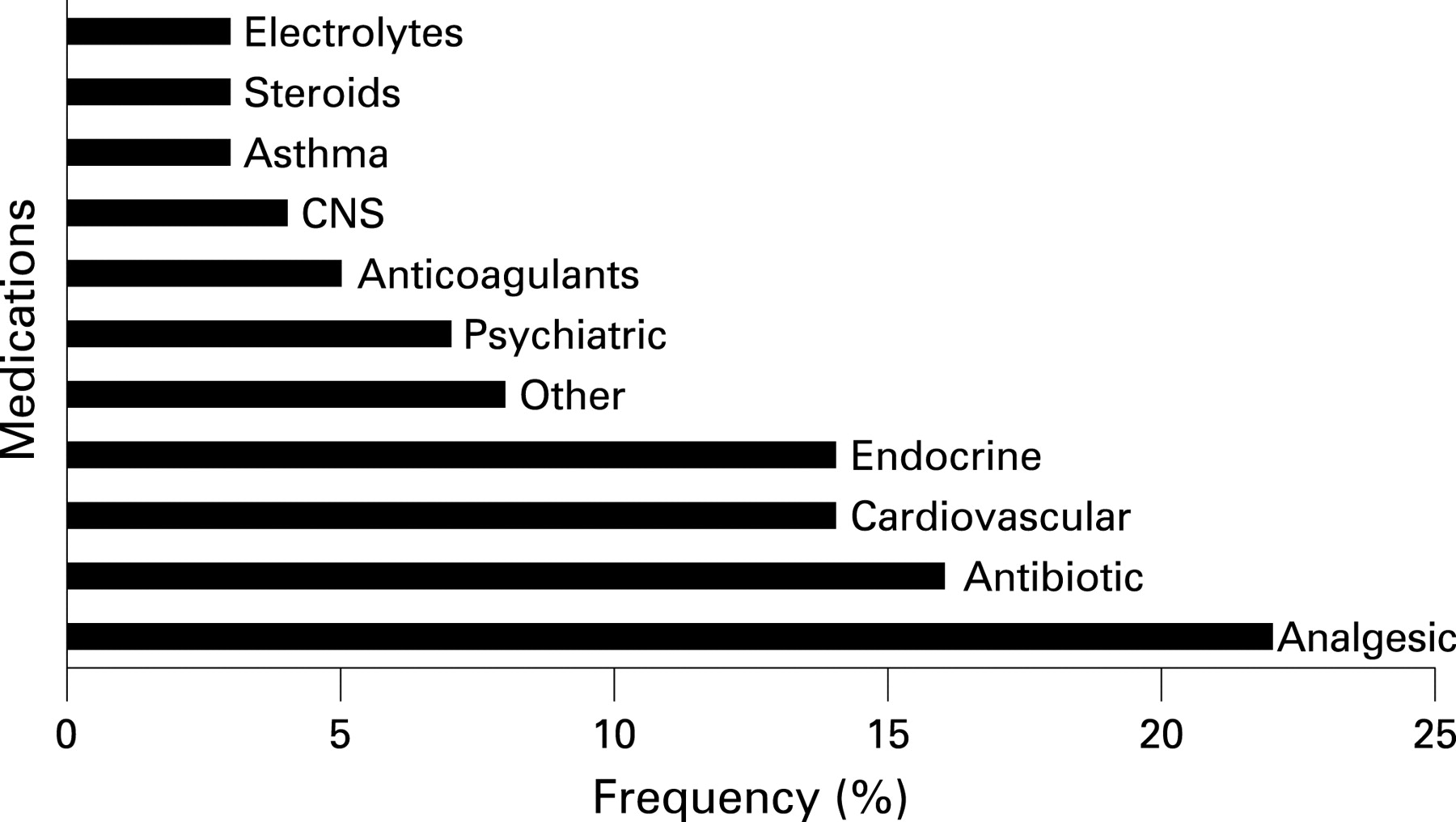
Both the person responsible for the error at the error node and the person preventing the error from reaching the patient were identified as a physician, pharmacist, patient, nurse, caregiver or someone else (eg, clinic staff). Reported medications were grouped into 10 therapeutic classes from the available data: analgesics, antibiotics, anticoagulants, steroids, electrolytes, drugs used for cardiovascular, endocrine, psychiatric and asthmatic disorders, and drugs affecting the central nervous system.
A unique feature of the METRIP coding system is the “Information Technology Preventability” coding. We classified each error according to whether or not existing informatics technology, if fully developed and implemented, would have prevented the error. IT features that could have prevented an error included common functionalities available in most computerised provider order entry (CPOE) systems and electronic medical records (EMR); for example, having a drug selection list, dosage selection, laboratory monitoring, drug allergy or interaction checks, and direct links with pharmacies and other care facilities. The METRIP codes are available from the authors on request or are available online at the AAFP website (http://www.aafp.org/online/en/home/clinical/research/ptsafety/taxonomy.html).
RESULTS
Participants from the two AAFP studies reported a total of 1265 medical errors (330 errors from the first study and 935 from the second study), of which 194 (15%) were coded as errors related to medication errors. Twelve were duplicate reports and four were not medication errors, leaving 178 reports for the analysis.
Origin of errors and severity of harms
The reported medication errors originated from the prescribing (126, 70%), administering (17, 10%), documenting (17, 10%), dispensing (13, 7%), and the monitoring (5, 3%) stage. Overall, 150 (84%) of medication errors resulted in no harm and 28 (16%) in temporary harm (adverse drug events). There were no errors resulting in permanent harm or death. The harm severity levels of reported medication errors are included in table 1. The relationships between harm categories and error nodes are displayed in fig 1.

Medication error types, reasons, and informatics preventability
The two most commonly reported medication errors were related to medication dose and selection, followed by the actual prescription itself and communication issues. Common reasons for these error types included incorrect dose, incorrect drug selection, contraindications, communication problems with pharmacy and insufficient information on the prescription (table 2). No errors associated with route or drug interactions were reported.
We estimated that 57% of the medication errors could have been prevented with currently existing features of EMRs and CPOEs (table 3). Only 3% of the participants reported using information technology in their practice.
Persons responsible for errors and persons preventing errors
The persons who were thought to be primarily responsible for the 178 medication errors reported from clinics in the study were physicians (111, 62%), nurses (19, 11%), other clinic staff (13, 7%), pharmacists (10, 6%), and patients (5, 4%); it was unclear who contributed to 10% of the reported errors. The persons who prevented the 72 errors from reaching patients included pharmacists (29, 40%), physicians (14, 19%), patients (12, 17%), and nurses (2, 7%); it was unclear who prevented 10 (14%) of errors from reaching patients.
Medication classes
Over a third of the reports did not specify medication names or therapeutic classes, and therefore could not be classified. The remaining 118 reported errors were grouped according to their therapeutic classes (fig 2). The most frequently reported medications were analgesics, antibiotics, cardiovascular (eg, drugs used to treat hypertension or hyperlipidaemia) and endocrine medications (eg, oral antidiabetes drugs, insulin, oestrogen/progestogen, levothyroxine).

{kind=link}
{kind=link}
DISCUSSION
Most reported medication errors in our study originated from the prescribing stage. Prescribing errors are the most frequently reported ambulatory medication errors in the published literature.17 Within prescribing, the most commonly reported medication error in our study was related to medication dose. Zhan et al analysed a voluntary medication error reporting database and compared medication errors between CPOE and non-CPOE facilities; they also found that the most common CPOE errors were dosing errors.18 We found that physicians were primarily responsible for committing the reported errors; this is in part due to the prescribing responsibilities of physicians. Also, the study was conducted in primary care clinics and physicians are involved in multiple medication processing stages in this setting. They are notified about problems pertaining to prescribing, dispensing, administering, monitoring and documenting medications. Since physicians were the largest reporting group, they might have reported more errors related to prescribing errors. Even though voluntary reports do not provide the actual frequency of medication errors and adverse drug events, the reported information is useful as a basis for root cause analysis and can be used for identifying error trends as more reporting programmes are implemented in primary care clinics.1
Though most of the reported errors resulted in no harm, we found that a sixth of the medication errors resulted in temporary harm and could be preventable adverse drug events. More than half of the errors reached patients. Pharmacists prevented nearly half of those errors that did not reach patients in our study. Consultation from clinical pharmacists in a collaborative medical team in the hospital setting has been shown to help reduce preventable adverse drug events by 30–78%.19–21 Similar to the inpatient setting, collaboration between physicians and pharmacists might be effective in reducing medication errors in the primary care outpatient setting as suggested by our data. In addition, we found that patients helped to prevent errors in the outpatient setting. For example, they informed their physicians about medications they were allergic to when they were prescribed such medications. Nurses also assisted in medication error prevention. For example, they checked for patient’s medication allergies and clarified medication names and dosages. Methods designed to prevent medication errors and adverse drug events through collaboration among physicians, pharmacists, nurses and patients are warranted in the future to improve medication safety in the outpatient setting. They prevented errors from causing harm, and vigilance by all will probably remain important.
Health informatics tools integrated into the course of primary care delivery would considerably improve medications safety in ambulatory care. Including codes pertaining to informatics preventability in the METRIP tool allowed us to assess the likelihood of error reduction based on the reported information. The informatics features included in the current version of the METRIP tool only included features known to be available today, even though features such as the use of direct linking between clinics and other entities (eg, pharmacy, other clinics, hospitals, nursing homes) is not yet widely used at this time. Since only 3% of the clinics participating in our studies reported using informatics technology, we were not able to make comparisons of errors with and without IT support. Even though some electronic prescribing tools may contribute to errors if not designed or used correctly,22 informatics tools, when paired with a process intervention such as a complete medication reconciliation process, could potentially prevent some, if not almost all, medication errors.23 For example, the Mayo study reported by Nassaralla et al found that EMR and electronic prescribing feature did not improve accurate medication lists until a formal medication reconciliation process was put in place.24
Reporters were not asked to include names of medications. However, the two-thirds of reports mentioning medication names or classes suggest that strategies for future interventions to reduce medication errors in family medicine could be targeted for analgesics, antibiotics, cardiovascular (including antihypertensives) and endocrine (eg, hormones and antidiabetes) medications. Cardiovascular and analgesic agents were also found in a primary care study evaluating prescription clarification by pharmacy calls.25 Future studies of medication errors in primary care may benefit from more explicit naming of medications to understand if there are specific medications within classes that are more prone to error or harm.
A large proportion of errors reported from family physician offices in the USA are medication errors. In the AAFP reporting studies that provided the data for this analysis there was a smaller proportion of medication error reports compared with other ambulatory care studies in the USA. The two-year Applied Strategies for Improving Patient Safety (ASIPS) collaborative study found 35% of reports to be related to medication problems, and a 1-year hospital-based ambulatory care study found 47% of their reported errors involved medications.2627 The lower proportion of medication errors observed in the AAFP studies may be due to the very general definition of error given to the reporters. Clearly, medication errors are among the most frequent types of errors observed in primary care practice.
Our results should be interpreted in the context of several limitations. First, data collected from error reporting programmes do not reflect the actual frequency of medication errors and adverse drug events occurring in the study setting. Our data were based on voluntary reports from clinicians and clinic staff; there were no chart reviews or direct observations to capture all possible errors and adverse drug events. Since the reporting form did not ask for specific type of medication errors, not all errors and events were reported (eg, no drug–drug interactions were reported). Second, the two AAFP reporting studies were conducted in family medicine offices, thus our data do not represent medication errors in other ambulatory care settings. For example, the dispensing errors included in our study were errors found in both clinic and community pharmacies. If the study included only dispensing errors from community pharmacies, the frequency of dispensing errors may be different. Third, physicians in the study may have been more willing to report errors that were prevented before reaching their patients, thus biasing distributions we found in harm categories. Fourth, questions on the reporting form were for general descriptions of error events, not specifically addressing medication events. Over a third of the reports had missing information about medication classes because reporters were not specifically asked to include medication names.
Despite these limitations, our findings showed that most medication errors reported from primary care clinics are related to prescribing errors. In addition, many of these errors reached patients. Our study was conducted in a national practice-based primary care research network including private, teaching, and community clinics located in rural, urban and suburban areas, thus our study findings may more accurately reflect family medicine practice in the USA. Interventions including continuation of error reports using coding tools such as METRIP, involvement of multidisciplinary clinicians and patients, improved medication management process in outpatient clinics, combined with the use of informatics technology are needed to further reduce primary care outpatient medication errors and adverse drug events in the future.
Acknowledgments
The authors wish to acknowledge participants affiliated with the American Academy of Family Physicians National Research Network (AAFP NRN). We appreciate the support from the AAFP NRN and the Robert Graham Policy Center. Dr S Dovey and Dr D Meyers contributed in error coding for both AAFP error-reporting studies. Ms D Cousins from the United States Pharmacopeia (Rockville, Maryland, USA) granted us permission to use the USP MERP Index as one of the reference coding tools for the analysis.
REFERENCES
Footnotes
Funding: We gratefully acknowledge the funding and support from the Agency for Healthcare Research and Quality (AHRQ) to the American Academy of Family Physicians National Research Network (AAFP NRN) and the Robert Graham Center (P20HS11584) and to GMK, (K08HS014552); from the American Academy of Family Physicians to the AAFP NRN and the Robert Graham Center.
Competing interests: The authors declare that they have no potential, perceived, or real competing and/or conflicts of interest.
Ethics approval: The error reporting studies were approved by institutional review boards at Georgetown University, the University of Missouri-Kansas City, the AAFP, and by individual site institutional review boards as required. Analysis for this study was also approved by the Baylor College of Medicine institutional review board.